Article Text

Abstract
Background Denmark and Sweden have implemented reforms that narrowed disability benefit eligibility criteria. Such reforms in combination with increasing work demands create a pincer movement where in particular those with moderate health problems might be unable to comply with work demands, but still not qualify for permanent disability benefits, ending up with temporary means-tested or no benefits. This paper examines whether this actually happened before and after the reforms.
Methods The Survey of Health, Ageing and Retirement in Europe (SHARE) study waves 1–2 and 4–6 in Denmark and Sweden for the age group 50–59 years (N=5384) was used to analyse changes in employment rates and benefits among people with different levels of health before, during and after disability benefit reforms. Interaction between time and health in relation to employment versus permanent or temporary benefits was used as a criterion for whether our hypotheses was confirmed.
Results Overall, employment rates have increased in the age group, but only among the healthy. The OR for receiving temporary or no benefits increased from 1.25 (95% CI: 0.81 to 1.90) before to 1.73 (95% CI: 1.14 to 2.61) after policy reforms for the 29% with moderate health problems and from 2.89 (95% CI: 1.66 to 5.03) to 6.71 (95% CI: 3.94 to 11.42) among the 11% with severe health problems. The interaction between time and health was statistically significant (p<0.001).
Conclusion People with impaired health and workability are forced into a life with temporary means-tested or no benefits when pressed by rising work demands and stricter disability benefit eligibility criteria.
- health policy
- social inequality in health
- social epidemiology
- health reforms
- social security
Statistics from Altmetric.com
Introduction
How to keep older workers in employment
The economic and political sustainability of the Nordic welfare states depends on a high employment rate. This is challenged by demographics with an ageing population, but also — starting five decades ago1 2 — by a tendency among the older workforce to leave the labour market due to ill-health, declining demands for unskilled workers3–5 and reforms in Denmark and Sweden that granted access to early exit from the labour market.6 7
Denmark and Sweden share many policy characteristics of universality and emphasis on social investments including active labour market policies. However, employment policies in the two countries relating to the older workforce differ resulting in a higher employment rate in Sweden compared with Denmark (table 1). In the 1970s and early 1980s, policies designed to make it easier for older workers to leave employment early became widely popular, particularly, in Denmark. However, a political process to reverse the reforms to keep older people in the workforce soon began. From the late 1980s a tendency to reduce generosity of sickness, disability and unemployment benefits was observed in many countries including Denmark and Sweden.8 However, both countries also implemented other policies to keep people in employment through improving work environments, creating subsidised jobs with more flexible demands (flexjobs) and efforts to increase effectiveness of medical and vocational rehabilitation.8–10 In general, the Scandinavian approach to encourage employment has been more successful compared with many other countries.11 12 In the age group 25–54 years, the employment rate has been as high as 85% for both men and women. In comparison, the age group 55–64 years has a significantly lower employment rate though it has been increasing since 2000 (table 1).
