Article Text

Abstract
Objectives Adverse occupational exposures can accelerate age-related lung function decline. Some longitudinal population-based studies have investigated this association. This study aims to examine this association using findings reported by longitudinal population-based studies.
Methods Ovid Medline, PubMed, Embase, and Web of Science were searched using keywords and text words related to occupational exposures and lung function and 12 longitudinal population-based studies were identified using predefined inclusion criteria. The quality of the studies was assessed using the Newcastle-Ottawa Scale. Lung function decline was defined as annual loss of forced expiratory volume in 1 s (FEV1), forced vital capacity (FVC) or the ratio (FEV1/FVC). Fixed and random-effects meta-analyses were conducted to calculate pooled estimates for ever and cumulative exposures. Heterogeneity was assessed using the I2 test, and publication bias was evaluated using funnel plots.
Results Ever exposures to gases/fumes, vapours, gases, dusts, fumes (VGDF) and aromatic solvents were significantly associated with FEV1 decline in meta-analyses. Cumulative exposures for these three occupational agents observed a similar trend of FEV1 decline. Ever exposures to fungicides and cumulative exposures to biological dust, fungicides and insecticides were associated with FEV1 decline in fixed-effect models only. No statistically significant association was observed between mineral dust, herbicides and metals and FEV1 decline in meta-analyses.
Conclusion Pooled estimates from the longitudinal population-based studies have provided evidence that occupational exposures are associated with FEV1 decline. Specific exposure control and respiratory health surveillance are required to protect the lung health of the workers.
- Occupational Health
- Dust
- Pesticides
- Solvents
- Lung function
Statistics from Altmetric.com
WHAT IS ALREADY KNOWN ON THIS TOPIC
Epidemiological studies suggest that some occupational exposures are associated with the decline in forced expiratory volume in 1 s (FEV1) and forced vital capacity (FVC) or FEV1/FVC. However, the findings from general population-based studies are inconclusive and not systematically synthesised.
WHAT THIS STUDY ADDS
We found exposures to gases/fumes, vapours, gases, dusts, fumes (VGDF), aromatic solvents, biological dust, fungicides and insecticides were associated with FEV1 decline. Other exposures such as herbicides, mineral dust and metals did not show statistically significant associations in the pooled analysis.
HOW THIS STUDY MIGHT AFFECT RESEARCH, PRACTICE OR POLICY
Periodic workplace health surveillance and lung function testing in exposed occupations will help to identify respiratory disease at an early stage to control the exposure and to protect against further disease progression.
Introduction
Lung function decline is a normal feature of ageing in adults, but excessive decline can result in lung function deficits imposing substantial public health burden.1 A lower level of lung function and decline in forced expiratory volume in 1 s (FEV1) as a predictor of lung function is associated with the development of chronic 0bstructive pulmonary disease (COPD),2 which is now the world’s fourth leading cause of death and projected to be the third leading cause by 2030.3 Accelerated decline in FEV1 or FEV1/forced vital capacity (FVC) is also associated with increased risks of cardiovascular morbidity and mortality as well as all-cause mortality.3
There is some evidence that occupational exposures can be a risk factor for lung impairment. The relationships between occupational exposures and lung function status and decline have been investigated in workplace-based studies, specifically in farmers, bakers, timber, cotton textile, manufacturing and construction workers.4–7 Several cross-sectional studies have also shown that occupational exposures to vapours, gases, dusts, fumes (VGDF) were associated with poor lung function in the general population.8–10 Given these links, it is important to investigate the lung function decline using longitudinal studies, where people have different work histories throughout their careers, and the outcomes may vary between follow-ups.11 There are a limited number of longitudinal population-based studies that investigated this association, and their findings are contradictory and inconclusive.
Previous systematic reviews have been conducted to synthesise the evidence for the relationship between occupational exposures and lung function, but they were limited to a few specific occupational exposures and risk of airflow obstruction and only included cross-sectional studies.11–13 A recent systematic review and meta-analysis reported an association between exposure to organic dust and lung function decline using data from workplace-based studies.12 While other studies identified the association between exposre to biological dusts, mineral dusts, respirable quartz dust, gases/fumes and pesticides and the risk of COPD,14 they did not investigate lung function decline.11 13 15 Given there was no systematic review or meta-analysis synthesising the relationship between occupational exposures (ever and cumulative) and lung function decline in longitudinal population-based studies, we aimed to examine this association using findings reported by longitudinal population-based studies.
