Article Text

Abstract
Objective: To determine whether adverse psychosocial and individual psychological factors increase the risk of pain across regional sites.
Methods: A prospective study was conducted of newly employed workers from 12 diverse occupational groups. Near to the beginning of subjects’ employment, details of work related psychosocial factors and individual psychological distress were obtained by means of a self completed questionnaire. Questionnaire follow up after 12 months provided data on these same exposures and ascertained pain at any of four anatomical sites: the low back, shoulder, wrist/forearm, and knee.
Results: Of the original 1081 subjects, 829 (77%) provided full details at the one year follow up. Psychosocial work demands and high levels of individual psychological distress were found to have a common effect across sites. Psychological distress was associated with a doubling of the risk of reported pain (odds ratio = 2.1, 95% confidence interval 1.6 to 2.7), while aspects of job demand, poor support from colleagues, and work dissatisfaction were all associated with increased odds of reported pain onset of between 1.4 and 1.7. These effects were almost all common across the four regional pain sites.
Conclusions: In cohorts of newly employed workers, certain work related psychosocial factors and individual psychological distress are associated with the subsequent reporting of musculoskeletal pain, and generally this effect is common across anatomical sites.
- epidemiology
- musculoskeletal pain
- occupational effect
- psychosocial factors
- GEE, generalised estimating equations
- GHQ, General Health Questionnaire
- ROC, receiver operating characteristic
Statistics from Altmetric.com
- GEE, generalised estimating equations
- GHQ, General Health Questionnaire
- ROC, receiver operating characteristic
Extensive research into the role of occupational factors in the development of musculoskeletal pain has been carried out.1,2 However, there are very few conclusive findings because of some common methodological flaws. Firstly, most studies have been cross sectional and therefore can neither determine the temporality of the relationship between workload and pain nor exclude recall bias. Secondly, studies have tended to be carried out amongst established workforces, where those who have developed symptoms might have left, thereby leaving behind a relatively healthy workforce—one aspect of the “healthy worker” effect, referred to as “secondary selection”. Thirdly, most studies have focused on a single occupation and therefore workers’ exposure to physical workload and work related psychosocial factors have been reasonably homogeneous. Their ability to find associations is limited. Further, this has reduced the external validity of the main study findings because conclusions can only be generalised to a specific occupational group.
Similarly, with very few exceptions,3,4 studies have focused on a single region of pain. Such concentration on individual sites may be inappropriate because pain at multiple sites is common, with no clear distinction between single and multiple site syndromes.5,6 It has been proposed that mechanical factors are important in the aetiology of acute regional pain, whereas psychosocial and individual psychological factors are important in the aetiology of persistent and generalised pain.3,7,8 We have previously reported that adverse work related psychosocial factors are cross sectionally associated with pain at several anatomical sites,9 but such studies cannot determine the temporal relationship between these.
We have therefore proceeded to conduct a prospective study to test the hypothesis that workplace psychosocial factors can predict the future onset of musculoskeletal pain, and that these effects are consistent across anatomical sites.
MATERIALS AND METHODS
The design was a one year, prospective, occupation based cohort study of newly employed workers. The study group comprised 1081 subjects across 12 occupational groups. The occupations were selected on the grounds that most workers would be taking up their first full time employment. They represented industries or occupations where high rates of musculoskeletal disorders had previously been identified, had reasonably stable workforces, and represented a range of occupations and industries. Only full time newly employed workers were eligible for recruitment in order to overcome the “healthy worker” effect. Subjects were invited to participate as close as practicable to the beginning of their employment or training, but not so near to the start that subjects were not familiar with what the job entailed. The median duration of employment reported by the subjects was eight months. The employers reported that no-one from the target population had left any one of the selected occupational groups owing to musculoskeletal pain before the start of data collection.
The sources for recruitment of subjects have been described previously,9 but details are reproduced in appendix 1.
