Article Text

Abstract
Background The WHO International Classification of Functioning, Disability and Health (ICF) is now the dominant model for exploring the social consequences of a health condition. This paper investigates the association of the different ICF disability domains with mortality.
Methods Data are from the British Women Heart and Health Study, a large (n=4157) prospectively studied cohort of women randomly selected from 23 towns aged 64–83 years in 2003. Scores were calculated to describe the cumulative load of impairments, limitations and restrictions within each ICF domain. Cox proportional hazards regression was used to calculate mortality HRs per unit score increase within each ICF domain. Adjustments were made for age, town, living status, socioeconomic status, lifestyle behaviours and health conditions.
Results Each ICF domain was associated with mortality after controlling for lifestyle factors and health conditions. However, only complex activities (HR=1.09, 95% CI 1.01 to 1.18) and participation (HR=1.10, 95% CI 1.04 to 1.16) were independent predictors of mortality following adjustment for all other disability domains and potential confounders.
Conclusions Results suggest that difficulties with complex activities or social participation could be used to identify and target women at high risk of dying. Interventions to facilitate complex activities or improve social participation may help to delay mortality in elderly women.
- Disability
- mortality
- elderly
- social participation
- WHO-ICF
- epidemiology
- addictive behaviour/addiction
- ageing
- alcohol
- heart disease
- genetic epidemiology
- developing country
- coronary heart disease
- stroke
Statistics from Altmetric.com
- Disability
- mortality
- elderly
- social participation
- WHO-ICF
- epidemiology
- addictive behaviour/addiction
- ageing
- alcohol
- heart disease
- genetic epidemiology
- developing country
- coronary heart disease
- stroke
Introduction
Projections suggest that the proportion of the population aged above 65 years will increase from 16% of the population in 2008 to 23% by 2030.1 Assuming no improvement in age-specific disability rates, the number of older disabled people in the UK is projected to increase by 40% between 2002 and 2022.2 An alternative scenario is that extra years of life could be lived in better health with morbidity and disability postponed to ever-older ages—the compression of morbidity theory.3 Indeed, recent UK government policy has been consistently targeted at helping people to live longer and to live more healthily.4–6 A third ‘steady-state’ scenario is that both the number of years lived in good health and the number of years lived with disability will increase.7
It currently remains unclear which scenario is most probable.8 In the USA, some evidence supports the compression of morbidity theory.9 UK statistics suggest that recent improvements in life expectancy at age 65 have not been matched by improvements in disability-free life expectancy.10 Other evidence suggests that more recent UK cohorts may have a higher level of disability, contrasting with declining trends in other countries.11 12 Severity of disability may also influence evidence supporting the different scenarios. For example, in England and Wales, increasing prevalence of limiting longstanding illness may be due to an increase in more minor problems while the prevalence of the most severe disabilities is declining.13 Hence, a better understanding of the implications of different conceptualisations of disability for mortality is needed.
The medical model of disability attributes limitations in activity and participation solely to various physical conditions. In contrast, the social model of disability recognises that these are the product both of the individual's physical capacity and the environment they inhabit.14 The social model is incorporated into the WHO's International Classification of Functioning, Disability and Health (ICF) (figure 1), now the dominant model for exploring the consequences of a health condition on disability.15 16 According to the ICF, disability is described as functioning according to three domains: impairments, activities and participation. Impairment relates to pathological body function and structural changes (eg, visual impairment), activities describe the capacity of a person to carry out basic (eg, drinking from a cup) and complex tasks (eg, preparing a hot meal), while participation refers to the extent of involvement in life situations (eg, going on outings). These three domains are placed within the context of environment and personal factors.

The International Classification of Functioning, Disability and Health (ICF). Source: World Health Organization Geneva 2002, ‘Towards a Common Language for Functioning, Disability and Health: ICF’.
