Article Text

Abstract
STUDY OBJECTIVES To assess the incidence of seroconversion and seroreversion in IgG antibodies to Helicobacter pylori within a 11 year observation period using these events as markers for acquisition and loss of the infection, respectively.
DESIGN Population based prospective cohort study
SETTING Northern part of Copenhagen County, Denmark
PARTICIPANTS AND METHODS A random sample of 2527 Danish adults were examined and blood obtained in 1983 and in 1994. Matching pairs of sera were analysed for the presence of IgG and IgM antibodies toH pylori with an in house enzyme linked immunosorbent assay. Participants who were seronegative at study entry and seropositive at follow up and had a fourfold increase in baseline IgG antibody levels were categorised as seroconverters and regarded as having acquired H pylori infection. Participants who were seropositive at study entry and had at least a fourfold decrease in baseline IgG antibody levels at follow up were assumed to have lost the infection (seroreverters).
RESULTS The seroprevalence of H pylori infection was 24.7 (95% confidence intervals (95% CI) 23.0, 26.4) % in 1983 and 24.5 (95% CI 22.8, 26.2) % in 1994. A total of 14 participants seroconverted within the observation period (cumulative 11 year incidence proportion: 1.0 (95% CI 0.5, 1.5) %). Having increased IgM antibody levels at study entry significantly increased the likelihood of IgG seroconversion (relative risk 6.4 (95% CI 2.1, 19.6). Seroreversion was seen in 48 participants (cumulative 11 year incidence proportion: 7.7 (95% CI 5.6, 9.8) %).
CONCLUSIONS Changes inH pylori infection status with time are rare in Danish adults. Few adults become infected with H pylori in Denmark.
- Helicobacter pylori
- seroconversion
- sero-reversion
Statistics from Altmetric.com
Helicobacter pylori is a human pathogen bacterium that causes chronic gastritis, peptic ulcer disease, and is a probable cause of gastric cancer.1-4 Although most cases of H pylori infection are acquired in childhood,5 6 cross sectional studies have shown that the prevalence of infection increases steadily with age.7-11 It is generally agreed that this age related increase in prevalence is attributable to a cohort phenomenon—that is, that certain birth cohorts have been exposed to H pylori early in life and retain a high infection rate throughout life.9 12 First time H pyloriinfection in adult life is rare and annual incidence rates have been low ranging from 0.006 to 1.1 per cent.13-19
Whereas spontaneous eradication of H pylori infection after primary acquisition of the bacteria has been reported in infancy,20 21 spontaneous eradication seems to be rare in adults. Once acquired, the bacterium stays in the stomach for life in most cases unless gastric atrophy develops.19 22 Incidental eradication ofH pylori secondary to antimicrobial treatment of other infections is probably unlikely,23 butH pylori can be eradicated by a triple or quadruple therapy that combines an antisecretory drug with different antimicrobials. When eradication is successful, serum levels of IgG and IgA antibodies directed against H pylorisurface antigens decline significantly within two to six months but do not return to pre-infectious levels.24-27
The aim of this study was to assess the cumulative 11 year incidence proportion of IgG seroconversion and seroreversion as markers for acquisition and loss of H pyloriinfection, respectively in a random population of Danish adults.