Evaluation of exposure and pain status at job entry
All subjects at baseline were asked to complete a questionnaire on workplace psychosocial factors (work demands, job control, social support from colleagues, and job satisfaction) and psychological distress. These were regarded as exposures—that is, external stressors rather than personal factors. Subjects were asked to shade on a blank body manikin any pain experienced during the past month which had lasted for longer than 24 hours. By requiring subjects to recall pain which had lasted for a minimum of 24 hours, any trivial episodes will be excluded. If the pain was sited in one of the four predefined areas of interest it was classified accordingly.
The questions relating to psychosocial factors at work are reproduced in appendix 2. We measured work demands, level of job control, and support according to the model of Karasek.10 Those questions on work demands had originally been used in the West of Scotland-07 Study of Health in the Community11 and have more recently been shown to be related to the reporting of shoulder pain, low back pain, and forearm pain in population and workplace studies.12–14 Two questions were used to measure job control, relating to work autonomy and learning new things at work. The first question was developed solely for the purposes of the study. The second question has been demonstrated as being related to the reporting of back and limb disorders.15 One question was used to assess social support from colleagues, which was a modified version of a question used previously.15 In addition, a question was included to measure general job satisfaction. This question has previously been used in a population study, and been demonstrated to be associated with the reporting of low back pain.13
The 12 item General Health Questionnaire (GHQ) was included. This instrument has been tested for reliability, validity, and sensitivity as a screening tool for mental disorder and as a measure of short term psychological distress.16 Subjects score between 0 and 12, with high scores indicating high levels of distress.
Evaluation of outcome pain status and exposure at one year follow up
About 12 months later subjects were mailed a further questionnaire, with follow up of non-responders. Follow up included those subjects who had changed jobs. Subjects were asked to provide data relating to all exposures originally queried at the baseline stage. Subjects were asked to state if they had experienced pain in a predefined area for at least 24 hours during the past month. Four separate preshaded manikins were used (fig 1A–D) in order to define pain at the four anatomical sites of interest: low back, shoulder, wrist/forearm, and knee.

Preshaded manikins used to define pain at (A) low back; (B) shoulder; (C) forearm; and (D) knee.
Because exposure might have changed during the follow up year, all exposure data were available both at baseline and follow up. Each exposure was categorised into one of four groups: (1) those not reporting exposure at either baseline or follow up; (2) those reporting exposure at baseline only; (3) those reporting exposure at follow up only; and (4) those reporting exposure at both years. The cut off points used for each were as follows: (a) psychosocial work demands—those who stated that they were exposed at least half of the time; (b) job control—those who stated that they had control seldom or very seldom; (c) job satisfaction and satisfaction with support from colleagues—those who reported that they were dissatisfied or very dissatisfied; (d) psychological distress—those who scored above zero on the 12 item GHQ score (range of scores 0–12).
Statistical analysis
Analyses were carried out in STATA (version 6.0).17 All subjects who responded at both baseline and follow up were included in the analysis. Because some subjects were lost to follow up, there is the potential for bias because participation at follow up might be related to pain status. For example, those with pain might be more likely to take part. To overcome this problem, each subject who completed both phases of the study was allocated a sampling or probability weight (known as pweight in STATA). The weights were based on occupational group and baseline GHQ score. These factors were chosen because response rates varied between occupational groups (table 1) and with baseline GHQ score. This weight is calculated in such a way that all subjects in a particular stratum who completed a questionnaire at follow up would represent all subjects who were eligible to be surveyed in that particular stratum. For example, suppose that 70 of the original 100 subjects in a particular stratum who completed the questionnaire at baseline take part at follow up, then a sampling weight will be assigned to each of the 70 subjects such that the data acquired from them represents the data of all the eligible subjects in that particular stratum—that is, 100/70. In the current study such weighting had, however, little effect on estimates.
