Article Text

Abstract
Objective: To systematically review studies of the effects of the Compressed Working Week on the health and work-life balance of shift workers, and to identify any differential impacts by socio-economic group.
Methods: Systematic review. Following QUORUM guidelines, published or unpublished experimental and quasi-experimental studies were identified. Data were sourced from 27 electronic databases, websites, bibliographies, and expert contacts.
Results: Fourty observational studies were found. The majority of studies only measured self-reported outcomes and the methodological quality of the included studies was not very high. Interventions did not always improve the health of shift workers, but in the five prospective studies with a control group, there were no detrimental effects on self-reported health. However, work-life balance was generally improved. No studies reported differential impacts by socio-economic group; however, most of the studies were conducted on homogeneous populations.
Conclusion: This review suggests that the Compressed Working Week can improve work-life balance, and that it may do so with a low risk of adverse health or organisational effects. However, better designed studies that measure objective health outcomes are needed.
Statistics from Altmetric.com
Work has long been acknowledged as an important social determinant of health and health inequalities.1–4 Employment, or lack of it, and its quality and type are vital in terms of income and social status in all advanced industrialised societies. However, the nature of work has altered considerably over the past two decades, not least in terms of the cultivation of labour market practices in which skills, working hours, contracts, conditions, pay and location are more flexible.5 6 Similarly, a 24-hour society has started to emerge with associated concerns about abnormal working hours and work-life balance (WLB).7
In this context, recent reports from the UK Department of Health and Department of Work and Pensions, the US Department of Health and Human Services, and the World Health Organization show that the workplace is increasingly being considered by policymakers as an important intervention point at which health can be improved and health inequalities reduced.4 8–11 Attention to date has focused on the psychosocial work environment, in particular psychological demands and job control (individual decision authority), as explored in depth in the Whitehall studies.12–16 However, there is a largely untapped literature on the effects of particular types of work patterning on health and health inequalities, and, in particular, there is a large body of evidence spanning several decades that describes the negative effects of shift work on health and wellbeing.17 18
Reported health problems associated with shift work include sleep disturbances, fatigue, digestive problems, and stress-related illnesses, as well as increases in general morbidity, and in sickness absence.9 These health problems may derive from disruption to physiological, psychological and social circadian rhythms,17 18 as shift work, particularly that involving night work, disrupts the natural circadian rhythm, leading to disruption of sleep (as natural alerting mechanisms such as the cortisol surge and temperature rise will interrupt sleep) and daytime functioning (wakefulness at night will be reduced by temperature drops and melatonin surges). Sudden changes in schedule can, therefore, have an effect akin to “jet lag”. Disruption to the circadian rhythm can also lead to disharmony within the body as some functions (e.g. heart rate) adapt more quickly than others (typically endogenous functions such as body temperature, and melatonin).18 This leads to desynchronisation, which itself can result in psychological malaise, fatigue and gastrointestinal problems. Realignment can take several weeks.18 Most existing research emphasises these physiological changes, but shift work also involves significant social desynchronisation, involving working at times and on days that may make it difficult to maintain a balanced domestic and social life work life balance (WLB).20 Literature also suggests that cardiovascular problems such as hypertension and heart disease may be related to shift work.21 It has also been suggested that shift work is associated with breast cancer, (possibly due to circadian disruption) and the birth of pre-term (premature) babies, but the current evidence base is inconclusive.22–25 Shift work may also involve increased risk of injuries and accidents as performance fluctuates.26
Shift work may, therefore, be an important, but largely overlooked determinant of health and wellbeing for many workers. The practice is common with one in five European workers involved in shift work,25 though the definition of the term can be complex (the UK Labour Force Survey for example identifies ten different categories).27 Shift work is also socially patterned, being less common in graduates, and more common amongst manual workers and those working in the manufacturing or healthcare sectors.27
Changes to the organisation of shift work have the potential to reduce these negative health effects and perhaps also have an impact on social inequalities in health and wellbeing. A popular organisational level intervention is changing the hours of shift work by introducing a Compressed Working Week (CWW). The CWW is an alternative work schedule in which the hours worked per day are increased, whilst the days worked are decreased in order to work the standard number of weekly hours in less than five days.28 The CWW, therefore, represents a radical break from the 8-hour working day length favoured by workers and trade unions.27 However, a cap still remains on the number of hours worked per week (a maximum of 48 hours under the European Union Working Time Directive).27 The most popular forms of CWW are the 12-hour CWW, the 10-hour CWW and the Ottawa system.18 The 12-hour CWW involves four 12-hour shifts (day, night) over four days with three or four days off. Under a 10-hour CWW, four 10-hour shifts are worked followed by three days off. The Ottawa system consists of three or four 10-hour morning or afternoon shifts spread over four days, then two days off. This is followed by a block of seven eight-hour nights, then six days off.