Methods
Search strategy and selection criteria
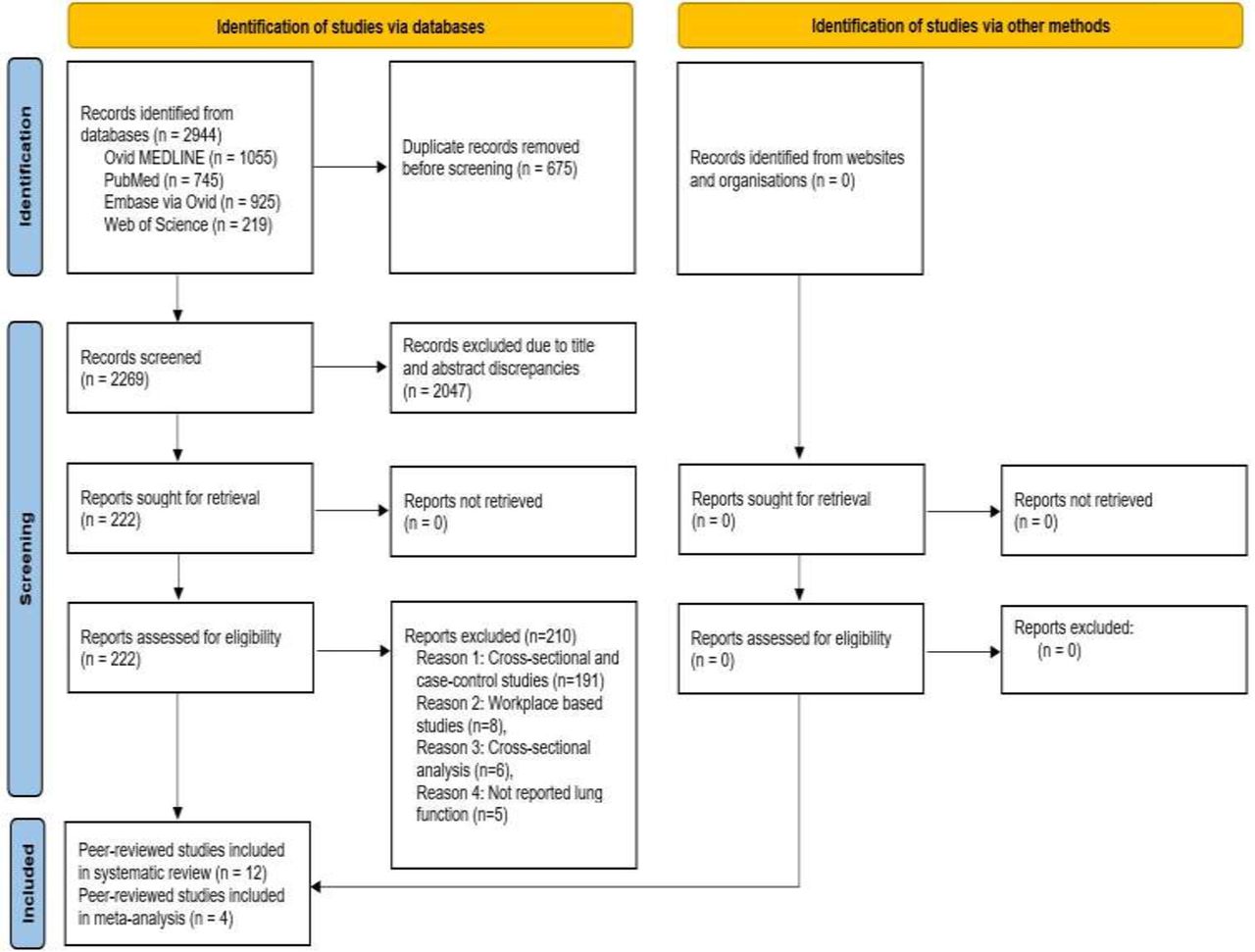
This systematic review and meta-analysis was performed according to the updated version of the PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analysis) guideline (figure 1).16 The study was registered in PROSPERO (International Prospective Register of Systematic Reviews) in 2020 (CRD42020154227). The detailed prespecified protocol is available on request.
