Article Text

Abstract
Objectives: To assess the occurrence and prognostic factors for the ability to maintain paid work in patients with rheumatoid arthritis (RA).
Setting: Inception cohort of patients with RA recruited from rheumatology departments in nine NHS Hospital Trusts in England.
Patients: All consecutive patients with RA of less than two years' duration, before any second line (disease modifying) drug treatment, and followed up for five years.
Methods: Clinical, laboratory, and radiological assessments, and all treatments were recorded prospectively using a standardised format at presentation and yearly.
Outcome measures: Changes in, and loss of paid work by five years' follow up.
Results: 732 patients completed the five year follow up. 353/721 (49%) were gainfully employed at the onset of RA, 211 (60%) were still working at five years, 104 (29%) stopped because of the disease, and 31 (9%) retired for reasons other than RA. Work disability at five years was more likely in manual workers (odds ratio (OR) 2.3, 95% confidence interval (CI) 1.4 to 3.8) and worse baseline Health Assessment Questionnaire (HAQ>1.5, OR 2.26, 95% CI 1.38 to 3.7). In combination with other baseline variables (erythrocyte sedimentation rate, sex, age of onset, and radiological erosions), employment outcome was predicted in 78% using multivariate analysis.
Conclusions: Nearly half of the patients with RA were in paid employment at onset, work disability was an adverse outcome for a third of these patients by five years, and manual work and high baseline HAQ were important predictors for this. These details are likely to be useful to clinicians, health professionals, and patients in order to plan medical, orthopaedic, and remedial treatments in early RA. Future disease modifying treatments could be compared with this cohort of patients who were treated with conventional second line drugs.
- rheumatoid arthritis
- work
- early rheumatoid arthritis
- functional outcome
- Health Assessment Questionnaire
- CI, confidence interval
- DMARD, disease modifying antirheumatic drug
- ERAS, Early Rheumatoid Arthritis Study Group
- ESR, erythrocyte sedimentation rate
- HAQ, Health Assessment Questionnaire
- OR, odds ratio
- PWD, permanent work disability
- RA, rheumatoid arthritis
Statistics from Altmetric.com
- CI, confidence interval
- DMARD, disease modifying antirheumatic drug
- ERAS, Early Rheumatoid Arthritis Study Group
- ESR, erythrocyte sedimentation rate
- HAQ, Health Assessment Questionnaire
- OR, odds ratio
- PWD, permanent work disability
- RA, rheumatoid arthritis
The course of rheumatoid arthritis (RA) varies greatly from mild, even self limiting, disease to a severe destructive form within a few years. Outcome in RA has been described mainly in terms of mortality, radiographic damage, cost, and functional disability scores,1 which has been the subject of an extensive review.2 Permanent work disability (PWD) has considerable impact on patients' lives, family income, and indirect costs for society. Information on this in RA has come mainly from retrospective or cross sectional studies in America and northern Europe, which have reported variable results. The incidence of work disability in these studies varies from 29% to 50% by around five years of disease duration.39 A few prospective studies from the early stages of RA have been carried out, mainly in northern Europe, and although many of these have been limited by small sample sizes and variable follow up, a number of different predictors for work disability have been identified.1019 Despite the differences in study designs, healthcare and social security arrangements, and methods for ascertaining work disability in RA in different countries and over time, most prospective studies have reported physically demanding jobs and severity of RA as important risk factors for work loss. The point at which this occurs in the course of RA does vary between studies, and another major difference between all cross sectional and prospective reports is the relative importance of disease characteristics compared with socioeconomic backgrounds and the physical nature of, and attitudes to, work.
We have previously reported on five year outcomes from the Early RA Study (ERAS), which included the occurrence of work disability in nine regions in England18 and the importance of socioeconomic background.20 An important finding from the only other UK study, based in Norfolk,19 was lack of evidence that earlier intervention with second line drugs reduced work disability rates, in contrast with a report indicating that early treatment was protective.10 Information which would be important for planning future healthcare services in the UK includes greater detail about reasons for loss of work or changes in employment during the first few years of RA, regional variations, and whether early recognition and any remedial interventions can be effective. This paper reports in greater detail on work loss due to RA in the first five years and on predictive factors for work disability in ERAS patients.