In this paper, we present the results of the first systematic review of primary empirical studies on the health and WLB effects of changes to the organisation and experience of shift work brought about by CWW interventions, and any differential impacts by social group. Although previous literature reviews of the CWW exist, these concentrate on observational epidemiological (descriptive or comparative) studies rather than evaluative intervention studies, and have not been conducted using full systematic review methodology.7 1929
METHODS
Inclusion and exclusion
We sought to identify all empirical studies (both prospective and retrospective, with or without control groups) that examined the effects of CWW interventions on the health and WLB of shift workers and their families. For the purposes of the review, shift work was defined as “any regularly taken employment outside the hours of 07:00 and 18:00”.18 Interventions had to be implemented in actual workplaces, so non-workplace laboratory-based studies were excluded. Health-related outcomes included specific diseases, as well as more general measures of physical or psychological health and wellbeing. Sickness absence, health behaviours and injuries resulting from workplace accidents were included, as were physiological measures, and measures of physical and mental wellbeing such as tiredness, fatigue and sleep.22 The social impacts of the interventions, specifically on WLB were also examined. Organisational effects (eg job satisfaction, individual or organisational performance), when reported alongside the primary outcomes (health and WLB), were also recorded to help in understanding the motivations behind the CWW interventions, and also their viability. Impacts on inequalities in health were considered as outcomes.
Search strategy
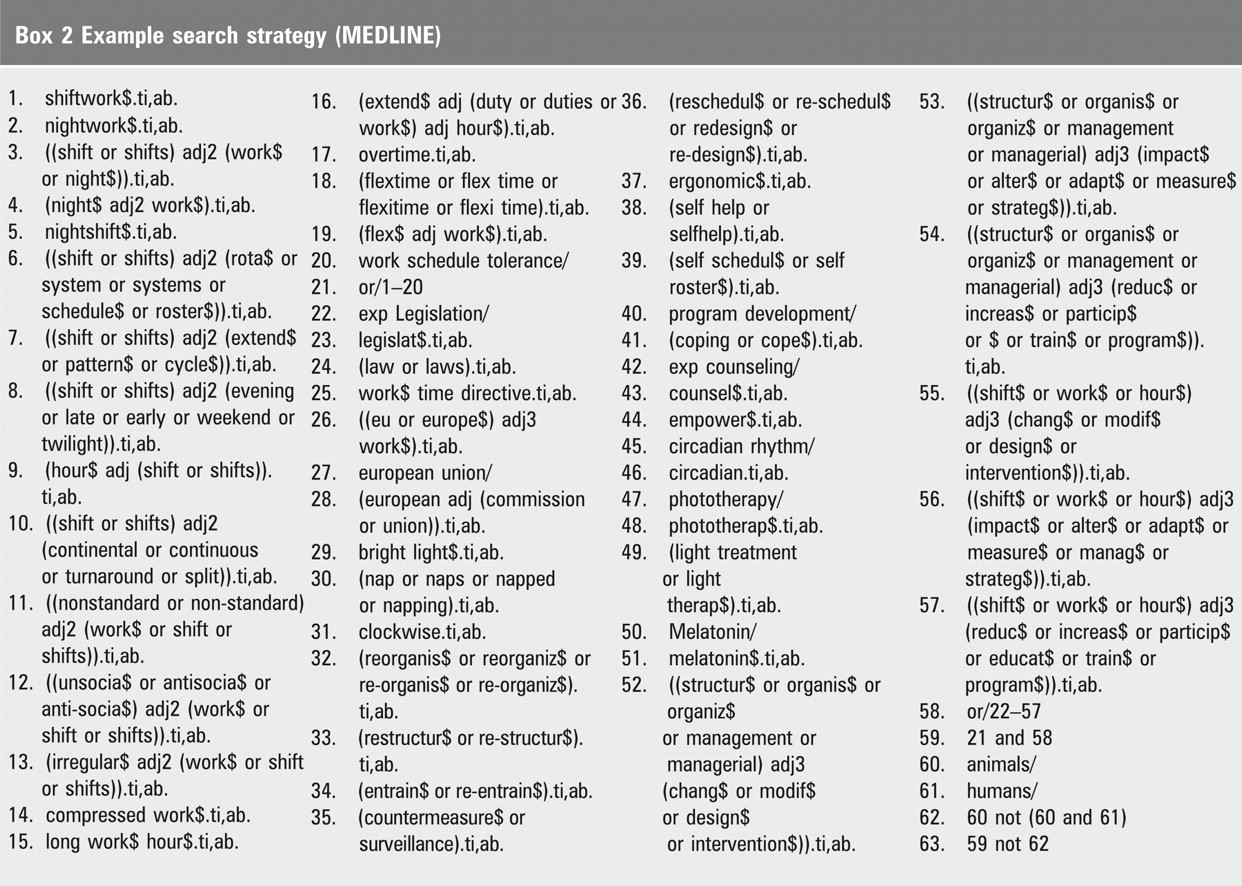
We searched 27 electronic databases and websites for documents of any type, from any country, at any time and in any language. Details of the databases searched and an example search for MEDLINE are detailed in boxes 1 and 2. The full search strategy is available online (Appendix 1). We also searched bibliographies and reference lists.
Box 1 Databases and websites
The following 27 databases and websites were searched from start date to November 2005:
ASSIA (CSA)
EU Community Research & Development Information Service
Dissertation Abstracts
Eric (CSA)
European Commission Libraries Catalogue
Econlit (Webspirs)
Electronic Collections Online (FirstSearch)
Embase (Ovid)
Geobase (FirstSearch)