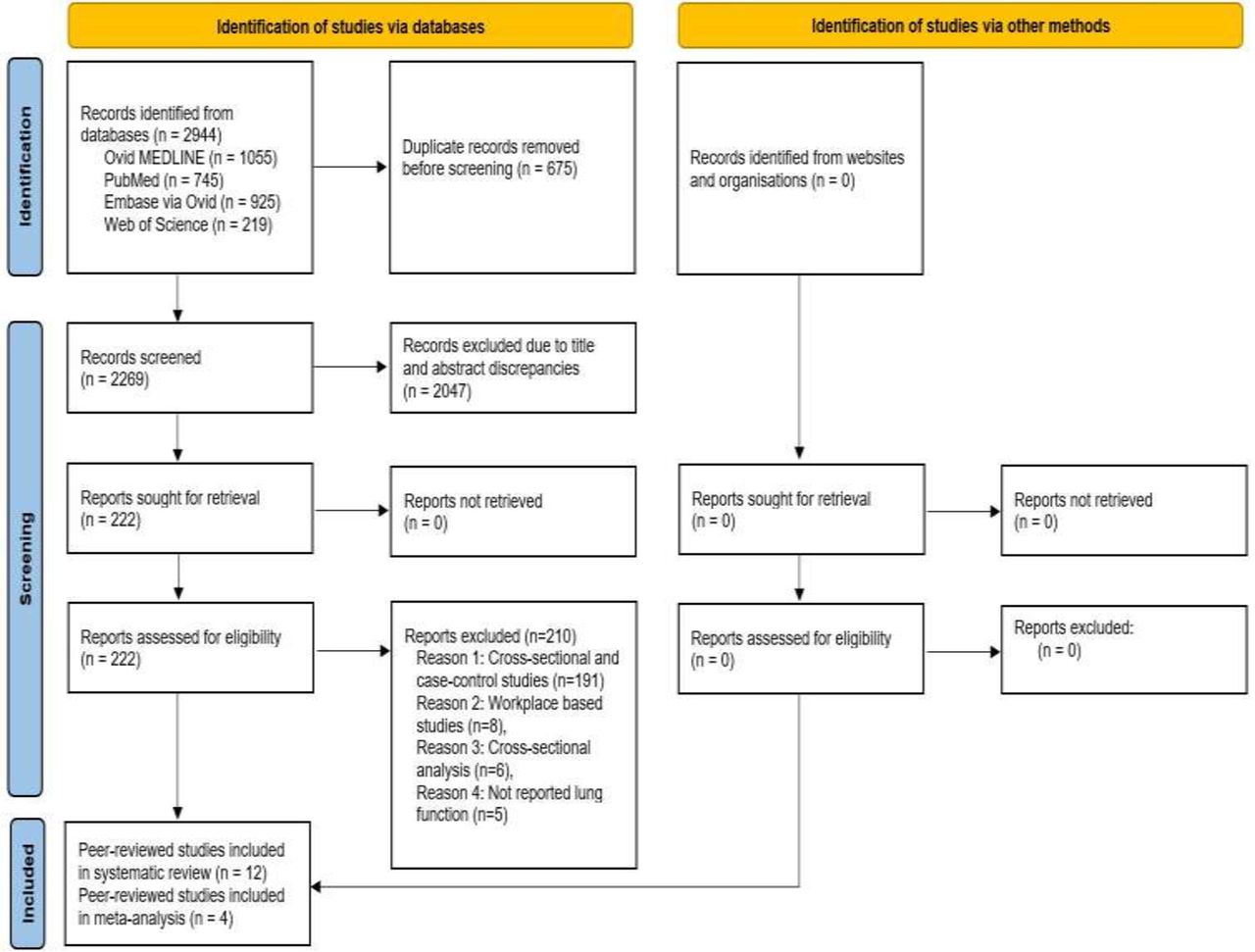
PRISMA (Preferred Reporting Items for Systematic Reviews and Mata-Analysis) 2020 flowchart of peer-reviewed study selection process.