Employment rates (%) in the age group 55–64 years in Denmark and Sweden 2000–2015
Main disability reforms since 2000
In recent decades, Denmark and Sweden have both introduced restrictions on eligibility criteria to disability benefits. These restrictions are part of a larger trend of political reforms intended to keep people with health problems in the labour market. In 2003, a disability benefit reform in Denmark focused on creating incentives to remain in employment. However, the lack of increased attachment to the labour market lead to a new reform in 2013, which tightened the eligibility criteria for disability benefits. Thereafter, permanent disability benefits were only granted for people with so little workability that they cannot comply with regular employment or a subsidised flexjob. At the same time the flexjob scheme was expanded to include people with a workability down to a few hours per week.13 14 In 2014, a reform of the sickness insurance benefits was introduced where assessment of the workability was advanced from after 1 year to 5 months of benefits. Claimants evaluated to be at risk of further sickness absence are offered a vocational rehabilitation program.15
In Sweden, similar changes started in the 1990s after a strong increase in spending on sickness and disability benefits in the 1980s. Disability benefits eligibility criteria were limited to only medical criteria without any consideration of local labour market conditions.9 Several organisational efforts have later been introduced to ensure a more strict and efficient practice. In 2005, the assessment of disability benefit claimants was centralised to a single governmental agency with the intention to ensure a uniform treatment of citizens as regional variations in sick leave and disability benefits — that could not be explained by differences in health — had been observed. The 2005 changes were thus more in implementation than actual change of legislation.16 In 2008, the disability benefits eligibility criteria were tightened further. Previously, disability benefits had been granted on a temporary or permanent basis, but from 2008 only people with permanently reduced workability would be eligible. The reform also introduced a ‘rehabilitation chain’, with repeated assessments of workability at fixed time intervals. Furthermore, the reform limited the benefit period to 1 year though it is possible to apply for an extension, which implies it is possible to receive sickness benefits up to 2,5 years before a person would enter the unemployment benefits system and the introductory programme at the job centres.6 In 2015, a further centralisation was done of the assessment of disability claims, which has resulted in a rejection rate of 70% per cent of claims.17 The value of benefit levels have gradually been lowered in both countries15 and overall policies have moved from a focus on economic security and vocational rehabilitation to a focus on economic incentives to work16 and stricter disability benefits eligibility criteria.
Reforms in a labour market context
The implementation of the political initiatives described above has taken place in a context where work demands may have increased on the labour market. Though changes in self-reported physical and psychosocial demands have been surprisingly small according to Eurofound-data for 2005–15 rising mental demands in public services like health and education have been observed.18 These findings have been partly confirmed by national surveys in Denmark and Sweden.19 20 In Sweden, it has been found that, in general, job strain (high mental demands combined with low decision latitude) has increased in the workforce, especially, among women. This is partly a consequence of the service sector expansion, but most of the rise in strain has taken place within job categories, primarily in welfare services such as care and education.20
Taken together, the context described above shows that people with health problems and functional limitations could be facing a pincer movement where on the one hand they are facing high and rising work demands which might make even people with moderate health limitations unable to cope on the labour market and, at the same time, eligibility criteria for disability benefits are tightened. In particular, people with mental health problems might be vulnerable since the psychological and social demands at work are rising in some sectors, and at the same time stricter medical criteria for disability pension may have a stronger impact on those with mental health problems where diagnostic criteria are less clear.21 22
A systematic review of changes to eligibility criteria for disability related benefits covering Norway, Sweden, the UK and Canada found that such changes generally shifted people onto other benefit schemes such as unemployment benefits and did not lead to more people entering employment.23 A recent Danish study showed that people on temporary means tested welfare benefits have experienced a rise in the prevalence of common mental disorders.21 Similar findings have been made in Sweden.24 Further analysis indicates that this was generated both by an increase of people with mental health problems leaving the labour market, and by an increase in people with health problems moving into means tested welfare benefits,21 potentially because they were not sick enough to qualify for a disability pension. A study from the UK found that reassessment of existing disability claimants against tighter criteria for disability benefits did not increase employment chances of people with a longstanding illness outside the labour market.25
In this study, we aim to analyse how the employment situation changes for people with health problems with different levels of severity in the context of recent disability benefit reforms. We hypothesise that when eligibility criteria are tightened or enforced more strictly those with moderate health problems are pushed into means-tested and temporary benefits, while the employment of those in good health is not affected and those with severe health problems would still qualify for disability benefits.
Material and methods
Study population
The study is based on repeated cross-sectional data from the Survey of Health, Ageing and Retirement in Europe (SHARE).26 SHARE is a bi-annual survey based on a random sample that collects data on health, socioeconomic variables and social networks in individuals above 50 years and their partners. In this study, we used data collected in Denmark and Sweden in 2004–2015 with waves 1, 2, 4, 5 and 6.27–31 Individuals were selected if they were between 50 and 59 years at the time of the interview in order to avoid influence by early retirement reforms applying to those older than 60 years. The total sample consists of 5384 observations based on individuals in the age interval 50–59 years from Denmark or Sweden. The sample consisted of 3242 individuals out of which 1585 individuals (48.9%) contributed with a single observation, 1172 (36.2%) contributed with two observations and 485 (15.0%) participated with observations in three different waves.