Harvard Business Review
HMIC (OVID)
Index to Theses
International Bibliography of the Social Sciences (OVID)
JSTOR
Labordoc
Management Contents (Dialog)
Medline (Ovid)
Medline In-Process & Other Non-Indexed Citations (OVID)
NTIS
PAIS (Webspirs)
PapersFirst (FirstSearch)
PsycINFO (Ovid)
REGARD (ESRC)
Research Papers in Economics
Social Science Citation Index (Web of Science)
Sigle (Webspirs)
Sociological Abstracts (CSA)
{kind=link}
Data extraction
We located 13 308 titles, of which 419 were examined in more detail, and of these 88 were retrieved for full-paper analysis. The lead reviewer (CB) excluded obviously irrelevant titles and abstracts from the initial literature search, and retrieved full-text copies of the remainder. Studies making any reference to health or wellbeing were independently appraised by two reviewers (CB and MP), who re-examined papers jointly to resolve disagreements. We included percentages, confidence intervals (CI), p values, and effect sizes when they were reported in the original study, or calculated these statistics (using final sample sizes) if sufficient information was available (although lack of data was a problem in some studies).
Critical appraisal
Critical appraisal criteria were adapted from existing systematic reviews of the health effects of employment interventions and, guidance for the evaluation of non-randomised studies (box 3).30–32 Two reviewers (CB and MP) independently appraised the included studies according to these criteria.33 The critical appraisal criteria were used for descriptive purposes only and to highlight variations in the quality of studies (see tables 1–3). No quality score was calculated.
Box 3 Critical appraisal criteria30–32
Is the study prospective?
Is there a representative sample?
Is there an appropriate control group?
Is the baseline response greater than 60%?
Is the follow-up greater than 80% in a cohort study, or greater than 60% in a cross-sectional study?
Have the authors adjusted for non-response and drop-out?
Are the authors’ conclusions substantiated by the data presented?
Is there adjustment for confounders?
Were the entire intervention group exposed to the intervention? Was there any contamination between the intervention and control groups?
Were appropriate statistical tests used?
These criteria were used to appraise all of the included studies. The results of this process are presented under the critical appraisal section of the results in tables 1–3, with the numbers 1–10 representing satisfactory fulfilment of the corresponding criterion.