In epidemiological studies of the effects of disability on mortality, many studies of isolated aspects of functioning have been undertaken, often limited to walking or activities of daily living.17–19 Thus, the majority of studies to date relate to what would be classed as impairments or activities according to ICF. However, a large meta-analysis has recently highlighted the importance of social relationships for survival, with effects comparable in size to established risk factors (smoking, alcohol, physical inactivity).20 To our knowledge, no study has attempted to explicitly contrast the effect of different ICF domains of disability on mortality. Existing studies are also diverse with respect to populations (nationality, community based, in-patients, gender), with the study of disability in older women particularly under-represented.
We examined the association between disability and mortality to gain a better understanding of the optimal targets for health and social care interventions to reduce mortality in older people. The independent effects of disability domains defined according to the ICF on all-cause mortality were compared using data from a large nationally representative cohort of older women.
Methods
Study design
The British Women's Heart and Health Study (BWHHS) is a prospective cohort of elderly women recruited in 1999 from General Practitioner (GP) practices in 23 towns across England, Scotland and Wales. Women aged 60–79 years were selected at random from GP registers in these towns. Four thousand two hundred and eighty-six of the women originally invited agreed to participate in the study, corresponding to a response rate of 59%. There have been two subsequent follow-ups of the BWHHS in 2003 and 2007 (with a further follow-up in progress). In this study, the 2003 wave was taken as baseline since disability was much more comprehensively measured at this follow-up. Of the 4286 women recruited in 1999, data for 4132 women (96%) were available in 2003. Ethics approval for the BWHHS has been granted by the 23 Local Research Ethics Committees for the study population and the London School of Hygiene & Tropical Medicine Ethics Committee. All women gave signed informed consent at baseline.
Outcome
Women were prospectively followed until February 2010 with deaths recorded via the NHS Central Registry. Six hundred and fifty-three deaths were recorded during the 7-year period of follow-up, with the number of deaths per year shown in table 1. The proportion of women who died during follow-up was 0.158.
Survival status by year
Exposure variables
All variables in the 2003 wave of BWHHS were assessed for inclusion in the ICF framework. This process resulted in the identification of 40 variables: 8 impairments, 24 activities and 8 participations (online appendix A). These included variables from the EQ-5D, Nottingham Health Profile Part II, activities of daily living and instrumental activities of daily living.21–23 The authors (CD and HK) consulted the ICF browser to provide objective classification of the variables into the different ICF domains of health conditions, impairments, activities or participation.24
The ICF browser distinguishes impairments from activities and participation but does not clearly distinguish between activities and participation.24 Independent external expert opinion was sought for any items where uncertainty remained. Activities were further subdivided into basic and complex activities. Basic activities were defined as simple actions to accomplish a task (eg, bending down) and complex activities as those involving several faculties and cognition (eg, preparing a hot meal). Using this definition, the authors (CD and HK) classified the 24 activities into 16 basic and 8 complex activities (online appendix A). No item was assigned to more than one ICF domain.
Health conditions were categorised into two groups depending on whether they related to cardiovascular disease or not. Cardiovascular health conditions included heart attack, heart failure, angina, stroke, deep vein thrombosis, claudication, pulmonary embolism, diabetes and aortic aneurysm. Non-cardiovascular health conditions included cancer, asthma, bronchitis, gastric, peptic or duodenal ulcer, gout, gall bladder disease, osteoporosis, arthritis, cataract and glaucoma. The cumulative load of adverse conditions within each group was summed.
The cumulative number of adverse lifestyle factors was also summed. Lifestyle factors included smoking (1=current smoker), drinking alcohol (1=most days), healthy diet (1=fruit and vegetables less often than four or five times per day) and physical inactivity (1=less than 2 h moderate or vigorous activity per week).
Scores were calculated to express the cumulative load of disabilities within each ICF domain (impairments, activities, participation) and also for health conditions and lifestyle factors. All variables were binary (0/1) coded such that 1=adverse. To account for missing data, participants were assigned a score based on the proportion of adverse endorsements to the number of questions answered in the domain. The proportion was subsequently rescaled from 0 to 10 (online appendix B), so 1 point of the score reflects a 10% increase in the proportion of endorsement. In all domains, a higher score indicates a greater adverse load.