Response by occupational group
Multivariate profiles of pain responses (that is, presence/absence of reported pain at several different sites) were analysed through the use of generalised estimating equations (GEE).18 In brief, the site of the pain was treated as a within-subject factor called “site” (with the four levels representing the four regions). Exposure variables were between-subject factors or covariates. The basic model to predict presence of pain included the effect of site and the exposure covariates. Between-site associations within an individual subject are allowed for by a working correlation matrix.18 Firstly, site-specific effects were calculated. A Wald test was carried out to establish if there was a significant interaction between area of pain and effect of exposure—that is, if an exposure has a differential effect on the onset of pain at the four sites considered. The Wald statistic tests the homogeneity hypothesis that an effect measure is uniform across strata: small p values indicate that differential effects are likely. In cases where the effect was found to be common, this common effect estimate was obtained from the model. Further details of the use of GEE methods in this type of application are described by Everitt and Dunn.19
To determine the best predictors of pain, a forward stepwise regression model was applied. All factors under investigation were treated as potential candidates. The area under a receiver operating characteristic (ROC) curve was used to determine how good this model was at predicting those subjects with pain at follow up.
Associations are summarised as odds ratios with 95% confidence intervals. All relationships were adjusted for age and sex. Possibly, other factors apart from age and sex may act as confounders of the relationship between baseline exposures and pain at follow up. One such factor is baseline pain. Therefore pain at any one of the four anatomical sites reported at baseline during the past month was added to the final GEE model to determine if there was an interaction between baseline pain and any of the independent predictors of pain.
RESULTS
Of the 1081 participants at baseline (91% participation rate), 829 (77%) returned a completed questionnaire at follow up. Those workers who were not allocated a specific time by their employers to take part in the survey were most likely to fail to take part at baseline.20 The follow up rate varied between the different occupational groups (table 1). These differences partly reflect mobility of some occupational groups and the ease with which they could be contacted individually. The lowest response rate was found amongst the army infantry and the highest among the firefighters, police officers, army clerks, retail workers, and shipbuilders. As expected by the varying participation rates between occupational groups, response rates also varied across sex and age. Responders were more likely to be female compared with non-responders (34% of responders were female compared with 25% of non-responders, p<0.001) and more likely to be slightly older (median age 24 (interquartile range 21–29) v median age 23 (interquartile range 20–26), p<0.001).
Table 2 shows the unweighted prevalence of pain at follow up in the four anatomical sites of interest. Overall, low back pain was most common (prevalence of 26%) and forearm pain the least common (prevalence of 6%). Low back pain was most common amongst podiatrists. Both shoulder pain and knee pain were most common amongst army infantry. Retail workers reported the highest prevalence of forearm pain. Many subjects reported pain in more than one of the four anatomical sites of interest. Overall 344 (41%) of subjects reported pain in at least one region; of these, 217 (63%) subjects reported pain in a single region compared with 127 (37%) who reported pain in at least two regions. Only 7 (2%) reported pain in all four anatomical regions of interest.
One month prevalence of pain (measured using the preshaded manikin) by occupational group
Table 3 presents the relationship between the psychosocial factors, psychological distress, and the individual pain sites. In summary, most of the exposures resulted in an increased risk of onset of pain at each of the four anatomical sites. Only for “lack of control over work”, did the effect appear to vary by site—there was no relationship with low back pain. This one significant finding of heterogeneity, however, needs to be set in the context of evaluating a total of 32 such interactions. Table 4 provides estimates of the “common” effect for the remainder of exposures. At either baseline or follow up, high levels of psychological distress were associated with an approximate doubling of the risk of reporting pain at follow up. For the remainder of exposures relating to job demands, support, and satisfaction with work, the increased odds varied between 1.4 and 1.7.