RESULTS
Forty studies examined the effects of CWW interventions on the health and WLB of shift workers.34–83 The majority of CWW studies examined changes to four days of 12-hour shifts, although four examined changes to 10-hour shifts,34 35 56–59 61 and two examined the introduction of the Ottawa shift system.37 78 Twenty-three of the studies were prospective cohorts,34–61 of which five were controlled.34–39 In this paper, we focus our detailed comments on the results of these better-designed studies (that is, the prospective cohorts with control groups), although the overall synthesis reflects the results of all 40 studies. Most of the CWW studies were based in one of four distinct occupational settings: healthcare organisations (9), the police force (8), manufacturing companies (11) or energy industries (9). No studies were found relating to other key shift-working occupations, such as retail or entertainment.26 The majority of health outcomes, and all WLB ones, were self-reported. In a sizeable number of the CWW studies, the intervention was either at the behest of the work force,34–36 41 47 49 60 69 70 83 or from the management (with a stated desire to improve health or WLB).37 50 62–64 66 71 74 79 80 82 However, in other studies, the motivation was more obviously efficiency or productivity.46 48 51 53 54 59 61 67 77 78 81 Results are summarised by study design in tables 1–3 and detailed results are available online (Appendix 2).
Health-related outcomes
The effects of the CWW interventions on health outcomes were not conclusive: a number of studies reported some improvements in workforce health,34–38 42–45 47–50 52 54 56–60 62–65 67 68 72–74 78–83 whilst others found no change,39 40 46 53 55 66 69–71 75 76 77 and two found only negative effects.41 51
The five prospective cohort studies with control groups34–39 found that there were no detrimental effects on self-reported health-related outcomes after the introduction of CWW (table 1), and in four of the studies some improvements were recorded.34–38 In one Canadian study of 30 police officers,34 35 self-reported health behaviour in the form of sporting activities improved in the intervention group compared with the control group (intervention mean 8.1 to 13.9, comparison mean 7.9 to 7.0, F = 8.8, p<0.01), but sickness absence rates did not change significantly. In another study of 70 UK police officers,37 all but one (sleep quality) of the self-reported health indicators improved significantly in the intervention group (e.g. for the General Health Questionnaire scores, the intervention mean improved from 11.2 to 7.1, whereas the comparison mean worsened from 11.0 to 11.9, F = 15.56, p<0.001). However, our critical appraisal of this study identified notable differences in health at baseline between the control and intervention groups: the intervention group had a better baseline score than the control group, thereby possibly leading to an exaggerated intervention effect.
In a Swedish study of 46 chemical plant workers,38 self-reported sleep quality was generally better in the intervention group, eg mean scores for “feeling rested when wake up” improved in the intervention group (from 4.06 to 4.47) whilst they worsened in the comparison group (4.38 to 4.23). However, self-reported changes in fatigue, sufficient levels of sleep and general health did not differ from the control group at follow-up. Our critical appraisal of this study38 queried the suitability of the control group, and noted a lack of adjustment for confounders or non-responders (table 1). In a Canadian study of 85 young male mine workers,36 self-reported sleep problems and tiredness showed no difference between the intervention and control groups; however, levels of sickness absence decreased substantially (reduction of 73% in the intervention group compared with only 2% in the control group), as did the number of accidents (reduction of 69% in the intervention group compared with only 10% in the control group). The critical appraisal of this study,36 though, suggests that the sample was not representative, the baseline and follow-up responses were low and that there was a lack of adjustment for confounders or non-responders (table 1).
In another study,39 of 45 UK police officers, self-reported health did not improve: chronic fatigue, physical health and GHQ-12 (a generic measure of psychological stress) scores did not differ between the intervention and the control group at follow-up, and the significant improvement in sleep duration in the intervention group disappeared when shift work experience was taken into account. This study was not notably different from the others in terms of methodological quality.
Although these studies were robust in terms of study design (employing control groups), the sample sizes were small, ranging from 23 to 85, and the lengths of follow-up were relatively short. No study followed up respondents for at least a year, which may be the optimum as it allows for the possibility of controlling for possible seasonal effects. It should also be noted that three of the five controlled prospective studies were conducted in the police force and so care is needed in generalising from these results to other occupational groups involved in shift work.
