Does Primary Care Mental Health Resourcing Affect the Use and Costs of Secondary Psychiatric Services?


Abstract
:1. Introduction
2. Experimental Section
3. Results and Discussion
3.1. Results


{kind=link}
{kind=link}
{kind=link}
| Variable | Primary Care Mental Health Nurses | Outpatient Visits | Inpatient Days | Admission Rate | Length of Stay | Costs | MHI | Unemployment Rate | Average Income | Single Households |
|---|---|---|---|---|---|---|---|---|---|---|
| Primary care mental health nurses | 1 | |||||||||
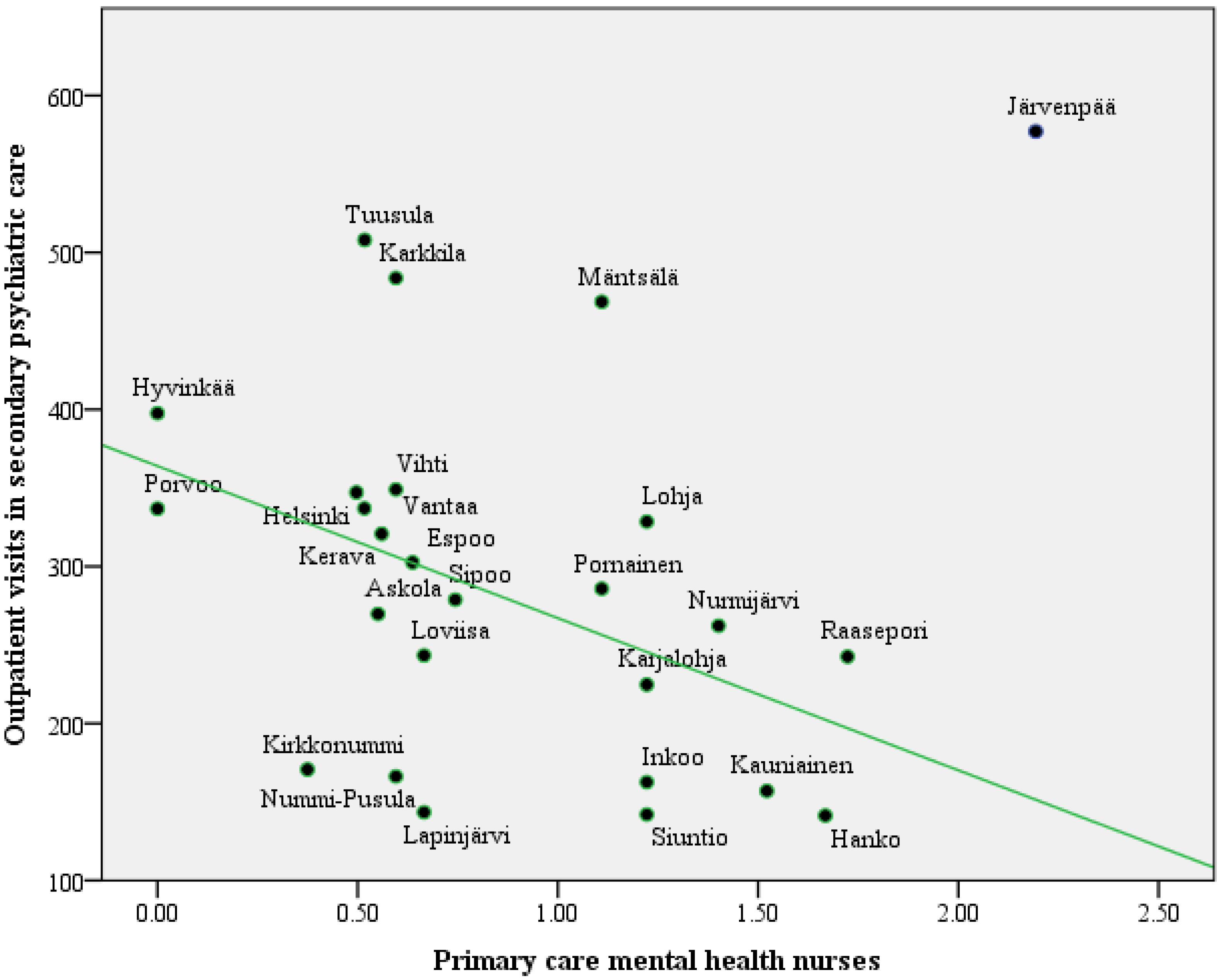
| Outpatient visits in secondary psychiatric care | −0.39 * | 1 | ||||||||
| Psychiatric inpatient days | 0.19 | 0.41 * | 1 | |||||||
| Psychiatric hospital admissions | 0.074 | 0.36 | 0.68 ** | 1 | ||||||
| Length of hospital stay | 0.07 | −0.007 | 0.21 | −0.55 ** | 1 | |||||
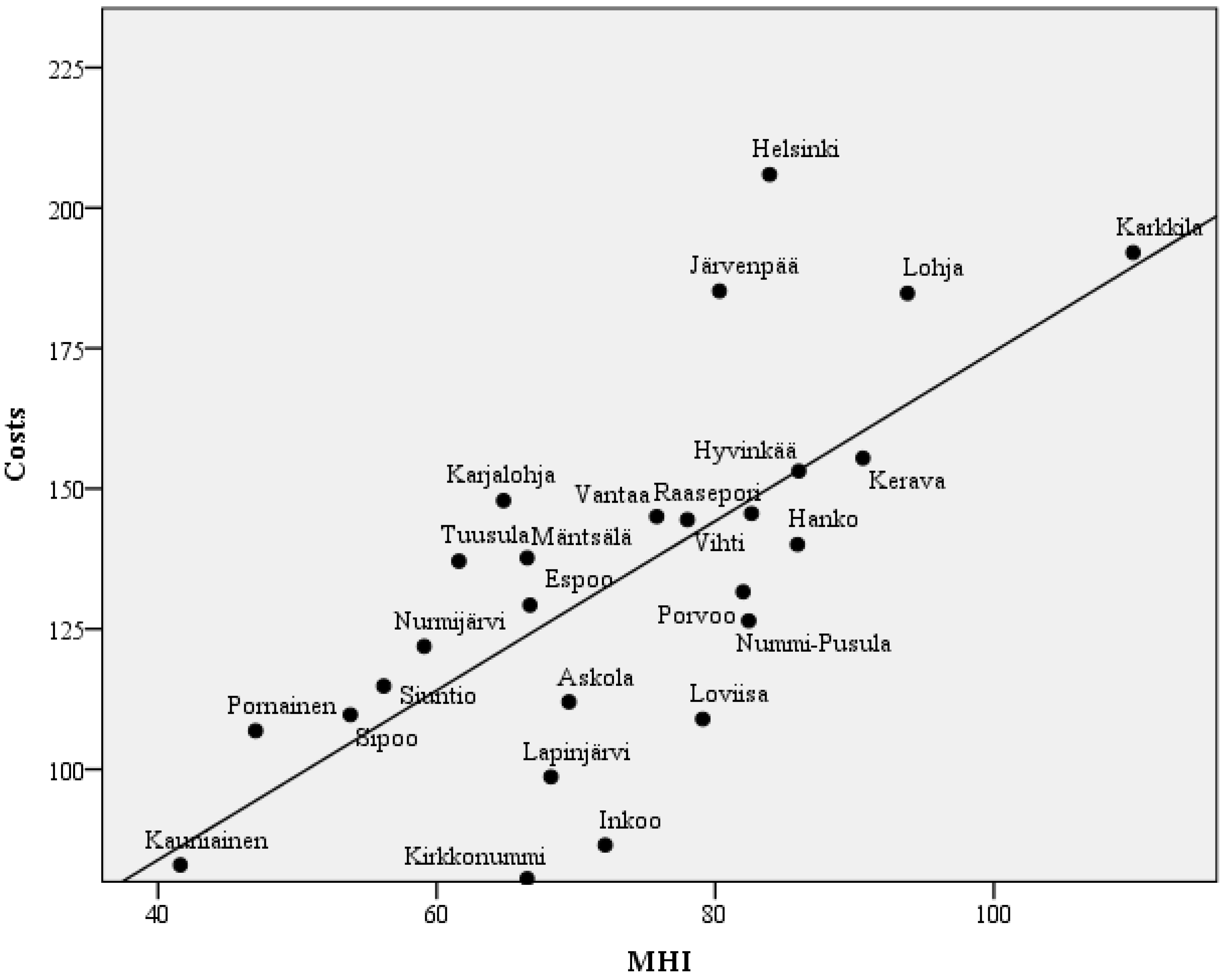
| Costs of secondary psychiatric care | −0.075 | 0.63 ** | 0.83 ** | 0.73 ** | −0.041 | 1 | ||||
| MHI | −0.22 | 0.29 | 0.39 | 0.62 ** | −0.39 * | 0.69 ** | 1 | |||
| Unemployment rate | −0.19 | 0.06 | 0.37 | 0.54 ** | −0.31 | 0.46 * | 0.64 ** | 1 | ||
| Average income | −0.079 | 0.17 | −0.065 | −0.43 * | 0.57 ** | −0.18 | −0.45 * | −0.66 ** | 1 | |
| Percentage of single households | −0.056 | 0.11 | 0.47 * | 0.51 ** | −0.16 | 0.61 ** | 0.75 ** | 0.82 ** | −0.49 * | 1 |
| Education | −0.096 | 0.17 | −0.088 | −0.44 * | 0.56 ** | −0.13 | −0.37 | −0.66 ** | 0.95 ** | −0.41 |

| Independent Variables | Inpatient Days | Admission Rate | ||||
|---|---|---|---|---|---|---|
| B | se | p | B | se | p | |
| Intercept | −23.27 | 53.23 | 0.666 | −5.06 | 3.13 | 0.12 |
| MHI | 1.23 | 0.67 | 0.077 | 0.15 | 0.04 | 0.001 |
| Primary care mental health nurses | 44.23 | 17.94 | 0.022 | 2.29 | 1.06 | 0.041 |
| Outpatient visits in secondary psychiatric care | 0.16 | 0.08 | 0.074 | 0.00 | 0.01 | 0.485 |

3.2. Discussion
3.3. Strengths and Limitations
4. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Thornicroft, G.; Tansella, M. The balanced care model: The case for both hospital- and community-based mental healthcare. Brit. J. Psychiat. 2013, 202, 246–248. [Google Scholar] [CrossRef] [PubMed]
- WHO Regional Office for Europe. European Health for all Database (HFA-DB), 2014. Available online: http://www.euro.who.int/en/data-and-evidence/databases/european-health-for-all-database-hfa-db (accessed on 18 March 2014).
- Psykiatrinen erikoissairaanhoito 2012. National Institute of Health and Welfare. Official Statistics of Finland. Psychiatric Specialist Medical Care 2012. Available online: http://www.julkari.fi/bitstream/handle/10024/114909/Tr05_14.pdf?sequence=1 (accessed on 18 March 2014).
- Westman, J.; Gissler, M.; Wahlbeck, K. Successful deinstitutionalization of mental health care: Increased life expectancy among people with mental disorders in Finland. Eur. J. Public Health 2012, 22, 604–606. [Google Scholar] [CrossRef] [PubMed]
- Pirkola, S.; Sohlman, B.; Heilä, H.; Wahlbeck, K. Reductions in postdischarge suicide after deinstitutionalization and decentralization: A nationwide register study in Finland. Psychiatr. Services 2007, 58, 221–226. [Google Scholar] [CrossRef]
- Pirkola, S.; Sund, R.; Sailas, E.; Wahlbeck, K. Community mental-health services and suicide rate in Finland: A nationwide small-area analysis. Lancet 2009, 373, 147–153. [Google Scholar] [CrossRef] [PubMed]
- Hämäläinen, J.; Isometsä, E.; Sihvo, S.; Pirkola, S.; Kiviruusu, O. Use of health services for major depressive and anxiety disorders in Finland. Depress. Anxiety 2008, 25, 27–37. [Google Scholar]
- Kessler, R.C.; Demler, O.; Frank, R.G.; Olfson, M.; Pincus, H.A.; Walters, E.E.; Wang, P.; Wells, K.B.; Zaslavsky, A.M. Prevalence and treatment of mental disorders, 1990 to 2003. N. Engl. J. Med. 2005, 352, 2515–2523. [Google Scholar] [CrossRef] [PubMed]