Health score
We constructed a health score based on three variables assessing health and functional limitations. The included variables cover mental health status, pain and functional limitations. As mental health conditions and musculoskeletal pain are some of the most important drivers of disability benefits in Denmark and Sweden in the age group of the current study,32 33 we wanted to apply a score that included these conditions in addition to the measure of functional limitations.
Mental health status was based on Euro-D scale, which was developed to compare symptoms of depression across European countries. The scale covers the following 12 symptoms: depression, pessimism, suicidality, guilt, sleep, interest, irritability, appetite, fatigue, concentration, enjoyment, tearfulness.34 35 We categorised responses in three levels: 0–1 symptoms, 2–3 symptoms and ≥4 symptoms.
Functional limitations was measured by use of the Global Activity Limitations Index (GALI). The question for GALI asks ‘For the past six months at least, to what extent have you been limited because of a health problem in activities people usually do’. The three response categories were no limitations, limited but not severely and severely limited.
The pain variable was constructed differently in the two time periods owing to the lack of a consistent measure throughout all the waves in the SHARE study. In the first time period from 2004 to 2010 (waves 1, 2 and 4) the pain variable was constructed by a combination of questions on joint pain and the use of medication. In the second time period from 2010 to 2015 (waves 4–6) the pain variable was harmonised across the waves. In wave 4, the pain variable was based on the pain and discomfort domain of the EQ-5D. In waves 5 and 6, it was based on a question of severity of pain. The harmonised response categories across all waves were: no pain, moderate pain and severe pain.
Our health score combines the three dimensions on mental health, functional limitations and pain on a five-point scale. The final health score was categorised into three levels due to power reasons: good health (score 1), moderate health problems (score 2+3) and severe health problems (score 4+5) (see online technical appendix).
Supplemental material
Timing of the implementation of reforms
The implementation of the disability reforms mainly took place after 2005 and 2008 in Sweden and after 2013 in Denmark. Therefore, our time measurements of before and after the reforms involves different calendar periods in the two countries. The time period includes three measurement times for each of the two countries, but due to a very small sample size in Sweden — with insufficient statistical power for a separate country analysis — the measurements from Denmark and Sweden are combined in our analysis. Hence, we combined the data for both countries into the following three time periods: the first time period includes data before the recent reforms (wave 1 (2004) in Sweden and wave 4 (2011) in Denmark), the second time period includes data from around the early stages of implementation of the reforms (wave 2 (2007) in Sweden and wave 5 (2013) in Denmark), whereas the third period includes data from later stages of implementation of the reforms (wave 4 (2011) in Sweden and wave 6 (2015) in Denmark).
Outcome: employment status
Employment data was collected with a question on the interviewed individual’s current job situation. The response categories covered retired, employed or self-employed (presumably including people on sick leave or flexjobs), unemployed, permanently sick or disabled, home maker or other. We classified the responses in three groups: the individuals that answered that they were ‘employed’ or ‘self-employed’ were classified as being employed, individuals who reported they were ‘retired’ or ‘permanently sick or disabled’ were classified in the group disability benefits, and individuals that stated they were ‘unemployed’, ‘home maker’ or ‘other’ were classified as being on temporary or no benefits.
Statistical analysis
The analysis was based on multinomial logistic regression. Three outcome levels were used: employed, temporary/no benefit and disability pension. The health score, time period and the covariates age, gender and country were all modelled as categorical variables. An interaction term between time period and health score was included to assess our hypothesis of whether the effect of the health score on employment has changed during the implementation of the reforms restricting eligibility criteria for disability benefits. Age, gender and country were included as confounders.