The uncontrolled prospective studies (table 2) were also inconclusive, as, whilst the majority identified an improvement in one or another of the various health outcomes measured, they found little effect for other health outcomes.43–45 49 50 52 54 56–59 62–65 67 68 Amongst the five largest studies (sample sizes >100),49 51 59–61, two reported mixed health effects,49 59 two reported health improvements60 61 and one recorded a negative health effect.51 Williams’ study of 131 male chemical plant workers49 recorded an improvement in self-reported depression (decreased from 2.43 to 2.12, t = 2.32, p<0.05), but found no change in absence and injury rates.49 Similarly, a study of Canadian mine workers59 found that after the introduction of CWW, sleep (mean difference = −0.3, t = 2.43, p<0.01) and tiredness (mean difference = 0.9; t = 4.77, p<0.001) worsened on the day shift whilst gastrointestinal problems (mean difference = −0.4, t = 2.35, p<0.01) and headaches (mean difference = −0.3, t = 2.07, p = 0.03) improved. Two studies of American production workers60 61 reported various improvements in self-reported health, including a decrease in the prevalence of common shift-related health disorders (such as heartburn, acid stomach and diarrhoea) from 43.8% to 27% (p<0.001)59 and a decrease in sickness absence (eg from 11.39 to 4.69 days).61 However, in a study of 150 UK nurses,51 dissatisfaction with levels of mental (0.8 (0.53 to 1.07)) and physical (0.7 (0.50 to 0.90)) fatigue increased.
A number of smaller studies of varying methodological quality and sample size reported no changes in any of the health indicators.40 46 53 55 66 Other studies were more conclusive, finding significant improvements in sleep duration,42 absence,47 physiological distress, fatigue and stress,48 sleep between shifts, sleep difficulties, and health disorders.60 In all these studies,42 47 48 60 employees were either involved in the design and implementation of the intervention or they were supportive of the change. Importantly, only two studies, both based in healthcare settings, found that all the self-reported measures of health worsened after the introduction of the CWW.41 51 Overall, the prospective studies were rather limited in terms of length of follow-up and sample size: only three studies had lengths of follow-up of 12 months or more, and the studies were small (tending to involve 15 to 50 participants).
The pattern was similar for the retrospective studies (table 3), with only a minority reporting any significant intervention effect (table 3).72–74 78–83 The majority of the significant effects, though, were positive, particularly in terms of self-reported general health and morbidity;72 73 78 headaches, gastric upset, diarrhoea, and alcohol problems;72 73 sleep;74 and injuries.79–81 83 These retrospective studies were generally of low quality; all had sample sizes <100; and low response rates. However, one of the larger and better-quality retrospective studies,72 73 with a sample of 247, a response rate >60% and adjustment for demographic confounders, reported a significant decrease in the age-standardised morbidity ratio amongst men from 1.02 (95% CI 1.00 to 1.05) to 0.47 (95% CI 0.46 to 0.48), but a non-significant decrease in women from 0.76 (95% CI 0.71 to 0.82) to 0.67 (95% CI 0.63 to 0.71).
Fatigue
Shift work is often associated with fatigue18 20 26 and it might be expected that CWW, due to the longer working day, the potential for moonlighting, or excessive overtime, might further increase problems of fatigue amongst shift workers. However, of the 18 intervention studies covered in this review that measured fatigue or tiredness, in only four was there an adverse change in fatigue levels after the introduction of CWW.41 51 59 67 Three studies recorded improvements,42 53 59 and in the other eleven there was no intervention effect.41 43–45 51 69 72 75 80 81 86 The introduction of longer working days under CWW does not, therefore, appear to adversely affect fatigue; however, this may well be because of the extended rest period, which means that the normal weekly working hours are not exceeded in a seven-day period.28 However, it may also be due to the popularity of CWW interventions amongst workers (as they increase leisure time and/or enable moonlighting)39, and this may bias the findings of evaluations in a positive direction, especially in studies with a short follow-up period. Subsequently, it is important that employee safeguards such as the EU Working Time Directive or other measures that limit overtime and moonlighting are incorporated into CWW schedules.
Work-life balance
The majority of studies that examined WLB outcomes noted improvements after the introduction of CWW,34 35 37 38 40 46 48 49 53 54 62–65 68 74 77 78 82 with only a few reporting no intervention effect36 39 47 50 or a worsening in WLB.43–45 51 54 However, CWW are often popular amongst shift workers, largely because they value the additional days off that are afforded by the CWW model.84 Indeed, in 22 of the CWW studies, the intervention was either specifically requested by the employees,38–40 45 51 53 64 73 74 87 or implemented with their support.48 54–59 61 65 67 71 74 78–81 Similarly, the ability of an individual worker to adapt the new schedule to his/her needs may have influenced findings.