- Wang, P.S.; Aguilar-Gaxiola, S.; Alonso, J.; Angermeyer, M.C.; Borges, G.; Bromet, E.J.; Bruffaerts, R.; de Girolamo, G.; de Graaf, R.; Gureje, O.; et al. Use of mental health services for anxiety, mood, and substance disorders in 17 countries in the WHO World Mental Health Surveys. Lancet 2007, 370, 841–850. [Google Scholar] [CrossRef] [PubMed]
- Archer, J.; Bower, P.; Gilbody, S.; Lovell, K.; Richards, D.; Gask, L.; Dickens, C.; Coventry, P. Collaborative care for depression and anxiety problems. Cochrane Database Syst. Rev. 2012, 10. [Google Scholar] [CrossRef]
- Woltmann, E.; Grogan-Kaylor, A.; Perron, B.; Georges, H.; Kilbourne, A.M.; Bauer, M.S. Comparative effectiveness of collaborative chronic care models for mental health conditions across primary, specialty, and behavioral health care settings: Systematic review and meta-analysis. Amer. J. Psychiat. 2012, 169, 790–804. [Google Scholar] [PubMed]
- Williams, J.W., Jr.; Gerrity, M.; Holsinger, T.; Dobscha, S.; Gaynes, B.; Dietrich, A. Systematic review of multifaceted interventions to improve depression care. Gen. Hosp. Psychiat. 2007, 29, 91–116. [Google Scholar] [CrossRef]
- Gilbody, S.; Whitty, P.; Grimshaw, J.; Thomas, R. Educational and organizational interventions to improve the management of depression in primary care: A systematic review. JAMA 2003, 289, 3145–3151. [Google Scholar] [CrossRef] [PubMed]
- Gilbody, S.; Bower, P.; Whitty, P. Costs and consequences of enhanced primary care for depression systematic review of randomised economic evaluations. Brit. J. Psychiat. 2006, 189, 297–308. [Google Scholar] [CrossRef] [PubMed]
- Jacob, V.; Chattopadhyay, S.K.; Sipe, T.A.; Thota, A.B.; Byard, G.J.; Chapman, D.P. Economics of collaborative care for management of depressive disorders: A community guide systematic review. Amer. J. Prev. Med. 2012, 42, 539–549. [Google Scholar] [CrossRef]
- Vuorilehto, M.; Kuosmanen, L.; Melartin, T. Depressiohoitajan työ on kohdallaan Vantaan kolmikantamallissa. Finn. Med. J. 2008, 63, 190–192. (In Finnish) [Google Scholar]