Results
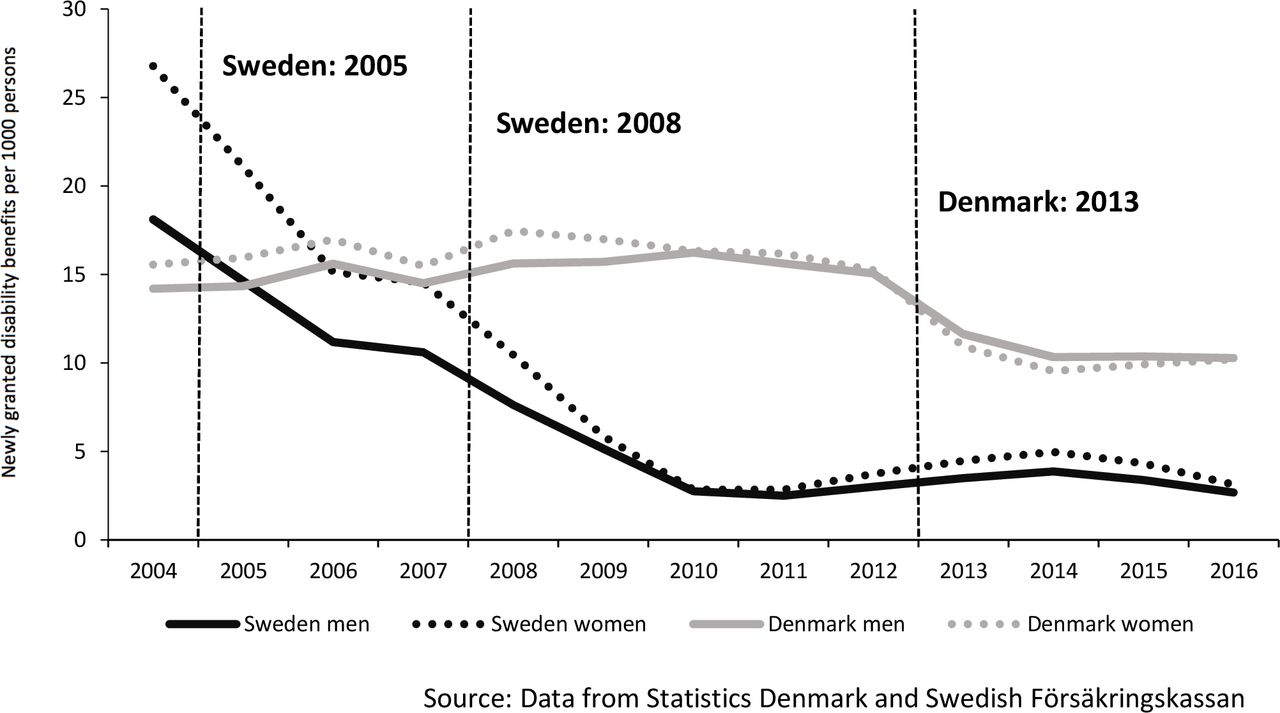
Figure 1 shows the rate of newly granted disability benefits per 1000 people in Denmark and Sweden from 2004 to 2016. The graphs show a marked drop in newly granted disability benefits in both Denmark and Sweden, but the drop happens markedly earlier in Sweden than in Denmark in line with the timing of the reforms in the two countries.

{kind=link}
Newly granted disability benefits per 1000 persons in the age 50–59 years in Denmark and Sweden from 2004–2016.