An extensive search strategy was developed to retrieve all articles published up to September 2021 in Ovid Medline, PubMed, Embase and Web of Science. We combined three sets of Medical Subject Headings (MeSH) keywords and text words to identify articles (online supplemental material 1). Additional searches were undertaken in the reference lists from retrieved articles in order to identify studies that may have been missed from the initial search. We followed the Population, Exposure, Comparator group and Outcome (PECO) criteria defined by Morgana et al.17 We defined cohorts as the population, the occupationally exposed group as exposure, the non-exposed group (to particular agent) as comparator and lung function decline as the outcome of interest.
Supplemental material
Search results were compiled using the bibliographic software Endnote X9.3. Two independent researchers (GR and NN) screened retrieved articles. The same investigators independently assessed full texts of records deemed eligible for inclusion. Any discrepancies were resolved by discussion and consensus with a third investigator (SMA).
Inclusion and exclusion criteria
We included English language peer-reviewed studies that reported associations between occupational exposures of interest including biological dust, mineral dust, VGDF, fungicides, herbicides, insecticides, aromatic solvents, chlorinated solvents, metals, fibres or mists and lung function decline. We included longitudinal population-based studies with at least 1 year of follow-up that reported an association between occupational exposures and lung function decline. We excluded studies that did not report lung function decline with repeated lung function measurements. We also excluded cross-sectional, case-control, case-series, reviews, editorials, letters and correspondence.
Exposure definitions
The exposures were subdivided into not exposed (to particular agent, not against any occupational exposures), ever exposed, less likely to be exposed or low exposed, and highly exposed according to the exposure assessment methods such as expert assessment, Job Exposure Matrices (JEMs) or self-reported exposure. Cumulative duration of exposure and lung function decline were also extracted from the selected studies. All the studies defined the non-exposed group as those not exposed to particular occupational exposures as defined by the JEM.
Outcome definitions
The primary outcome considered in our review was annual loss (decline rate) of pre-bronchodilator or post-bronchodilator (1) FEV1, (2) FVC, or (3) the ratio of FEV1/FVC.
Quality assessment of included studies
We assessed risk of bias of included studies using the nine items of the Newcastle-Ottawa Scale (NOS) for cohort studies.18 The quality of the included studies was established by evaluating the study settings, completeness and duration of the follow-up, validity and completeness of exposure and outcomes ascertainment, generalisability of the study findings and adjustment for the known confounding variables using NOS (more details are given in the online supplemental material 1). The scale granted a maximum of nine points for each cohort, studies were assessed as good quality if they scored at least six items, moderate quality if they scored in four or five items, and low quality if they scored for three or fewer items.19 All the included studies scored six or more in quality assessment.
Data extraction and statistical analysis
The following information was extracted: first author, study location, sample size, study design, duration of follow-up, age at inception, occupational exposures assessment methods, measurement of lung function decline and confounders adjusted. FEV1 and FVC or ratios of FEV1/FVC were extracted with corresponding coefficient (β) and 95% confidence intervals (CIs) for the 11 exposures from the studies included. Studies with similar type of exposures and uniform pattern of outcomes assessment were combined for meta-analysis. Although there was variation in the study results, methodology and location, we included four studies for ever exposures and three studies for cumulative exposures out of 12 in meta-analysis (one study was added twice because it reported two cohort results separately in the same article). Sub-group analysis was conducted for FEV1 of nine exposures with similar exposure assessment (ALOHA plus JEM). As the heterogeneity between the studies varied, we performed both fixed and random effects meta-analysis and the pooled estimates were displayed using forest plots, and the publication bias was assessed using the funnel plot20 and Egger’s test (p<0.05 considered representative of statistical significance).21 The heterogeneity between studies was assessed using Higgins I2 statistic.22 We used Stata version 16.1 (Stata Corporation, College Station, Texas, USA) to perform the statistical analyses and pooled estimates were calculated by using the ‘metan’ package.
Results
Study selection
In total, 2944 records were identified through the initial database searches. Following the removal of 675 duplicates, the titles and abstracts of 2269 records were screened to identify papers eligible for full-text assessment. This left 222 articles where the full texts were reviewed. Studies were also included for full-text assessment if it was not clear from the title and/or abstract whether the article included data on occupational exposures and lung function decline. Twelve relevant articles were finally included in this systematic review, and four articles included in the meta-analysis of ever exposures and three articles for cumulative exposures (figure 1).