Three of the five prospective cohort studies with control groups (table 1) recorded significant improvements in self-reported WLB amongst the intervention group compared with the control group.34 35 37 38 In the Barton-Cunningham study of 30 Canadian police officers,34 35 all four of the indicators of wellbeing used in the study were significantly improved in the intervention group (eg time spent on domestic chores improved in the intervention group from a mean of 7.8 to 16.0, whereas the comparison mean worsened from 8.6 to 6.5, F = 14.7, p<0.01). These improvements all disappeared when the old eight-hour schedule was restored.34 35 Similarly, in the Totterdell and Smith study of 70 UK police officers37 all WLB indicators were improved in the intervention group (for example, a reduction was recorded in the intervention group for “insufficient time for family”, intervention mean 56.4 to 15.5, comparison mean 63.8 to 62.6, F = 41.61, p<0.001). However, there were significant differences between the intervention and control groups at baseline, which suggests that the findings need to be replicated in larger studies with well-matched control groups.
The Swedish study of 46 chemical plant workers38 also saw significant improvements in WLB with both time for social/family activities (intervention mean 2.65 to 3.02, comparison mean 3.25 to 3.02, p<0.05), and satisfaction with hours (intervention mean 3.53 to 4.62, comparison mean 4.29 to 4.5, p<0.05) increasing amongst the intervention group. There are some issues (as above) about the suitability of the non-randomised, non-matched control group (see table 1).
The other prospective study with a control group of 45 UK police officers39 found no changes in WLB (workload, social domestic interference) once shift work experience had been taken into consideration. Similarly, the study of 85 mine workers36 found no differences between the intervention and control groups for family satisfaction. Importantly though, none of the prospective cohort studies with control groups identified a decrease in WLB after the implementation of the CWW interventions. As noted above, these studies tended to employ relatively short periods of follow-up and small samples, and so, despite the controlled design, the evidence they present is suggestive rather than convincing.
Consistently, the prospective uncontrolled studies (table 2), including two of the studies with at least 12 months follow-up, found that aspects of WLB improved after the introduction of CWW interventions.40 46 48 49 54 62–65 68 WLB indicators (such as time available for recreation, time spent with family, or conflict between work and non-work time) improved in eight studies.40 46 48 49 54 62–65 68 Some smaller and less methodologically robust studies (e.g. low response and follow-up rates) did not identify any changes in WLB as a result of the intervention.47 50 Only three studies,43–45 51 54 of which all but one51 were revealed by our critical appraisal process to be of questionable methodological quality (small sample size, low response and follow-up rates, etc), reported any decreases in WLB and in two of these less robust studies only one or two aspects of WLB declined whilst others improved54 or were unaffected.43–45
In all of the retrospective studies that measured the effects of CWW interventions on WLB, it was found to improve.74 77 78 82 For example, improvements were reported in leisure time and time spent with partner,74 quality of life77 and family life,78 and child care.82 However, the critical appraisal process suggested that these studies had some methodological problems particularly in terms of low baseline response rates,77 78 low or no follow-up response rates,74 77 78 82 and little adjustment for non-responders or confounders.74 77 78 82
Health and work-life balance
The results of the CWW studies suggest a link between improved WLB and improved health. Three of the prospective studies with control groups,34 35 37 38 six of the prospective studies without a control group48 49 54 62–65 68 and three of the retrospective studies reporting increases in WLB,74 78 82 also reported improvements in health, particularly mental health. Changes in WLB were less likely to be accompanied by changes in measures of physical health. For example, in five studies,36 43–45 47 50 health improvements occurred despite no accompanying changes in WLB. This tentatively suggests that whilst changes in mental or physical health and WLB can clearly occur separately, positive changes in WLB can translate into positive mental health effects. The relationship between WLB and physical health, however, is less clear. Of course, this finding may reflect the self-reported nature of the health and WLB outcomes. However, this link and possible causal pathway should be examined further in future prospective studies.