There are a number of potential confounders of the disability–mortality association, including age, marital status, social support and socioeconomic status (SES).25–31 Hence, age (10 categories), town (23 towns), living status (living alone or with other people) and SES were considered to be potential confounders. SES was measured as a continuous score of life-course adversity where a higher score indicates more adverse events.32 Living status was included as a succinct measure of both marital status and social support.
Statistical analyses
A hypothetical framework of the association of ICF domains plus health conditions and lifestyle factors with mortality was used to inform the statistical modelling (figure 2). The independent association of each ICF domain with mortality was estimated and subsequently adjusted for confounders, lifestyle factors, health conditions and other ICF domains. Adjustments were made according to the following sequence:
Model 0: Crude association.
Model 1: Adjusted for potential confounders only.
Model 2: Adjusted for potential confounders, lifestyle factors, health conditions and prior ICF domains.
Model 3: Adjusted for potential confounders, lifestyle factors health conditions and subsequent ICF domains (but not for prior domains).
Model 4: Simultaneous adjustment for potential confounders, lifestyle factors, health conditions and all other ICF domains.
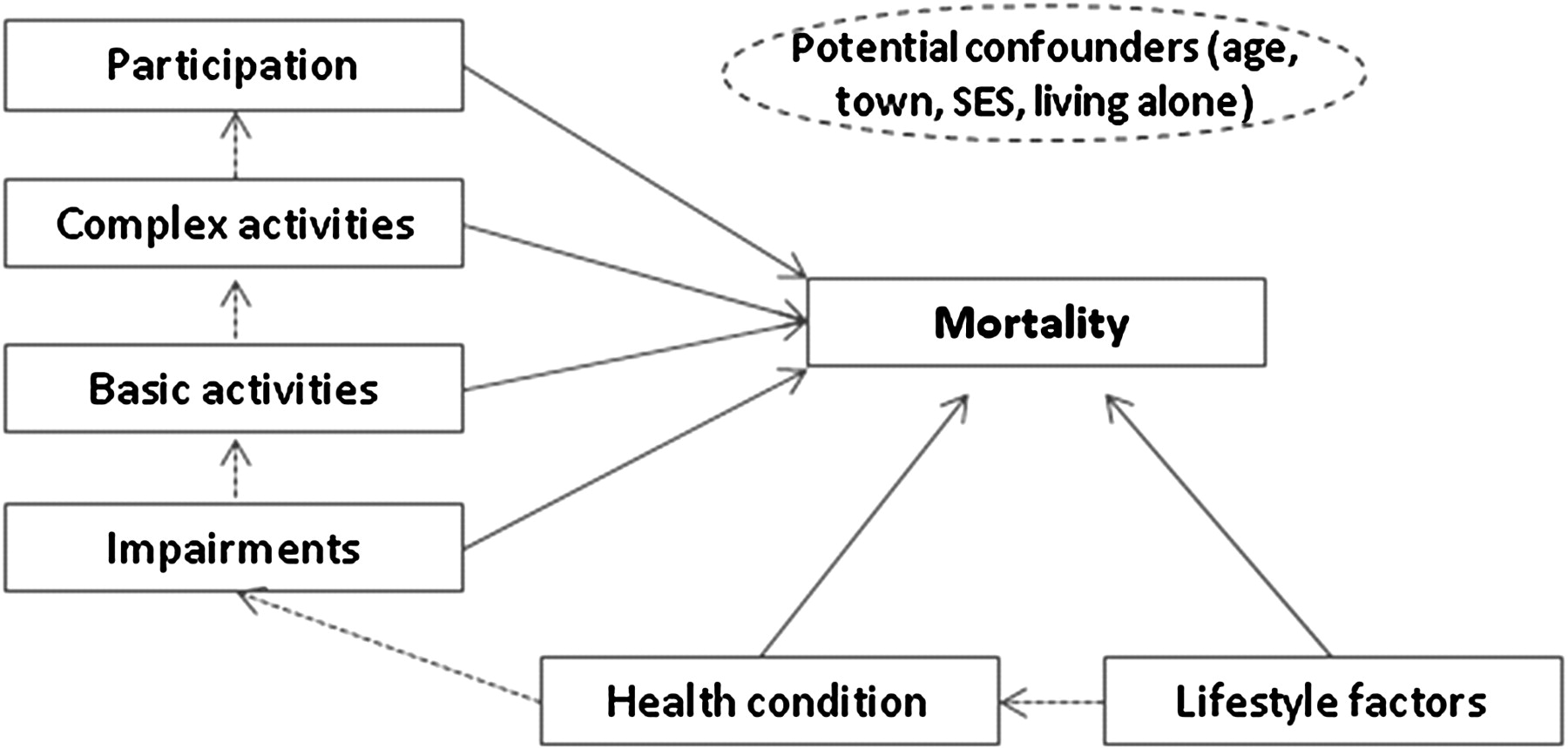
Hypothetical conceptual framework for the association of lifestyle factors, comorbidities and domains of disability with mortality. SES, socioeconomic status.