The association between work related psychosocial factors, psychological distress, and individual sites of pain
The association between work related psychosocial factors and psychological distress and pain across four anatomical sites at year 1 of follow up
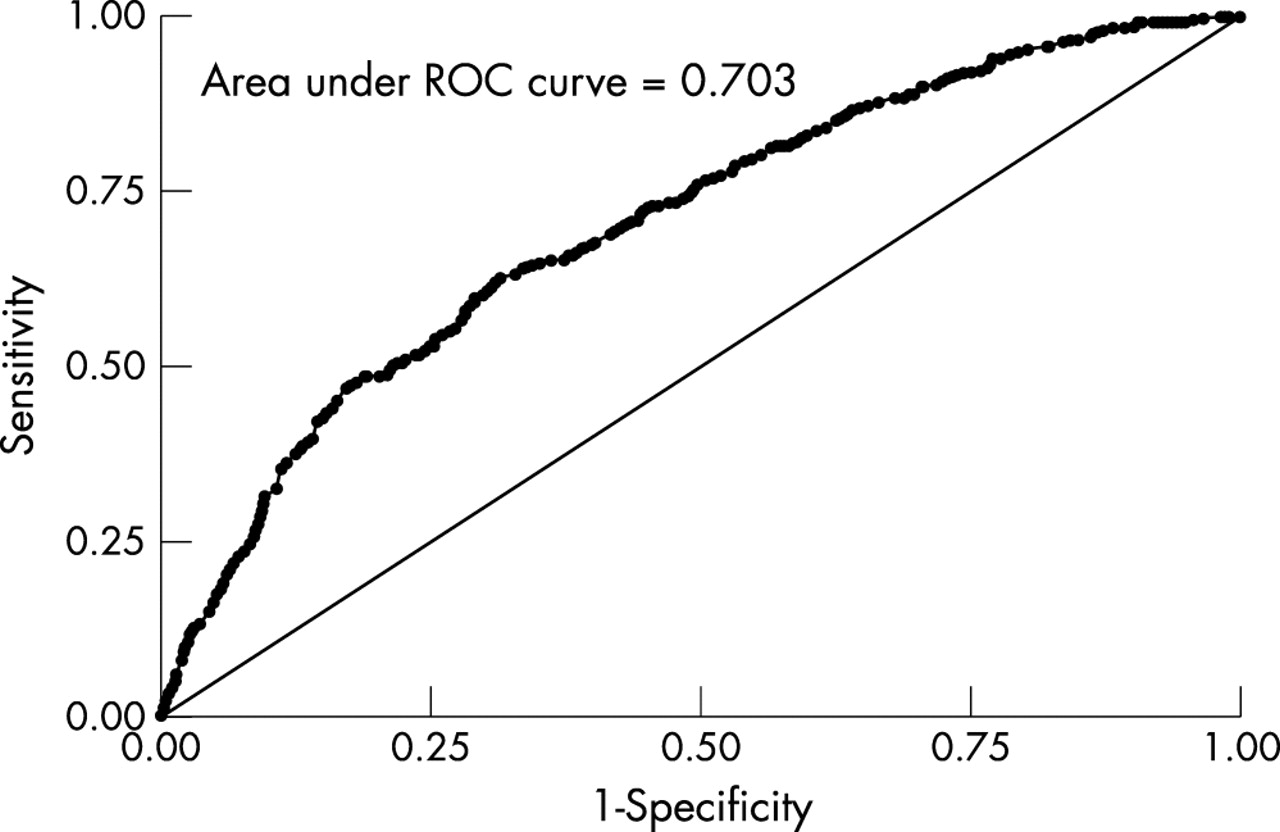
All the exposures examined were offered as candidates to a forward stepwise regression model. Four factors were retained in the model: psychological distress, hectic work, monotonous work, and lack of control over work (table 5). Because some subjects with pain at follow up already had pain at baseline while others did not, we evaluated whether predictors of pain at follow up differed in these two groups. When interaction terms between baseline pain and each of these factors were added to the model, none were significant. This implies that, for example, monotonous work at baseline was associated with pain at follow up irrespective of whether a subject had pain at baseline. The performance of the model was tested using an ROC curve (fig 2). The area under the curve was 0.70 (95% confidence interval 0.68 to 0.73), which indicates that the model correctly distinguished between an individual with pain at follow up and one without pain in 70% of cases.