Methods
STUDY POPULATION AND RESPONSE PATTERN
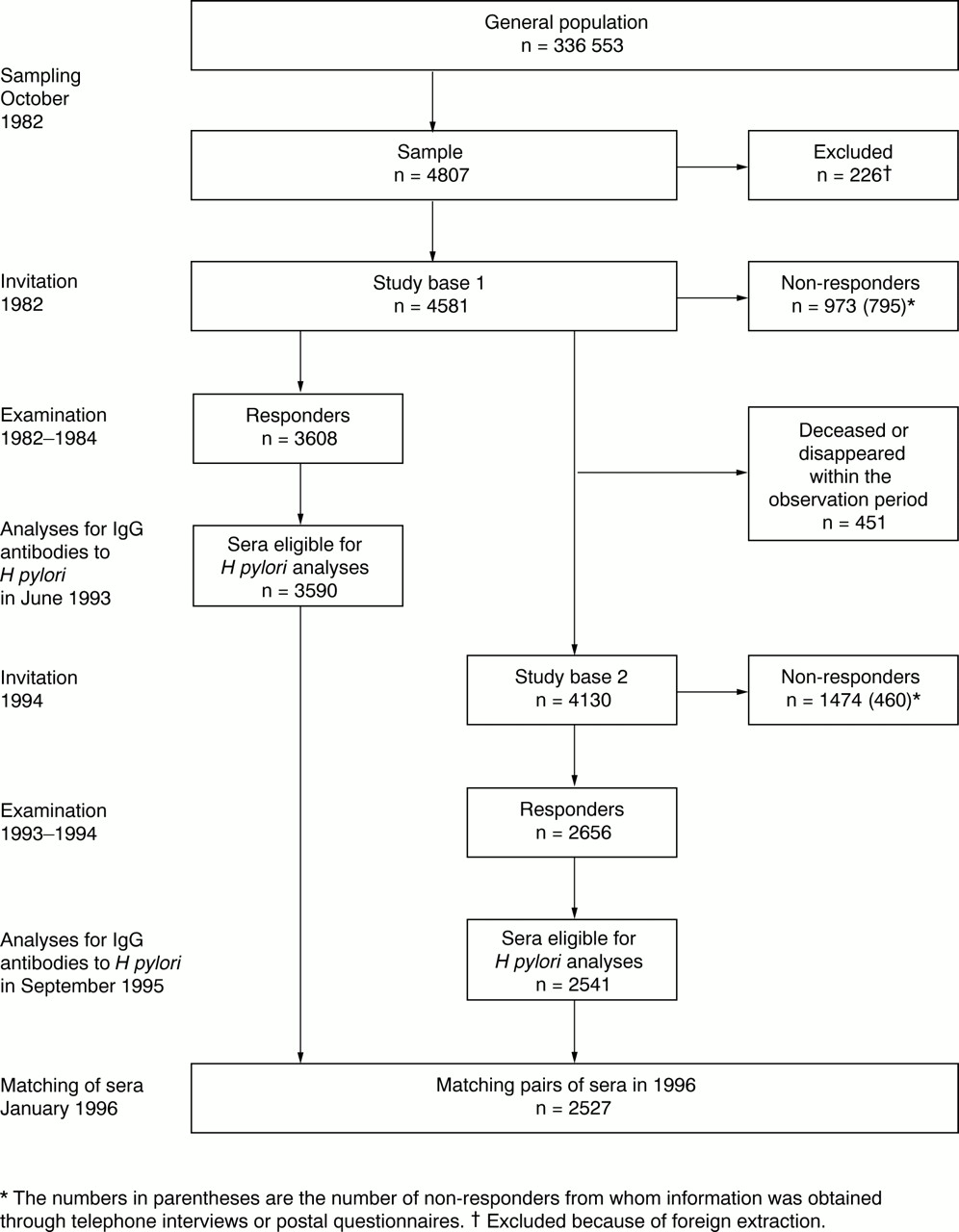
In October 1982, a population study governed by the World Health Organisation for the Monitoring of Trends and Determinants in Cardiovascular Disease (DAN MONICA) was initiated at the Copenhagen County Centre of Preventive Medicine at the Glostrup University Hospital, Denmark. An age and sex stratified sample consisting of 2404 men and 2403 women, (age 30, 40, 50, and 60 years) was drawn from the National Danish Civil Registration System, in which all people who live in Denmark are registered by a unique 10 digit number. After 226 people of foreign extraction had been excluded, 2280 Danish men and 2301 women (study base 1) were invited to a general health examination by a standard letter containing information about the project (fig1).29 Also enclosed was a self administered questionnaire concerning medical history, drug consumption within the preceding five years, and health and lifestyle practices. Between November 1982 and February 1984, 3608 people (response rate 78.8 per cent) (m/f=1843/1765) entered the study (fig 1). Data on the non-responder group (n=973) were as previously reported.28 29
{kind=link}
Sampling and response pattern in 4581 Danish adults who were invited for a population study in 1982.
By January 1993, 450 members of study base 1 had died and one person had disappeared. The remaining 4130 sample members of Danish extraction (study base 2) were re-invited to a follow up examination. A total of 2656 people (response rate 64.3 per cent) (m/f=1333/1323) attended the follow up examination that took place between June 1993 and December 1994 (fig 1). Among non-responders at follow up, 460 people were interviewed by telephone, 57 people had died between invitation and scheduled examination, 458 people refused to participate, and 499 people could not be reached.
The project was approved by the Regional Research Ethics Committee of the Copenhagen County.