PATIENTS, MATERIALS, AND METHODS
The entry criteria and standardised assessments made by trained metrologists have been described in previous reports from this group.18,20 Briefly, consecutive patients with RA were recruited from rheumatology outpatient clinics in nine different districts of England if symptoms of RA had lasted for less than two years and second line drug treatment had not been used. Patients who did not fulfil the 1987 revised American College of Rheumatology criteria for RA21 continued to be followed up and subjected to subgroup analysis. Only patients who completed five years' follow up have been included in this analysis. Details of differences between centres have been reported previously.18
Yearly assessments included two articular indices, one based mainly on tenderness, the Ritchie articular index,22 and the other on swelling, as previously described,18 visual analogue pain scale, functional grade,23 the disability index of the modified Stanford Health Assessment Questionnaire (HAQ),24 erythrocyte sedimentation rate (ESR), and rheumatoid factor (RF). ERAS started in 1987 and did not include all the components needed to calculate recently recommended disease activity scores and response criteria, but did for the disease activity score based on three variables: Ritchie articular index, swollen joint count, and ESR.25
Also recorded were all comorbid conditions, including any extra-articular manifestations of RA. Socioeconomic information included social class, educational level, and Carstairs deprivation index, as previously described.20 Details of paid employment were defined by economic activity.26 Also recorded were details of home support, house alterations, and number and type of social security and employment allowances (mobility, attendance, daily living, incapacity, care, and disability allowances, income support, and unemployment benefits). The main outcome was any major change in paid employment from baseline and the reasons for this. This included alteration in hours worked, time off work, and PWD, defined as when a patient leaves the paid labour force because of ill health. For purposes of analysis, the type of work has been grouped into mainly manual, semi-manual, semi-sedentary, mainly sedentary, and part time (<5 hours) or full time (≥5 hours).
Treatment
All centres followed the framework of the published UK guidelines for management of RA,27 which includes the provision of therapy services, appropriate orthopaedic interventions, and sequential use of second line or disease modifying antirheumatic drugs (DMARDs), together with measures to relieve symptoms, including judicious use of steroids. Combination treatment was used in severe and non-responsive RA. The DMARDs used were chosen according to the doctor's preference, although dosage schedules employing graduated regimens were previously agreed according to standard practice for each drug.
Various arrangements were in place in all ERAS centres to deal with work related problems, but not specifically for patients with early RA who were working but beginning to experience problems at work. These varied in the use of physiotherapy and occupational therapy departments, rehabilitation units, and occupational physicians. The last two were usually only used once patients had become work disabled. Two hospitals had physiotherapists or occupational therapists who had special interests in this field and were able to assess patients at the work place.
Statistical analysis
Summary statistics have been used to demonstrate differences in clinical and laboratory features between outcomes at five years. Median values with interquartile ranges are shown for continuous variables and tested for significance with the Mann-Whitney test. For categorical variables odds ratios (OR) with 95% confidence intervals (CI) were calculated. Logistic regression (for an outcome of work loss by five years) and Cox regression (with time to disability as a response variable) were both used to predict work disability from a number of clinical and laboratory measurements at baseline and at one year.
Patient sample
The clinical characteristics of this cohort of 732 patients followed up for five years have been described in detail elsewhere.18 The median duration of symptoms of RA before presentation to rheumatology departments and entry to the study was six (4–11) months. A total of 617 (84%) patients received at least one DMARD at a median of two months from first presentation (68% within three months and 87% by 12 months). Of the patients treated with DMARDs, 49.5% required more than one drug, and overall use of these drugs was sulfasalazine (45%), methotrexate (17%), intramuscular gold (15%), d-penicillamine (10%), antimalarial drugs (5%), and various others (8%). Oral steroids in doses of 7.5 mg daily or more for 12 months or more were used in 16%.
RESULTS
Employment details at baseline
At presentation, 368 (52%) patients were not in paid employment: 166 (23%) were housewives, 188 (26%) had already retired, 12 (1.6%) were unemployed, and two were students. Table 1 gives demographic and baseline clinical features by occupational status. This shows little variation between working and non-working patients, except that younger patients and more men were working, the latter mainly in manual type jobs. Of those working, the majority were in full time work (n=285, 81%). Part time workers were more likely to be in sedentary (14.5%) rather than manual jobs (10%). The 15 employed patients who were in functional grade III/IV at presentation were temporarily off work because of RA at this time. Employment rates varied from 34% to 59% between ERAS centres, explained largely by differences in age, sex, and socioeconomic background.20 Occupational status was missing in 11 patients (all <65 years, five close to retirement age). Thus the main analysis concerns the 353 patients who were working at baseline.