The summary characteristics of the 12 population-based cohort studies1 2 23–32 are presented in table 1 and the data on lung function decline are presented in online supplemental material table S1. The duration of follow-up in the studies ranged from 4.5 to 25 years, sample sizes ranged from 237 to 17 833, and the mean age at baseline ranged from 33.9 to 60.6 years. Eleven studies included both male and female participants, and one study included only male participants.26 The methodological quality of all the studies included in the systematic review ranged from six to eight out of a scale of nine (table 2). This parameter indicated a good overall quality, so sensitivity analysis was not conducted by excluding any papers.
Summary characteristics of the 12 longitudinal population-based studies included in the systematic review that examined the association between occupational exposures (ever and cumulative) and lung function decline
Methodological quality score of 12 studies included in the systematic review based on Newcastle-Ottawa quality assessment score
The studies used different exposure assessment methods. Most of the studies used JEMs to assess exposures,1 2 23 24 28–32 however only three studies were based on self-report.25–27 Exposure metrics (eg, ever/never, low/high, cumulative) were assigned by lifetime work history calendars,1 23 29 30 32 current job titles2 24 28 31 and any jobs at baseline or follow-up.25–27 All studies reported FEV1 and six studies1 23 24 28 30 32 also reported FVC as indices of lung function. The units for lung function decline were presented as either ml/year or %predicted/year.