MATCHING OF SERUM SAMPLES
Serum samples were obtained from 3590 participants at study entry and from 2541 participants at follow up. Sera obtained at study entry were thawed for the first time and analysed in June 1993.30 Sera obtained at follow up were analysed in September 1995 (fig 1). Matching pairs of sera were identified in 2527 cases. This study is based on these eligible pairs of sera.
DETECTION OF IGG AND IGM ANTIBODIES TO H PYLORI
IgG antibodies against a low molecular weight fraction ofH pylori antigens and IgM antibodies against heat stable H pylori antigens were measured in duplicate with an in house indirect enzyme linked immunosorbent assays (ELISA) as previously described.30-32 The IgG serology had been validated in a mixed population of 250 Danish adults with dyspeptic symptoms; a population that was comparable to the present study population in terms of sociodemographic factors and ethnicity.32 33 The sensitivity, specificity, positive predictive value, and negative predictive value was 98.5, 54.0, 76.1, and 96.2 per cent, respectively. Borderline cases were people with indeterminate IgG antibody levels between the cut off points for seronegativity and seropositivity. The assay was previously tested against commercially available assays and yielded similar sensitivity and specificity values when applied to a mixed population.34
To rule out that changes in the ELISA procedure between the initial and the follow up analysis affected antibody measurements, sera from people who changed antibody status and from people who showed a significant increase in IgG antibody levels within this period were re-tested pair wise on the same ELISA plate.
DEFINITIONS OF IGG SEROCONVERSION AND SEROREVERSION
Because of the uncertainty inherent to borderline cases two different definitions of IgG seroconversion were applied. Both definitions implied at least a fourfold increase in baseline IgG antibody levels within the observation period. The most strict definition (1) included people as seroconverters who were seronegative at study entry and seropositive at follow up. When using definition (2), seroconverters were those who were either seronegative or IgG borderline at study entry and seropositive at follow up. Seroreverters were seropositive at study entry and showed at least a fourfold decrease in baseline IgG antibody levels at follow up.
USE OF ANTIMICROBIALS WITHIN THE FIVE YEARS PRECEDING FOLLOW UP EXAMINATION
To examine if there was any association between the use of antimicrobials and IgG seroreversion, all participants were asked about their use of antibiotics within the five years preceding follow up (no use; daily use; weekly use; monthly use; long term prophylactic antimicrobial regimens). Daily, weekly, or monthly use, and long term prophylactic antimicrobial regimens were considered affirmative answers. No information was available on the duration or the type of antimicrobial treatment used.
INCREASED IGM ANTIBODY LEVELS ONLY AT STUDY ENTRY
People who had increased IgM antibody levels toH pylori unaccompanied by an increase in specific IgG and IgA antibody levels at study entry were suspected of harbouring a primary H pyloriinfection.30 To assess the validity of a solitary IgM increase as a marker for primary infection, IgG seroconversion rates were compared in this subgroup and in IgG negative people at follow up.
STATISTICAL METHODS
The SPSS statistical package for Windows was used.35The 11 year cumulative incidence proportion of IgG seroconversion (11 year seroconversion) according to definition (1) was calculated for participants who remained at risk of acquiring a first timeH pylori infection at study entry—that is, participants who were seronegative at study entry. When definition (2) was applied the population at risk also included participants with borderline increased IgG antibody levels at study entry.
The 11 year cumulative incidence proportion of IgG seroreversion (11 year seroreversion) was calculated in participants who were IgG seropositive when entering the study. Sex and age differences in cumulative incidence proportions were examined with the χ2 test.36 Ninety five per cent confidence intervals (95% CI) for proportions were obtained from the binomial distribution.
Results
key points
-
Serological signs of acquisition ofH pylori infection are uncommon in Danish adults. Studies on which factors predispose to the infection should focus on factors exerting their effect in childhood.
-
The seroprevalence ofH pylori infection in Danish adults does not change markedly with time. A single baseline assessment ofH pylori infection status is probably sufficient for aetiological studies on H pylori related diseases.
-
Only a minor proportion of people with solitary increased IgM antibodies to H pylori develops serological signs of long termH pylori infection.
IGG SEROPREVALENCES IN 1983 AND 1994
Whereas IgG seroprevalences increased significantly with age in women at both attendances IgG seroprevalences did not change significantly after age 40 in men (table 1). The overall seroprevalence of H pylori infection remained unchanged within the observation period. When stratified by age, minor and insignificant changes in age specific seroprevalences were seen between 1983 and 1994. There was an insignificant tendency towards higher prevalences of H pylori infection in men than in women in 1994.