Organisational outcomes
Generally, the studies suggested that the organisational effects of the CWW were small or absent with most studies finding no evidence of either benefit or detriment.34–37 42 47 49 52 54 65 66 68 78
Three of the prospective cohort studies with control groups (table 1) measured effects on performance (job satisfaction or effectiveness at work).34–37 None found any significant differences between the intervention and control groups. Similarly, in the other prospective cohort studies (table 2) the majority of the sixteen that measured organisational outcomes found no effect,42 47 49 52 54 65 66 68 whilst several reported improvements; in morale,53 62–64 job satisfaction,61 48 60 productivity and quality60 or organisational effectiveness.48 However, four studies reported adverse organisational effects such as an increase in turnover,41 decreased job satisfaction51 or decreased performance.59 67 Amongst the five retrospective studies that had organisational outcomes,76–80 82 four identified benefits in terms of reduced staff costs and errors,79 80 82 productivity,77 or morale.78 Overall, the balance of best evidence suggests that there were few positive or negative organisational effects, though it is possible that negative findings in this area may not have been published or may otherwise be unavailable (for example, for reasons of commercial confidentiality).
DISCUSSION
Overall, the evidence base on the health effects of CWW interventions is perhaps best described as cautiously positive: positive because whilst the CWW interventions might not always improve the self-reported health of shift workers, they are seldom detrimental (indeed, the five prospective cohorts with control groups found no detrimental effects on health); and cautious because of the methodological quality of the current evidence base (box 4). In contrast, the evidence on the effects of CWW interventions on the WLB of shift workers seems more conclusive (although the comments about methodological quality still apply): the CWW improves WLB.
Research implications
The evidence base on changing the organisation of shift work by introducing the CWW is relatively large by systematic review standards, both in terms of the intervention studies covered in this research report (40 in total), and the wider descriptive epidemiological literature.29 However, there are still some large evidence gaps, most notably in terms of any effects of shift work interventions on inequalities in health amongst working-age populations. The majority of studies were conducted in fairly homogeneous populations (eg police officers, male production workers, or female nurses) and, perhaps in part due to this, only one study differentiated outcomes by gender,72 73 and none of the studies differentiated by occupational grade or socio-economic group.
A key question remains of whether changing the organisation of shift work by introducing CWW has the potential to decrease health inequalities amongst the working-age population. An important consideration in this respect is the social patterning of shift work in the UK, which tends to be concentrated amongst workers from lower socio-economic groups (with the notable exceptions of medical and emergency services staff).27 This contributes to the generally poorer, more health-damaging work environment experienced by manual compared with non-manual workers. It is plausible that CWW interventions that improve the health of shift workers may, therefore, on the whole, help to reduce the gap in health between manual and non-manual workers caused by the differences in working conditions between the two groups. This possibility should be explored further.
There is also little evidence on the effects of CWW on the health behaviours of shift workers. Only four of the 40 studies in this review examined health behaviours. Two studies reported on the effects on exercise with one reporting an increase,34 35 whilst the other found no change;50 one study reported an increase in alcohol consumption,68 and another found no intervention effect on the consumption of social drugs.52 Furthermore, there were only two studies on the Ottawa CWW system,37 78 and so the effects of particular CWW systems is another area that could be examined in future research.
In addition, the research studies reviewed were subject to a number of methodological limitations (see box 4) such as inadequate control groups, lack of detail about implementation, small sample sizes and short follow-ups. Perhaps most importantly, the majority of outcomes were self-reported and this may have led to confounding, particularly in terms of whether employees were supportive or unsupportive of the imposed intervention. Therefore, in the future, prospective, well-controlled studies, which measure objective health outcomes, and which describe the background to the study and the implementation of the intervention, are needed.85 Studies that examine the mental health effects of CWW interventions and any interaction with changes in WLB would be the most useful.
Policy implications
The existing evidence, albeit somewhat methodologically limited, suggests that introducing the CWW may enhance the WLB of shift workers. There is also evidence to suggest that it is not detrimental to self-reported health in the short term. Importantly, CWW interventions tend to have either positive or negligible organisational effects and so employee health and WLB may be improved through the workplace without damaging company productivity or competitiveness. This message may be a useful aid in implementing the recent cross-departmental Health and Safety Executive, Department of Health and Department for Work and Pensions’ “Health, Work and Wellbeing” strategy86 amongst employers. Changing shift work organisation and working practices to make them more conducive to a WLB does not necessarily need a warning caveat about the dangers to productivity or competitiveness.
Box 4 Methodological limitations
Although the 40 studies reviewed represent the best available evidence on the health and work-life balance effects of Compressed Working Week (CWW) interventions, they were subject to a number of methodological and other limitations.