Ten studies followed American Thoracic Society (ATS) and European Respiratory Society (ERS) guidelines to perform spirometry,1 2 23–26 29–32 but two studies did not mention any spirometry guidelines.27 28 Eight studies presented outcomes using pre-bronchodilator (BD) spirometry,1 2 24 26–28 30 31 two studies used post-BD spirometry,25 32 one study used both pre-BD and post-BD,23 and one study perform spirometry without BD.29 One study included early COPD and current smokers at the baseline of the cohort,25 whereas the other cohorts did not have this criterion. All studies adjusted the associations for age, sex and smoking status except for one,23 which adjusted only for sex and socioeconomic status as this study developed a directed acyclic graph model for potential confounders and found smoking did not confound the association. Another three studies additionally adjusted for asthma, previous respiratory infection or lung diseases, co-exposures, among other factors.1 2 29
Occupational exposures (ever and cumulative) and lung function decline
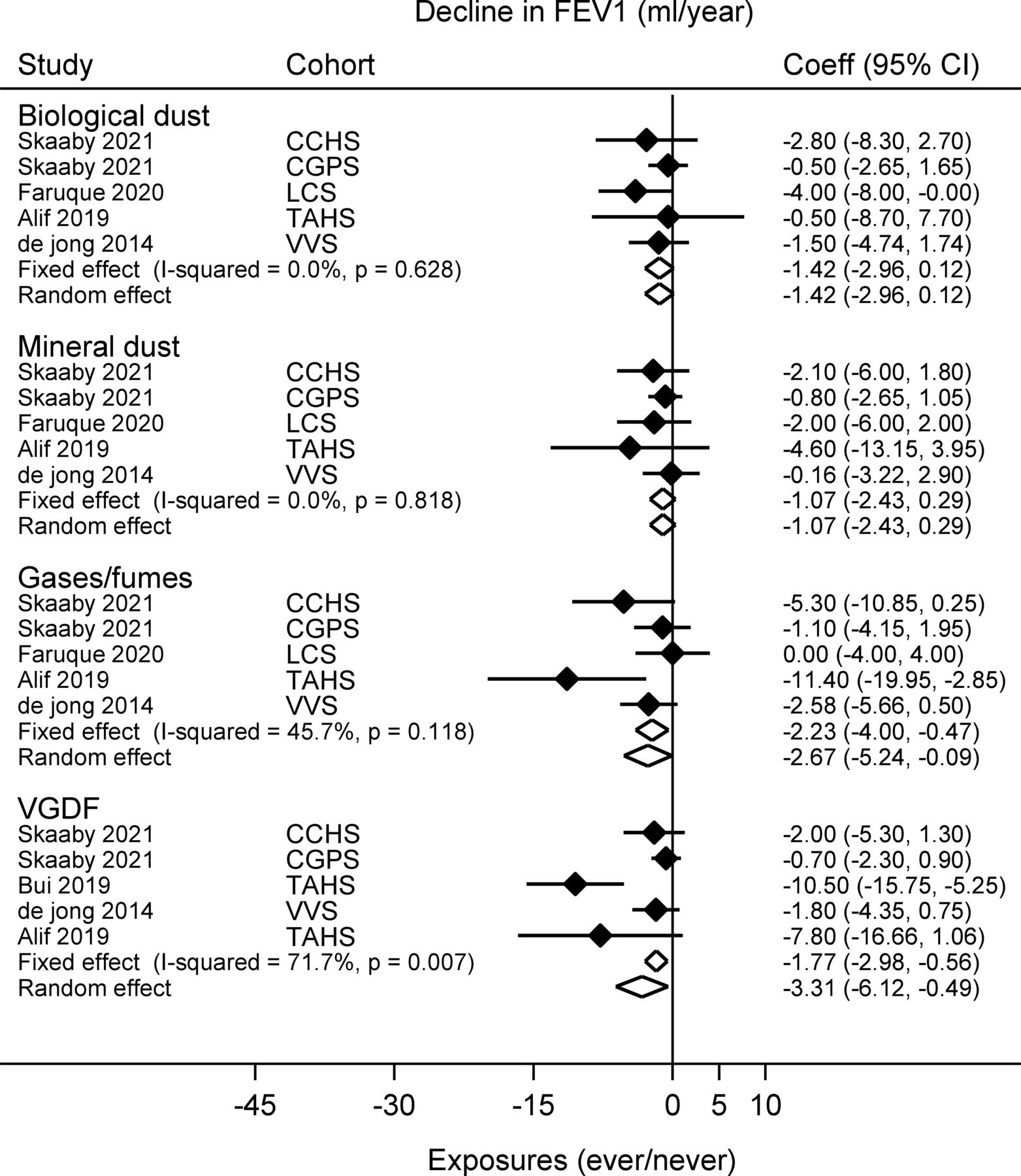
Of the 12 studies, six reported associations between biological dust and decline in FEV1, FVC or ratio of FEV1/FVC as lung function outcomes (online supplemental material table S1).1 2 24 30–32 Two studies reported a significant decline in FEV1 for ever exposures to biological dust compared with never exposures.24 32 The pooled estimates from both fixed and random effect meta-analysis found little evidence of heterogeneity (I2=0%) and 1.42 mL/year decline in FEV1 was observed with ever exposures to biological dust (figure 2). However, a meta-analysis of cumulative exposures provided evidence of an association for biological dust in the fixed effect model (table 3, online supplemental material figure S1). Publication bias was assessed by funnel plot (online supplemental material figure S3A and online supplemental material S4A) and an Egger’s test for small-study effects showed no publication bias (p=0.001).
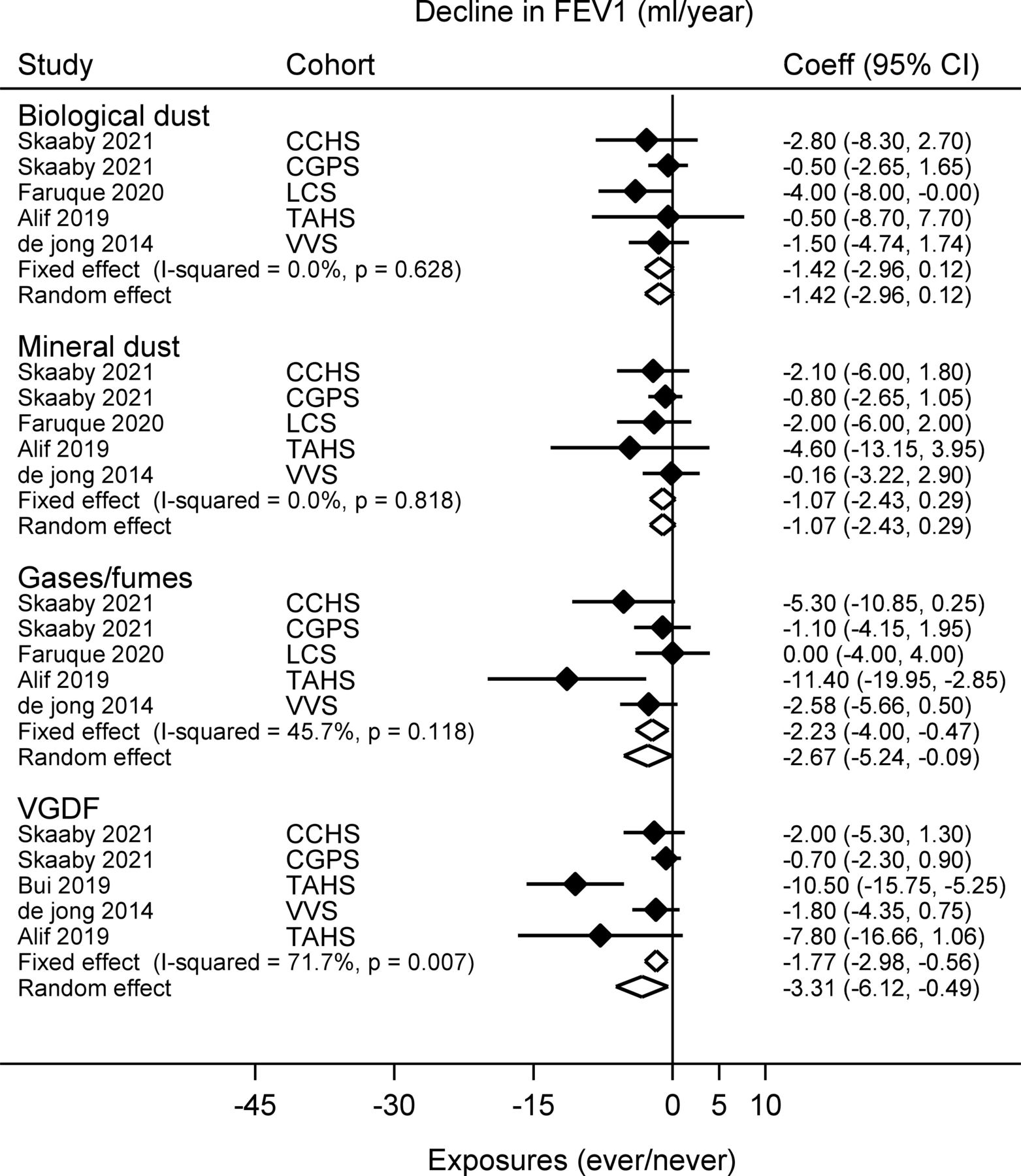