In each of the models above, Cox proportional hazards regression was used to calculate the increase in mortality HR per unit of disability score within each domain. HRs therefore represent the increased mortality hazard per 10% increase in the proportion of endorsements within a domain.
Results
The response profile for each disability domain, lifestyle factors, health conditions and confounders is described in table 2 according to mortality status at end of follow-up. Response to impairments, activities, participation, SES and living alone was lower than other variables in both follow-up categories. Baseline response rates were consistently higher in women who were alive at the end of follow-up compared with those who died during follow-up. These differences in response by mortality status were especially marked for impairments, activities, participation and living status. Mean scores were consistently higher among those who subsequently died for all domains and confounding variables, indicating higher adverse load in those who died.
Baseline response profile and mean scores by alive or dead status at follow-up
Histograms (online appendix C) illustrate score frequency within each domain and the trend in the probability of dying with 95% CIs by score. There was a consistent trend for higher probability of dying with increasing disability score, with similar trends for lifestyle factors and health conditions.
Figure 3 illustrates the increase in mortality hazard per unit increase in disability domain score. Unadjusted HRs (models 0; figure 3) were similar in all disability domains ranging from 1.17 (95% CI 1.14 to 1.20) for basic activities to 1.21 (95% CI 1.18 to 1.24) for complex activities. Compared with unadjusted models, adjustment for demographic confounders (models 1; figure 3) attenuated the effect for all disability domains, but all HRs remained above one. The 95% CIs for models adjusted for age, town, living status and SES (model 1) overlap with those for the unadjusted model (model 0) in all disability domains.

Mortality HRs per unit of disability domain score, with cumulative adjustment.
Further adjustment for lifestyle factors, health conditions and prior disability domains in model 2 led to attenuation of the mortality effect in all domains (figure 3), but again all effects remained above one (figure 3). For example, after adjustment for potential confounders, lifestyle factors and health conditions mortality hazard increased by 1.08 (95% CI 1.03 to 1.13) per unit increase in impairment score.
However, impairments were no longer associated with elevated mortality after adjusting for basic and complex activities and participation (model 3; HR=0.97, 95% CI 0.91 to 1.03). Similarly, basic activities were also no longer associated with mortality after adjusting for complex activities and participation (model 3; figure 3) or all domains and confounders (model 4; figure 3).
Conversely, complex activities remained a predictor of elevated mortality after adjustment for participation (model 3; HR=1.08, 95% CI 1.02 to 1.15) and for all domains and confounders (model 4; HR=1.09, 95% CI 1.01 to 1.18). Participation also remained an independent predictor of mortality following adjustment for all dimensions and confounders (model 4; HR=1.10, 95% CI 1.04 to 1.16).