Our total sample of 5384 observations is based on waves 1, 2 and 4 for Sweden and waves 4, 5 and 6 for Denmark. Just over half of the individuals in our total sample were women (55.9%). In our sample, 60.2% had good health, 28.7% had moderate health problems and 11.2% had severe health problems. The majority were employed (83.7%), whereas 6.6% were on temporary or no benefits, and 9.7% on disability benefits (data not shown). Table 2 shows numbers and proportions in the different employment and benefit categories across years and health scores. Not all years are included for both countries since the pain-component of the health variable is not directly comparable across the years, and those years are not needed for the analysis. In 2011, which is the only overlapping year, the employment rates were higher in Sweden than in Denmark across all levels of health status, but markedly higher for people with moderate health problems (87.1% in Sweden compared with 78.9% in Denmark) and with severe health problems (52.8% in Sweden compared with 42.6% in Denmark).
The numbers and proportion (%) employed, on disability pension and other benefits according to disability level in the age group 50–59 years in Denmark and Sweden 2004–2015
Table 3 shows the OR of being on temporary or no benefits or on disability benefits over time compared with the reference group who is employed and in good health before the implementation of the disability reforms. The OR for being on temporary or no benefits decreases for those in good health, which corresponds to the overall increase in employment found in table 1. For those with moderate health problems the OR show an increasing tendency from 1.25 (95% CI: 0.81 to 1.90) before the reforms to 2.05 (95% CI: 1.41 to 2.98) in the early phases of implementation and 1.73 (95% CI: 1.14 to 2.61) in the following years. For those with severe health problems, we also see an increase in OR for being on temporary or no benefits. The OR for being on permanent disability benefits show wider confidence intervals, but seems to decline after reforms among those in good health, and for those with moderate health problems. For those with more severe health problems there was no change. Overall, the development over time of employment versus benefits differs between the health levels and the interaction between timing of the reforms and health is statistically significant (p<0.001).
Trends in ORs for being on temporary/no benefits or on disability benefits by health score during the implementation of disability reforms
Discussion
In summary, our analysis shows that for the large group in good health (60%), the odds of receiving disability benefits or being out of work with no or temporary benefit is considerably reduced after the reforms and the employment rates correspondingly increased. Our hypothesis that those with moderate health problems would neither be employed or on disability benefits due to increasing job demands and stricter eligibility criteria was also partially supported by the analysis. For the 11% with more severe health problems, the chance of getting a permanent disability benefit is relatively unchanged, but the risk of ending up without any or a temporary benefit might have increased after the reforms.
The fact that more people with less severe or temporary health problems are working might be an effect of many ongoing secular trends and labour market policies including the disability reforms. The sum of those developments show up in the overall increasing employment rates shown in table 1. Our study indicates that not only the groups with moderate health problems, but also the group with severe health problems increasingly are on no or temporary benefits, and that might be a sign of the pervasiveness of the disability reforms. The disability benefit reforms seems to have pushed people with both moderate and severe health problems into a life exposed to the economic stress living with no or temporary and means-tested benefits.
The policy implication is that this approach to disability reforms may have contributed to keep some people with less severe or temporary health problems at work but people with health problems, who have difficulties to comply with demands of modern labour markets have been pushed out to temporary or no benefits. For the latter group, jobs with reduced and more flexible work demands (flexjobs) are more important than ever, if they shall not be pushed out into economic adversities that might further aggravate their health problems. As shown in figure 1, the rate of disability benefits has particularly in Sweden declined gradually and not with any clear changes linked to the timing of reforms. That indicates that our conclusion are less related to specific reforms, but rather gradual changes in implementation and practice of the authorities.