Independent predictors of pain

{kind=link}
{kind=link}
Receiver operating characteristic (ROC) curve for the four independent predictors of pain.
DISCUSSION
In this study both adverse work related psychosocial factors and high levels of psychological distress at the early stages of employment increase the risk of reporting musculoskeletal pain one year later. Their effects were generally common across all four sites studied—namely, low back, shoulder, knee, and wrist/forearm. Only lack of job control had site-specific effects, and this has to be set in the context of one significant result from the many examined. It may be the case that this particular psychosocial factor does have an effect on specific sites, but without evidence from other studies, it is difficult to determine if this is the case.
This study adds to the body of evidence that adverse psychological and psychosocial factors can predict the future onset of musculoskeletal pain. Bongers et al in a detailed review of workplace studies concluded that these factors were important in the onset of several musculoskeletal pain syndromes,21 although they did not attempt to compare them across sites nor did they identify any studies which had done so. As far as we are aware, our study is the first formally to examine and compare the effect of work related factors across different sites of pain. Previous studies which have considered a number of sites of pain have tended to focus on the role of physical workload factors. In one such study of retired postal workers aged 70–75,4 it was found that associations between physical workload and musculoskeletal symptoms were specific across anatomical site. This study, like ours, found that there was clustering of musculoskeletal symptoms observed within individual subjects. In a recent study,14 work related psychosocial factors were found to predict future episodes of forearm pain. However, forearm pain most commonly occurred together with other regional pain sites, suggesting that these individual sites may share aetiological factors. In one study that considered the influence of work related psychosocial factors on a number of anatomical sites, Toomingas et al found that, among 358 workers from various occupations, high job demands and low social support were both associated with symptoms relating to the neck, back, and hip.8 Contrary to our findings, that study failed to show a relationship between work related psychosocial factors and shoulder or forearm symptoms. Another study found that among 902 blue and white collar workers at an engineering company, psychosocial factors were associated with symptoms throughout the body and concluded that there was a general musculoskeletal sensitivity to mental stress.22 Finally, distress and depression have been found to predict musculoskeletal morbidity at various anatomical locations, including the neck and shoulders, the low back, arms, and legs.22
It was important that the follow up rate was high because response at follow up may be influenced by pain status and/or exposure. Particular attention was paid to contacting not only those who remained in the same employment but also those who changed jobs. Those subjects who leave employment may be more likely to have had pain as a result of their work and therefore the loss of such subjects will introduce the “healthy worker” effect—namely, that those surveyed in work will be more healthy than those omitted from the survey. Response rates varied between occupational groups, but it is reassuring that those who were least likely to respond—namely, the army infantry and army officers, were least likely to change jobs during the first few years of employment. To compensate for the effect of losses at follow up, the data were weighted to reflect the distribution of occupational groups in the original cohort and the level of psychological distress at baseline.
The current study relied on self reported pain. Many previous studies have relied on diagnoses in order to determine outcomes, but these require subjects who seek medical attention or, alternatively, necessitate an examination of each subject. Because there is no clinical “gold standard” for defining these outcomes of interest, it is questionable whether diagnoses should currently be used in such epidemiological research. In an attempt to overcome this problem there has been some work validating self reporting of symptoms and, specifically, the use of manikins.23 These have been extensively used in population surveys and screening questionnaires,13,24,25 and their construct validity has been demonstrated.12,26
In a prospective study those subjects who report the outcome of interest at baseline are often excluded from further analysis so that the effect of exposure on subsequent development of the outcome during the follow up period can be studied. By contrast, all subjects were included in the current analysis regardless of baseline pain status. A major concern with such an approach is that those subjects with pain at baseline are more likely to report pain at follow up. Thus any association found between exposure at baseline and pain at follow up may partly occur owing to overreporting of psychosocial and psychological factors at baseline because of a changed perception among those with baseline pain. In the current study pain status at baseline was not found to influence the relationship between exposure and pain at follow up, suggesting that this was not the case.