No trials and only five prospective cohort studies with a control group were located. The control groups were not matched or randomised, and in at least one case there were significant differences in health at baseline between the intervention and control groups.37
We elected to include all studies regardless of sample size. However, it needs to be noted that a number of studies were based on such small final sample sizes that their research value is limited. For example, nine studies50 52–58 68 79 80 82 had final sample sizes of 20 or fewer, and there was one study with only three participants.55 Therefore, in our synthesis, we have highlighted the larger studies.
Studies were often conducted in homogeneous populations. For example, three of the five controlled prospective cohorts were conducted amongst police officers.34 35 37 39 The generalisablity of the results to other occupations is, therefore, limited.
The number of small studies also raises the possibility that any positive findings may be due to publication bias, in which small studies with positive findings are more likely to be published (or are otherwise more easily located by reviewers) than those with negative findings. Similarly, bias may have arisen as we were only able to locate studies in the public domain, thus excluding the majority of commercial studies.
The health, work-life balance and organisational measures were usually self-reported and they varied greatly from study to study. Bias may, therefore, have occurred, as employees were aware of the intervention and in some cases highly involved in its design and implementation. There was a dearth of well-validated questionnaires, such as the General Health Questionnaire37 39 52 65 68 or the Standard Shift Work Index.39
The study follow-ups were generally 12 months or less34–55 59 62 74 76–80 82 and so it was not possible to analyse the longer term health or work-life balance effects of the CWW interventions, which may be particularly important in terms of accumulated fatigue and physical health. The short follow-ups may also account for the lack of a health effect (either positive or negative) in the majority of the studies.
There was also a lack of information provided in some studies about the background38–40 42–45 52 55–58 65 68 72 73 75 76 to the interventions or how they had been implemented.34–46 48 50–53 55–59 61–68 71–73 75–79 82 In those studies that reported background details, those in which the intervention was instigated by employees or the motivation was employee wellbeing,34–37 41 47 49 50 60 62–64 66 69–71 74 79 80 82 83 tended to have more positive health and work-life balance effects, whilst the effects of those that were the most overtly driven by economic motives were often negative or negligible.46 51 53 54 59 61 67 77
Policy implications
The evidence suggests that introducing the Compressed Working Week may enhance work-life balance for shift workers. It does not appear to be detrimental to self-reported health in the short term.
Importantly, Compressed Working Week interventions tend to have either positive or negligible organisational effects and so health and wellbeing may be improved through the workplace without damaging productivity or competitiveness.
The Compressed Working Week could, therefore, be an important tool for both policymakers and employers in terms of promoting healthier work places and improving working practices.
What is already known on this subject
A large number of observational studies suggest that shift work negatively effects employee health and work-life balance.
Shift work is common: one in five European workers are involved in some form of shift work.
Shift work is socially patterned – less common amongst graduates and more common amongst manual workers.
One hypothesis is that organisational level interventions such as the Compressed Working Week may be effective in reducing these negative health effects and perhaps also impact upon social inequalities in health and work-life balance.
What this study adds
This is the first study to systematically review 40 intervention studies of the effects on the health and work-life balance of shift workers of Compressed Working Week interventions.
The methodologically limited evidence base suggests that the Compressed Working Week appears to improve the work-life balance of shift workers, and that it appears to do so with little or no adverse health or organisational effects.
It is unclear what the effects are on health inequalities, although as shift work is concentrated amongst lower occupational groups it is plausible that effective Compressed Working Week interventions could help reduce the health gap between manual and non-manual workers.
Acknowledgments
The work in this paper was undertaken by the Centre for Public Policy and Health (University of Durham), the MRC Public and Social Health Sciences Unit (Glasgow), the Centre for Reviews and Dissemination (University of York), and the Department of Public Health (University of Liverpool) as part of the work of the Public Health Research Consortium (PHRC). The Public Health Research Consortium is funded by the Department of Health Policy Research Programme. The views expressed in the publication are those of the authors and not those of the DH. Information about the wider programme of the PHRC is available from www.york.ac.uk/phrc
REFERENCES
Supplementary materials
web only appendices 62/9/764
Files in this Data Supplement:
Footnotes
Funding: Department of Health Policy Research Programme (Public Health Research Consortium).
Competing interests: None.
Linked Articles
- In this issue