- Tuulari, J.; Aromaa, E. Depressiohoitajamallilla saadaan tulosta pohjanmaalla (Depression nurse model is effective in Ostrobohnia). Finn. Med. J. 2008, 63, 194–195. (In Finnish) [Google Scholar]
- Reports 2009:5 of the Ministry of Social Affairs and Health. Plan for Mental Health and Substance Abuse Work. Proposals of the Mieli 2009 Working Group to Develop Mental Health and Substance Abuse Work until 2015. Available online: http://www.stm.fi/en/publications/publication/-/_julkaisu/1385226 (accessed on 18 August 2014).
- Käypä Hoito Depressio. Current Care Guideline. Available online: http://www.kaypahoito.fi/web/kh/suositukset/suositus?id=hoi50023 (accessed on 17 February 2014). (In Finnish)
- Reijneveld, S.A.; Schene, A.H. Higher prevalence of mental disorders in socioeconomically deprived urban areas in the Netherlands: Community or personal disadvantage? J. Epidemiol. Community Health 1998, 52, 2–7. [Google Scholar] [CrossRef]
- Lorant, V.; Deliege, D.; Eaton, W.; Robert, A.; Philippot, P.; Ansseau, M. Socioeconomic inequalities in depression: A meta-analysis. Amer. J. Epidemiol. 2003, 157, 98–112. [Google Scholar] [CrossRef]
- Lorant, V.; Croux, C.; Weich, S.; Deliege, D.; Mackenbach, J.; Ansseau, M. Depression and socio-economic risk factors: 7-year longitudinal population study. Brit. J. Psychiat. 2007, 190, 293–298. [Google Scholar] [CrossRef] [PubMed]
- The Refinement Project Group. REFINEMENT Work Package 9: Building Optimal Models of Mental Health Care Financing. 2013. Appendix to the REFINEMENT Decision Support Toolkit (DST) Manual (Manuscript). Available online: http://rpc.spsichiatria.univr.it/refinementproject/ (accessed on 17 March 2014).
- Salvador-Carulla, L.; Ruiz, M.; Romero, C.; Poole, M. European Service Mapping Schedule—Revised. Finnish. Eurooppalainen Mielenterveyspalvelujen Kartoittamistyökalu. 2012. Available online: http://urn.fi/URN:ISBN:978-952-245-714-1 (accessed on 18 August 2014).