Another unusual feature of our study was the use of information from both baseline and follow up in order to classify exposure. In a prospective study it is usual to examine the relationship between exposure at baseline and outcome at follow up. Many subjects in the current study changed exposure over the course of the year because although very few changed occupation, aspects of a person’s work changed as many were undergoing training at the start of the study. By using exposure at either or both years of the study as a measure of exposure this provided a more accurate measure. In a subsequent analysis where the effect only of exposure at both baseline and follow up (and hence by definition the exposure was reported before the onset of symptoms), the results were unchanged (data not shown).
In summary, this study is the first to attempt to overcome the “healthy worker” effect in a prospective study of musculoskeletal pain. It has shown that adverse psychosocial factors and psychological distress do predict future reported pain and that their effect is largely similar across anatomical site. These findings suggest that regional pain syndromes may share some aetiological factors and, particularly, that interventions aimed at these factors should not limit evaluation of outcome to a single body region. They should be considered for implementation and evaluation in that context.
Appendix 1: Sources for recruitment of subjects
The sources for recruitment of subjects were as follows:
-
Companies opening a new branch in the Greater Manchester area (northwest England), and employing an entire new workforce were contacted: two met these criteria for inclusion. The first, a supermarket, employed workers in a number of areas, including checkouts, service counters, a creche, and in general office, stock management, and shelf stacking duties. The second, a postal distribution centre, employed workers who were, in the main, responsible for unloading and loading trolleys of mail bags on and off trains and lorries. Other workers were employed in administrative duties and catering. All workers from both sources who were employed for the required number of hours (at least 20 per week) were invited to participate.
-
Service organisations which regularly recruited cohorts of new workers: three were recruited to the study. All full time paid firefighters from four local counties who were in their initial training period were invited to participate. A total of nine training intakes were included. One police force contributed all trainee police officers belonging to three training intakes. Three types of new army recruits were involved in the study: officers, infantry, and clerks. Thirty four officers were selected at random from each of three companies. Fifty infantry soldiers were selected at random from each of two battalions and all clerks enrolled on three training intakes were included.
-
One established organisation, a shipbuilding company, which was recruiting a large group of apprentices. These workers carried out construction and engineering tasks. All apprentices were invited to participate.
-
Students in their final year of a vocational course. All nursing students from one academic institution, all dental students from two academic institutions, all podiatry students from a further two academic institutions, and all forestry students enrolled on two courses at a specialised college were invited to participate.
Appendix B: Questions relating to psychosocial factors at work
-
How satisfied are you with your current job?
-
– Very satisfied
-
– Satisfied
-
– Neither satisfied nor unsatisfied
-
– Dissatisfied
-
– Very dissatisfied
-
-
Is your job boring, monotonous or repetitive?
-
– Never
-
– Occasionally
-
– About half of the time
-
– Always or most of the time
-
-
Is your work hectic/too fast?
-
– Never
-
– Occasionally
-
– About half of the time
-
– Always or most of the time
-
-
Does your work cause you stress/worry?
-
– Never
-
– Occasionally
-
– About half of the time
-
– Always or most of the time
-
-
Are you able to decide how to carry out your work?
-
– Very often
-
– Often
-
– Sometimes
-
– Seldom
-
– Very seldom
-
-
Do you learn new things at work?
-
– Very often
-
– Often
-
– Sometimes
-
– Seldom
-
– Very seldom
-
-
How satisfied are you with any support you receive from your workmates?
-
– Very satisfied
-
– Satisfied
-
– Neither satisfied nor unsatisfied
-
– Dissatisfied
-
– Very dissatisfied
-
Acknowledgments
We thank all the workers who participated and all those who allowed us access to each workforce. We also thank the following: Professor Nicola Cherry, who was involved in aspects of design and monitoring study conduct, and both Christina Pritchard and Stewart Taylor, who collected the data.