Sensitivity analyses
Evidence suggests that non-responders to surveys are more likely to be in ill health.33 34 Therefore, models were re-estimated adopting a more extreme scenario whereby all missing data were assumed to be adverse in the construction of domain scores. The same pattern of association with mortality with sequential adjustments was observed (figure 4). This suggests that it is unlikely that the relative effect of the disability domains on mortality is explained by differential missing data in the domain scores. Under the extreme missing data scenario, there is weaker evidence for difference in the hazard of dying per unit increase in participation score (model 4; figure 4), while under the original missing data scenario, there was weaker evidence per unit increase in complex activities score (model 4; figure 3).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Mortality HRs per unit of disability domain score, with cumulative adjustment (assuming missing data are all adverse).
In further sensitivity analyses, health conditions were entered separately into the models rather than as a cumulative domain score. This led to more imprecise estimates resulting from the loss of sample size but no substantive change in results compared with the models using the domain scores for health conditions.
Discussion
This study provides evidence that all ICF disability domains are independent predictors of mortality after controlling for lifestyle factors and health conditions in a nationally representative sample of British women. However, after mutual adjustment for other disability domains, health conditions and lifestyle factors, only complex activities and participation are independent predictors of mortality. Thus, the ICF disability domains most closely association with death have been pinpointed as social participation and complex activities. At face value, these findings are consistent with the social model of disability, suggesting that, at least in terms of mortality, the ability of a woman to perform complex activities or participate in her social environment may be more important than her biological impairments or basic activities limitations.
The independent effect of participation on mortality is consistent with a previous finding of social engagement on cardiovascular mortality in British men (HR 0.70, 95% CI 0.53 to 0.93).35 Similarly, a HR=0.87 (95% CI 0.77 to 0.88) for social activities was found in a population of elderly people living in East London or Essex. By comparison, the strength of association in the current study is relatively modest at approximately a 10% increase in the hazard of death per unit increase in participation (or complex activities) score. However, direct comparison of effect sizes across studies is hindered by the use of different survey instruments and methods in different studies. This impact of measurement has been highlighted in a recent meta-analysis, where stronger effects were found with multidimensional assessments of social integration such as the one in the current study.20 This meta-analysis found an OR=1.91 (95% CI 1.63 to 2.23) for survival with complex measures of social integration.20 However, estimates with the least statistical control for confounding and the greatest level of contrast were meta-analysed, both likely to reveal stronger effects compared with methods applied in the current study.20 Furthermore, effect sizes in the current study relate to a per unit increase in ICF domain score, in other words the additional mortality risk associated with the addition of a single extra limitation or restriction. This compares with the Ramsay et al35 study using a nine item scale where HRs compared risk in those scoring 8–9 versus 0–3.
Low social engagement was also associated with higher mortality after controlling for physical health in a small Nottingham city sample.36 In a Dublin city sample, higher social engagement has been associated with enhanced mental and physical health, cognition and quality of life.37 Internationally, loneliness has been associated with higher mortality risk in a Finnish population sample38; while the less socially engaged were found to be less healthy in a large Dutch community sample.39 Strong cross-sectional association between social participation and disability were also found in a US community sample, but there was no evidence that participation was protective against functional decline, suggesting that findings may be more consistent with reciprocal causation, that is, functional decline causes lower participation levels.40
Our finding with respect to complex activities replicates the established evidence for an association between activities of daily living or instrumental activities of daily living and mortality.41–43 However, an interesting finding in the current study is that evidence for an independent association was limited to ‘complex’ activities, while ‘basic’ activities were not found to have an independent association with mortality.
Measurement issues
‘Reverse causality’ can arise through the presence of morbidities contributing to both future mortality and disability at baseline measurement. While confounding by health conditions was controlled for in the analyses, it is possible that this control was incomplete due to measurement error in the diagnosis of health conditions. Furthermore, despite the rich phenotyping available in the BWHHS, it was still only possible to control for a limited number of conditions and lifestyle behaviours. In addition, health conditions and lifestyle behaviours were modelled as binary variables, and therefore, potentially important variability in the severity of these conditions was not accounted for. Indeed, it is quite possible that the disability domains studied were acting as proxies for severity of health conditions.