The study is based on SHARE data of well-documented quality, comparable across waves and countries. A limitation of the study is that we were not able to account for the dependency between observations for individuals participating in more than one wave in the multinomial logistic regression models. However, the effect of repeated measurements was tested in a simpler model with a binary outcome and that only had marginal effect on the OR estimates and the overall pattern was similar in the two models (data not shown). Another limitation of the study is that we make use of a health score which is not validated to be able to include the dimensions on mental health status and pain. However, we have carried out a sensitivity analysis based on the GALI which is a simpler disability measure than the one we applied in our analysis. The analysis based on GALI showed a very similar pattern to the health score in our study (data not shown). Some misclassification may have taken place in the survey data in relation to our study. It is possible that a fraction of those who replied they are ‘permanently sick or disabled’ may not receive disability benefits which is how we have classified this question in our outcome variable. However, if they should have been placed in the category of temporary or no benefits it would imply that we have underestimated the effect of the reforms on the odds of being on temporary or no benefits. Furthermore, since we look at trends it is of less importance as the misclassification is not likely to change over the investigated time period. Finally, our results were limited by the small sample size in Sweden which implied that we were not able to carry out the analysis separately for the two countries, but had to merge the samples across different measurement years. The employment rates found in the SHARE sample are generally higher than what is found in the data from the Organisation for Economic Co-operation and Development (OECD) in table 1. That could indicate a selection bias with more non-responders among the not employed.36 The differences between Denmark and Sweden are similar to OECD data but the time trends indicate that this selection bias might increase over time.
What is already known on this subject
Labour market reforms including stricter disability pension eligibility criteria focused on increasing employment rates among the older labour force have succeeded. At the same time, productivity and work demands has increased to an extent that might make it difficult for people with reduced health to comply.
What this study adds
The combined effect of labour market policies including stricter disability benefits eligibility criteria and higher work demands has increased the employment rate among the healthy 60%, while the 40% with moderate and severe health problems are increasingly pushed into temporary means tested or no benefits.
Acknowledgments
This paper uses data from SHARE Waves 1, 2, 3 (SHARELIFE), 4, 5 and 6 (DOIs: 10.6103/SHARE.w1.611, 10.6103/SHARE.w2.611, 10.6103/SHARE.w3.611, 10.6103/SHARE.w4.611, 10.6103/SHARE.w5.611, 10.6103/SHARE.w6.611), see Börsch-Supan et al. (2013) for methodological details. The SHARE data collection has primarily been funded by the European Commission through the 5th Framework Programme (project QLK6-CT-2001-00360 in the thematic programme Quality of Life), through the 6th Framework Programme (projects SHARE-I3, RII-CT-2006 -062193, COMPARE, CIT5- CT-2005-028857, and SHARELIFE, CIT4-CT-2006-028812) and through the 7th Framework Programme (SHARE-PREP, N° 211909, SHARE-LEAP, N° 227822 and SHARE M4, N° 261982). See www.share-project.org for a full list of funding institutions. In addition, we would like to thank Professor Per Kragh Andersen, Section for Biostastics, Department of Public Health, University of Copenhagen assisted in the analysis.
References
Footnotes
Contributors NKJ, HBH, IA and FD designed the study. NKJ and HBH made the analysis. NKJ and FD drafted the first version of the manuscript. KT, AM, BBu, BBa, MW contributed to the interpretation of the results. All authors provided comments on earlier versions of the manuscript. All authors read and approved the final manuscript.
Funding The study is part of a larger project entitled Tackling Health Inequalities and Extending Working Lives (THRIVE). The funders were The Innovation Fund Denmark (5194-00004B), the Swedish Research for Health, Working Life and Welfare (2015-01531),The UK Economic and Social Research Council (ES/N019261/1) and was also supported by The Joint Programme Initiative More Years, Better Lives.
Disclaimer The funding agency had no role in design or analysis of the study. The views expressed in this paper are those of the authors and not necessarily of the funding agency.
Competing interests None declared.
Patient consent for publication Not required.
Ethics approval The Danish team do not need ethical approval to use the SHARE data as ethics approval is only required when using biological materials. For Swedish data, the Swedish team received ethical approval to use the SHARE data from the Regional Ethical Review Board of Stockholm (Dnr 2016/1353-31/5) Additionally, the SHARE project is submitted to continuous ethics reviews. From wave 4 and onwards SHARE has received ethical approval from the Ethics Council of the Max Planck Society. The last ethics approval was granted on 4 March 2016 (http://www.share-project.org/organisation/dates-facts.html).
Provenance and peer review Not commissioned; externally peer reviewed.