Work status and clinical features at baseline*
Job status at five years
By five years' follow up, 211 (60%) remained working in varying capacities; 188 remained in the same job, although 27 had reduced their hours of work, 15 changed to lighter work, and eight took more manual jobs. A total of 142 patients stopped working for the following reasons: age related retirement in 25 (18%), redundancies, social or personal reasons in six (4%), and RA in 80 (56%). In a further 24 (17%), several factors including RA were responsible for early retirement, the others being comorbidity (n=16) or social reasons (n=8). Forty per cent of patients overall had some time off work (mean number of months was 5.1).
Time from presentation of RA to loss of employment
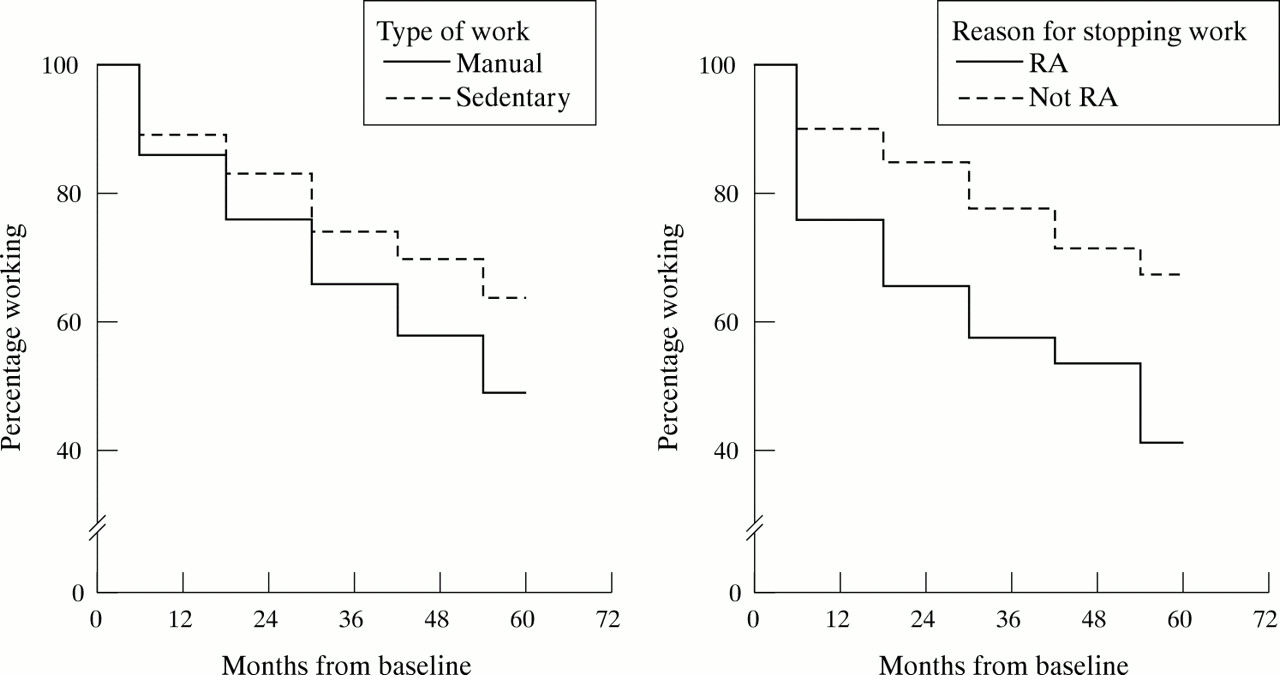
Figure 1 shows that the rate of job loss occurred earlier in manual than in non-manual workers, but at a regular steady rate, and RA related work loss occurred much earlier than job loss for other reasons. Of the 368 patients not working at presentation, 13 had lost their jobs as a result of RA in the time from the onset of RA and before presentation to rheumatology departments. Comorbidity was a factor in five of these. Another eight patients not working for other reasons (all were housewives and mothers) were working by the five year follow up.

Patients still working at 0–60 months.