The IgG seroprevalence % (n), of H pylori infection in 1983 and 1994 in 2527 Danish adults, by sex and age
NON-RESPONDERS AT FOLLOW UP
Cohort members that did not attend the follow up examination (non-responders) were more likely than responders to be old (relative risk 1.7 95% CI 1.5, 1.9) and to report low socioeconomic status (relative risk 1.6 95% CI 1.4, 1.8). The seroprevalence ofH pylori infection at study entry was significantly higher in non-responders than in responders (table 2).
IgG seroprevalence of H pylori infection (n/%) at study entry (responders and non-responders) and at follow up
IGG SEROCONVERSION
According to definition (1) 14 people seroconverted in IgG antibodies within the observation period (tables 2 and 3). A total of 1431 people were seronegative at study entry and remained at risk of acquiring H pylori infection. The 11 year seroconversion rate for both sexes was 1.0 (95% CI 0.5, 1.5) % (table3). When definition (2) was used, 38 people seroconverted among 1903 people at risk of acquiring H pyloriinfection resulting in a 11 year seroconversion rate of 2.0 (95% CI 1.4, 2.6) % (table 3). There was a tendency towards higher seroconversions rates with age in men. No sex differences were seen in seroconversion rates.
The 11 year incidence of seroconversion and seroreversion % (n) in IgG antibodies to H pylori in 2527 Danish adults, by sex and age
IGG SEROCONVERSION IN PEOPLE WITH SOLITARY INCREASED IGM ANTIBODY LEVELS AT STUDY ENTRY
A total of 48 people who had increased IgM antibody levels unaccompanied by an IgG or IgA antibody response at study entry were examined at follow up. Three persons (6.3 per cent) seroconverted in IgG antibodies within the observation period. Relative risk of seroconversion in this subgroup compared with people who were IgG seronegative at study entry was 6.4 (95% CI 2.1, 19.6).
IGG SEROREVERSION (LOSS OF H PYLORI INFECTION)
A total of 48 people were IgG seropositive at study entry and had a fourfold decrease in baseline IgG antibody levels within the observation period, suggesting seroreversion (table 3). The 11 year seroreversion rate was 7.7 (95% CI 5.6, 9.8) %. Among this group, 22 people were seronegative at follow up, whereas the remaining 26 people had antibody levels in the indeterminate region (table 2). There was an insignificant tendency towards higher seroreversion rates among women compared with men (relative risk 1.3 (95% CI 0.8, 2.3)). Young and middle aged people had slightly higher seroreversion rates than older people (table 3).
USE OF ANTIMICROBIALS AND IGG SEROREVERSION
Two people among 48 seroreverters had used antibiotics on one or more occasions within the past five years, whereas the corresponding numbers were 29 among 529 participants who tested IgG seropositive at both attendances. The relative risk of seroreversion was 0.8 (95% CI 0.2, 2.9) for antimicrobial users compared with those who had not used antimicrobials.
Discussion
In this population based prospective cohort study comprising more than 2500 Danish adults a low incidence of seroconversion in IgG antibodies to H pylori and a high incidence of seroreversion was found. Given that these events reflect acquisition and loss of H pylori infection, respectively, the overall prevalence of the infection may, perhaps also attributable to a cohort phenomenon, decline within the next decades.
The clinical picture of acute H pyloriinfection has been described in a few anecdotal reports.37These infections have manifested mild, but transient dyspeptic complaints, that are likely to go undiagnosed. The lowH pylori infection incidence rate found in this study supports the observation that acute H pylori induced gastritis is rarely seen in daily clinical work. The only lower seroconversion rate was found in a Canadian population.15 The latter study had a short observation period (two to three years) and only one person seroconverted (table4).13-18 38 H pyloriinfection rates in Denmark are generally low.11 30 For this reason, the risk of being exposed to H pylori is small.
Annual incidence (%) of first time H pylori infection in comparable studies
The response rate at follow up was low and non-responders more often emanated from poor socioeconomic levels. As H pylori infections are more frequent in deprived people, it is possible that non-responders were more likely to acquireH pylori infection than responders. This bias could result in an underestimation of the incidence of IgG seroconversion.