- Salvador-Carulla, L.; Alvarez-Galvez, J.; Romero, C.; Gutierrez-Colosia, M.R.; Weber, G.; McDaid, D.; Dimitrov, H.; Sprah, L.; Kalseth, B.; Tibaldi, G.; et al. Evaluation of an integrated system for classification, assessment and comparison of services for long-term care in Europe: The eDESDE-LTC study. BMC Health Serv. Res. 2013, 13. [Google Scholar] [CrossRef] [Green Version]
- Salvador-Carulla, L.; Tibaldi, G.; Johnson, S.; Scala, E.; Romero, C.; Munizza, C.; CSRP Group; RIRAG Group. Patterns of mental health service utilisation in Italy and Spain—An investigation using the European service mapping schedule. Soc. Psychiatry Psychiatr. Epidemiol. 2005, 40, 149–159. [Google Scholar]
- Salvador-Carulla, L.; Poole, M.; Bendeck, M.; Romero, C.; Salinas, J.A. Bridging knowledge in long term care 2009: Coding long-term care services—eDESDE-LTC. Int. J. Integr. Care. April–June 2009, 9, p. e64. Available online: http://www.ncbi.nlm.nih.gov/pmc/articles/PMC2707571/ (accessed on 22 August 2014).
- Johnson, S.; Kuhlmann, R.; EPCAT Group; European Psychiatric Assessment Team. The European Service Mapping Schedule (ESMS): Development of an instrument for the description and classification of mental health services. Acta Psychiatr. Scand. Suppl. 2000, 405, 14–23. [Google Scholar]
- National Institute of Health and Welfare, SOTKAnet Statistics and Indicator Bank. Available online: http://uusi.sotkanet.fi/portal/page/portal/etusivu/hakusivu?group=359 (accessed on 25 April 2014).
- Mental Health Index, not Age-Standardised (ID: 254). Available online: http://uusi.sotkanet.fi/portal/page/portal/etusivu/hakusivu/metadata?type=I&indicator=254 (accessed on 18 August 2014).
- Wilkinson, J.; Bywaters, J.; Simms, S.; Chappel, D.; Glover, G. Developing mental health indicators in England. Public Health 2008, 122, 897–905. [Google Scholar] [CrossRef] [PubMed]
- Tibaldi, G.; Munizza, C.; Pasian, S.; Johnson, S.; Salvador-Carulla, L.; Zucchi, S.; Cesano, S.; Testa, C.; Scala, E.; Pinciaroli, L. Indicators predicting use of mental health services in Piedmont, Italy. J. Ment. Health Policy Econ. 2005, 8, 95–106. [Google Scholar] [PubMed]
- Peen, J.; Dekker, J. Social deprivation and psychiatric service use for different diagnostic groups. Soc. Sci. Med. 2001, 53, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Dekker, J.; Peen, J.; Goris, A.; Heijnen, H.; Kwakman, H. Social deprivation and psychiatric admission rates in Amsterdam. Soc. Psychiatry Psychiatr. Epidemiol. 1997, 32, 485–492. [Google Scholar] [PubMed]
© 2014 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/3.0/).
Share and Cite
Sadeniemi, M.; Pirkola, S.; Pankakoski, M.; Joffe, G.; Kontio, R.; Malin, M.; Ala-Nikkola, T.; Wahlbeck, K. Does Primary Care Mental Health Resourcing Affect the Use and Costs of Secondary Psychiatric Services? Int. J. Environ. Res. Public Health 2014, 11, 8743-8754. https://doi.org/10.3390/ijerph110908743
Sadeniemi M, Pirkola S, Pankakoski M, Joffe G, Kontio R, Malin M, Ala-Nikkola T, Wahlbeck K. Does Primary Care Mental Health Resourcing Affect the Use and Costs of Secondary Psychiatric Services? International Journal of Environmental Research and Public Health. 2014; 11(9):8743-8754. https://doi.org/10.3390/ijerph110908743
Chicago/Turabian StyleSadeniemi, Minna, Sami Pirkola, Maiju Pankakoski, Grigori Joffe, Raija Kontio, Maili Malin, Taina Ala-Nikkola, and Kristian Wahlbeck. 2014. "Does Primary Care Mental Health Resourcing Affect the Use and Costs of Secondary Psychiatric Services?" International Journal of Environmental Research and Public Health 11, no. 9: 8743-8754. https://doi.org/10.3390/ijerph110908743