Risk factors for work disability
We have attempted to deal with two issues. Firstly, the relative importance of the severity of RA and type of job as factors contributing to work disability, an issue which has not been fully resolved on review of previously reported rheumatological studies. Secondly, whether it was possible to predict work disability over five years' follow up from clinical parameters at baseline.
Severity of RA as a risk factor
Figure 2 shows serial HAQs over five years in groups based on reasons for PWD. Patients who stopped work because of RA already had worse HAQs at baseline, and these did not stabilise with time as in other groups. Patients who stopped working because of RA were older, and had higher HAQ, joint and pain scores over time than those who remained employed (Mann-Whitney, p<0.0000 for all these variables), and higher ESRs (p<0.0005) (table 2). Table 3 shows categorical variables at the time of PWD for these groups. The results indicate the importance of persistence and severity of RA as well as manual work and less favourable socioeconomic backgrounds on loss of work within the first five years.
Work disability by five years. Clinical features according to reasons for permanent work disability (PWD). Results are shown as median (IQR)
Clinical features at five years by reasons for work disability

{kind=link}
{kind=link}
Change in HAQ over five years according to reasons for work disability.
Predicting work disability using baseline clinical features
Univariate analysis
Job loss due to RA was more likely in those with a high ESR (OR 2.37, 95% CI 1.4 to 3.9); HAQ >1.5 (OR 2.26, 95% CI 1.38 to 3.7); presence of erosions (OR 2.09, 95% CI 1.19 to 3.64); manual type work (OR 2.97, 95% CI 1.26 to 6.9).
Multivariate analysis
Multivariate analysis was performed using both logistic and Cox regression with the following baseline variables: type of employment, sex, age of onset, radiographs of hands and feet, functional grade, HAQ, rheumatoid factor, joint scores, and ESR. Among those working, there were 245 patients with non-missing values for the above predictors who were below retirement age (65 for men, 60 for women) at five years or at reaching work disability, whichever came first.
Logistic regression selected HAQ (p=0.0344), ESR (p=0.0027), age at onset (p=0.0001), radiographs (p=0.0739), sex (p=0.0368), and type of employment (p=0.0032) as predictors of PWD (table 4). This model resulted in correct prediction overall of 77.9%, specificity 89.7% and sensitivity 53.7%. The positive predictive value was 72%, and negative predictive value 80%. As can be seen from table 4, manual jobs carried significant risk of PWD, as well as an HAQ of ≥1. A raised ESR was also highly significant, as were age and sex effects. The presence of radiographic erosions was included in the list of predictors, although only marginally significant.
Logistic and Cox regression
To test the validity of the selected model, we split the data randomly into two subsamples (60% and 40%). Overall correct prediction was 77.21% for the training subsample, and 76.15% for the testing sample. These results confirm that the six predictors which we have selected are relevant for prediction of PWD. When stepwise logistic regression with the above predictors both at baseline and at one year was used, the final model selected was as described above except for HAQ at one year. Such a model had overall prediction quality of 80.17% (random split resulted in 78.06% v 72.22% for the two subsamples). The HAQ at one year was a slightly better predictor than HAQ at onset, but the model was not overwhelmingly better.
We also performed Cox regression, with time to disability as the response variable (table 4). The same predictors were chosen: HAQ categories (p=0.0130), ESR category (p=0.0241), age at onset (p=0.0001), radiographs (p=0.0182), sex (p=0.0706), and type of employment (p=0.0092). All the predictors were essentially the same for the Cox regression as for the logistic regression, although sex was only marginally significant in the Cox regression.