Serological assessment of infection status has mostly been performed at two points in time in previous studies on the incidence ofH pylori infection.13-18Incidence estimates have been based on the assumption that a person can change infection status only once within the follow up interval. Spontaneous loss of the infection is well evidenced in children20 21 but has not been reported in adults unless accompanied by gastric atrophy. Still, it cannot entirely be ruled out that self limiting episodes of infection may occur in adults. Incidences of H pylori infection calculated in this and previous studies may, therefore, underestimate the true incidence of infection. The proportion of primary infections that persists as well as which factors determine the persistence of the infection also remains unknown.
Misclassifications because of false positive and false negative serology results may introduce significant bias when the incidence of IgG seroconversion and seroreversion is estimated.39 The low specificity of the present serological results implies a high number of false positive results. It is possible that a number of seroreverters tested false positive at study entry and were not infected initially when they entered the study. Thus, we cannot rule out that some changes in H pylori infection status may have arisen through the play of chance.
Several factors may have affected the reliability of the serology. Although sera were tested twice in the same laboratory there is still a risk of variation over time attributable to the serology test in itself. Sera from people who changed IgG antibody status or had significant increases in IgG amounts at follow up were re-tested pair wise on the same ELISA plate and used for comparisons. Freezing and thawing of sera have limited effect on IgG antibody measurements with ELISA techniques.40 The fact that IgG seroprevalences in general did not change within the observation period argues against any effect of long term freezing and thawing. The high reproducibility of antibody measurements inclines that single baseline measurements ofH pylori IgG antibody status is useful as a means for analytic studies on H pylorirelated diseases.
No standard definition exists of IgG seroreversion.41 We chose a fourfold decrease in baseline IgG antibody levels as evidence of IgG seroreversion as fourfold variations in antibody values are generally considered significant. However, it is unknown if fourfold decreases in antibody levels within the seropositive range or in the indeterminate region simply reflect biological fluctuations in the host's immunological activity or loss of infection.
Antibiotics were not used more often in seroreverters than in people who remained seropositive. Incidental eradication ofH pylori is probably unlikely.23 The use of antimicrobials, however, was only assessed in the five year period preceding follow up. Furthermore, no information was available on the duration of treatment or on which antimicrobials had been used.
Gastric atrophy could account for some cases of seroreversion.22 Seroreversion was less frequent in the older age groups. As the likelihood of gastric atrophy increases with the duration of the infection and thereby with age,22atrophic gastritis is probably not a valid explanation for the high seroreversion rate.
The applicability of this study would improve, if H pylori infection status was assessed with another diagnostic test. Large scale screening necessitates non-invasive screening methods. Although urea breath tests and western immunoblotting are considered more accurate than serology, their sensitivity and specificity do not reach 100 per cent.42 43
The prevalence of solitary increased IgM antibody levels toH pylori in this population was previously reported.30 Although the IgG seroconversion rate was significantly higher in people who had solitary increased IgM antibodies at study entry as compared with those who were seronegative, most participants with solitary increased IgM levels remained IgG seronegative. An isolated increase in IgM antibody, therefore, may not be a reliable marker for primary H pyloriinfection in Danish adults. It is also possible that some episodes of first time H pylori infection may have been cleared spontaneously without causing a detectable increase in IgG antibody levels.
Two findings in this study support this theory that the age related increase in the seroprevalence of H pyloriinfection seen in this and similar studies is attributable to a cohort phenomenon rather than a constant infection rate. Firstly, IgG seroprevalences remained stable between study entry and follow up. Secondly, the seroconversion rate does not account sufficiently for the increase in IgG seroprevalence with age. The prevalences of peptic ulcer disease and gastric cancer are declining in the Western world. More studies are needed to determine whether this is attributable to a decrease in the incidence of H pyloriinfections or to the gradual extinction of generations who have carried a high prevalence of H pyloriinfection throughout life.
In conclusion, the rate of IgG seroconversion in H pylori antibodies is low in Danish adults. As loss of the infection, evidenced by IgG seroreversion, was seen more often than seroconversion, it is possible that the prevalence ofH pylori infection will decline within the decades to come. This may subsequently bring on a parallel decline inH pylori induced disorders such as peptic ulcer, chronic gastritis and possibly gastric cancer.
References
Footnotes
-
Funding: the study was supported by The Danish Health Insurance Foundation (11/099–95), The Ingeborg Roikjer Foundation (9043), The Danish Medical Research Council (12–1844–1), The Danish Hospital Foundation for Medical Research, Region of Copenhagen, The Faroe Islands and Greenland (46–83), and the Else and Mogens Wedell-Wedellsborgs foundation (6686–1).
-
Conflicts of interest: none.