The BWHHS questionnaire was not designed to assess the ICF and hence coverage of some domains may be incomplete. Impairments in particular were measured through self-report only and may be under-represented. Another measurement problem relates to the potential correlation between ICF domains. For example, locomotor activity limitation has previously been shown to be strongly associated with reduced participation in the BWHHS.25 Attempts have been made to identify measures of impairment, activity and participation uncontaminated by other ICF domains for particular health outcomes, such as the Aberdeen IAP for joint replacement surgery.44 It is likely that some items included in the current study may not purely measure the domain in question, thereby leading to misclassification bias and potential underestimation of domain effects.
Another potential limitation stems from partial questionnaire completion resulting in missing data in the disability domains. A lower level of response was found among those who subsequently died compared with those who were alive at the end of follow-up. It is likely that non-responders may have had a higher disability load as well as being more likely to die, and therefore, complete case estimates of the association between disability and death will be conservative. However, in sensitivity analyses, results were found to be robust to the more extreme missing data scenario where all missing disability data were modelled as adverse.
The BWHHS is a prospective cohort of elderly women in Great Britain; therefore, results may not be generalisable to other populations with different disability or mortality profiles.
Implications of a social participation focus
For the association between social participation and mortality to be considered causal, identification of a biologically plausible pathway would be required. It has been argued that a direct pathway may exist through physiological changes to the cardiovascular, hormonal and immunological systems.45 Social support has been linked to favourable inflammatory profiles in men,46 47 as well as to enhanced immune response and increased resistance to upper respiratory illness.48 49 An indirect pathway may operate through encouraging healthier lifestyle behaviours, such as improved diet and greater physical activity. Yet lifestyle factors were controlled for in the current study, albeit imperfectly. Furthermore, social activities that have little physical fitness benefit have also been shown to be associated with survival benefits.50 Another possible pathway is via psychosocial benefits. Social engagement has been prospectively associated with favourable change in depressive symptoms in some populations.51 52 There is also some evidence for lower cognitive decline in those with more social ties,53 while social integration has been found to delay memory loss in the US Health and Retirement Study.54 However, it is difficult to rule out the possibility of residual confounding by unmeasured health status in such associations.
Public health implications
Inability to carry out complex activities and limited social participation predict survival prospects and could provide a means of identifying ‘at risk’ women in the community for targeted support. If association with social participation is causal, this would suggest that interventions to improve participation in older people could delay mortality. However, complex care interventions have previously been found to have no overall benefit for mortality, although they can help with independent living.55 This is consistent with the recent finding that received social support is less predictive than social integration for mortality.20 Hence, community-based interventions that leverage naturally occurring community social capital with targeted individual interventions to increase social participation may prove more effective for reducing mortality. Conversely, in the current climate of worldwide recession, cuts to public spending could precipitate a decline in social participation among the elderly people that might ultimately result in higher mortality.
What is already known on this subject
The proportion of older disabled people in the UK and many other high-income countries is increasing rapidly.
Different aspects of disability, often studied in isolation, have been associated with mortality. However, their relative importance and whether their effect is accounted for by lifestyle factors and comorbidities are not well understood.
What this study adds
Using the disability framework provided by the WHO's International Classification of Functioning, Disability and Health, we showed that social participation and complex activities were the strongest predictors of mortality. These associations were independent of other disability domains as well as from lifestyle factors and major chronic comorbidities.
This study demonstrates the importance of social participation and complex activities in the elderly people, highlighting that these should not be overlooked in planned reforms to the social care system.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Files in this Data Supplement:
- Download Supplementary Data (PDF) - Manuscript file of format pdf
- Download Supplementary Data (PDF) - Manuscript file of format pdf
Footnotes
Caroline Dale, David Prieto-Merino contributed equally to this work.
Funding The British Women Heart and Health Study is supported by grants from the British Heart Foundation (EPNCCD08) and the Department of Health (009/0049). The funders had no role in the study design; in the collection, analysis and interpretation of the data; in the writing of the report or in the decision to submit the paper for publication.
Competing interests None.
Ethics approval This study was approved by London School of Hygiene & Tropical Medicine Ethics Committee and 23 Local Research Ethics Committees.
Provenance and peer review Not commissioned; externally peer reviewed.