DISCUSSION
The clinical profiles of patients with early RA given conventional drug treatment in this study showed that nearly half were in paid employment at onset, and most of these were still working at five years (60%). However, a third of patients lost their jobs by five years because of RA, often early on. Thirteen patients were already work disabled by the first presentation to rheumatology clinics, a lower proportion than in some studies, which reported 42%14 and 18%.19 Severity of disease, manual work, age of onset, and less favourable socioeconomic background were important factors for work disability. In our patients the most important factors at baseline for PWD identified by logistic regression were manual-type work and HAQ >1.5. In combination with other independent clinical features, correct prediction was 78%. Comorbid conditions in addition to RA were important factors in 16 patients, a feature not reported in other studies. Some of the differences seen between centres could be explained by population and socioeconomic differences in employment status. We have previously reported the adverse effect of lower socioeconomic status on functional scores in RA.20
Work disability rates vary considerably in prospective studies,1019 a subject of recent reviews.19,28 However, of those prospective studies which recruited patients in the past 10 years, many reported similar rates of work disability as our study of around 30–40% by five years. Severity of RA and heavy work, which we found to be the most important factors for work disability, were reported in only some studies. An unresolved issue in published rheumatological reports for risk factors for work disability is the relative importance of the severity of RA compared with socioeconomic background and type of work, for which quite different management strategies are required. From retrospective surveys in America, Yelin et al identified social and work place factors,3 and Callahan et al reported that socioeconomic and functional measures had the greatest impact on work loss in patients with RA.5 Of 119 patients surveyed with a mean disease duration of nearly two years in the Netherlands,8 40% had PWD because of RA, and this was dependent on clinical and laboratory features of disease severity and on educational level. Reisine et al reported that clinical features rather than physical demands of the job were more important for work status in 392 patients (61% with RA >5 years).6 Wolfe and Hawley found persistent abnormalities of ESR, HAQ, and pain over time were the best predictors of PWD in 456 patients who had very variable disease duration at the time of study.7 In a placebo controlled drug trial in early RA, Borg et al described younger age, low HAQ and joint score, white collar work, and self employment as protective at two years.10
Examining predictive factors at presentation, Eberhardt and Fex reported that in a Swedish inception cohort of 144 patients, one third stopped working and 16% changed or reduced their work arrangements by the second year of follow up.12 No sociodemographic features had predictive value, but initially high HAQ and physically demanding employment carried a worse prognosis for work loss at two years,12 and HAQ, age and educational level at four years.14 Kaarela et al and Jantti et al, both reported on an inception cohort in Finland, but at different follow up stages, and showed that severity of disease was the main cause of work disability, although significantly smaller numbers of patients with arduous jobs were able to continue.11,15 In their series of 103 patients, work disability increased from 31% at one year to 80% by 20 years, because of RA in 42/66 at this time. Mau et al reported 37% PWD in 73 patients (mainly by three years) followed up prospectively for four to eight years in northern Germany.13 Predictors for PWD were older age, high ESR, and more physical type of work. Barrett et al found that one third of 160 patients in a community based study in one region in England had stopped working by around five years.19 Although type of employment and age were identified as additional factors in multivariate analysis, only baseline HAQ was a significant predictor for this. Sokka et al reported that heavy work was the strongest independent risk factor for PWD.16
The main strengths of this study include recruitment from the earliest stages of RA before use of second line drugs, the relatively few exclusion criteria (which are so restrictive in clinical trials), thus reflecting actual clinical practice, yearly standardised assessments, and good follow up. Possible sources of bias, including treatment effects and left and right censoring, have been previously described.18 Although the effects of different DMARDs cannot be accounted for, our patients were being treated early in a conventional manner.
Clearly, arrangements for patients heading for work disability were not geared to a rapid response in the nine hospitals taking part, and it is likely that this reflects similar practice elsewhere in the UK. Nor was there close collaboration between rheumatologists and occupational physicians, and all centres agreed that this aspect of the rheumatology service could be improved. The identification of factors indicative of poor outcome early in the course of RA is crucial for tailoring treatment and supporting coping mechanisms.29 There are a number of potential opportunities for interventions to prevent work disability, apart from controlling disease with disease modifying drugs. These include remedial treatment and rehabilitation,28 and with predictive factors in mind, should be considered early and before work loss. The latter is often an irreversible outcome and not always in the patients' interest, whereas the disease course and severity may be improved by stopping work. Closer communication between rheumatologists, health professionals, occupational physicians, and employers would seem to be the most obvious requirement. The measures we have identified which predict this outcome in 78% are simple and could be used routinely in early RA to help this process.
Acknowledgments
The ERAS group was funded by the Arthritis Research Campaign (ARC) and BUPA Research Foundation. The ERAS coordinator is funded by an ARC Academic Secretary grant. The authors thank Cathy Mayes, Annie Seymour, Terry McCourt, Lynn Hill, Linda Waterhouse, Hazel Tait, Dora White, Sue Stafford, Helen Dart, Cathy Boys, and Alison Kent for their invaluable metrology work.
References
Footnotes
-
The authors are all members of the Early Rheumatoid Arthritis Study Group, ERAS, UK.