Forest plot showing the association between exposures to biological dust, mineral dust, gases/fumes and vapours, dust, gases and fumes (VGDF) and forced expiratory volume in 1 s (FEV1) decline. CCHS, Copenhagen City Heart Study; CGPS, Copenhagen General Population Study; LCS, Lifelines Cohort Study; TAHS, Tasmanian Longitudinal Health Study; VVS, Vlagtwedde-Vlaardingen Study.

Forest plot showing the association between exposures to fungicides, herbicides and insecticides and forced expiratory volume in 1 s (FEV1) decline. LCS, Lifelines Cohort Study; TAHS, Tasmanian Longitudinal Health Study; VVS, Vlagtwedde-Vlaardingen Study.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Forest plot showing the association between exposures to aromatic solvents and metals and forced expiratory volume in 1 s (FEV1) decline. LCS, Lifelines Cohort Study; TAHS, Tasmanian Longitudinal Health Study.
Association between cumulative exposures (per intensity-year) and decline in FEV1 (mL) in three studies included in systematic review and meta-analysis
Seven studies reported the association between ever exposures to mineral dust and decline in FEV1, FVC or ratio of FEV1/FVC.1 2 24 26 30–32 None of the studies reported the statistically significant association for decline in FEV1, however Sunyer et al reported that women had a greater decline in FEV1 but the association was not significant for men.31 One study by Faruque et al reported a significant decline in FVC with exposure to mineral dust compared with never exposures (online supplemental material table S1).24 Meta-analysis for both ever and cumulative exposures did not show significant decline in FEV1 compared with never exposures (figure 2, table 3). No publication bias was found by visualising the funnel plot (online supplemental material figure S3A, S4A), and Egger’s test for small-study effects also showed no sign of publication bias (p=0.001).
Exposures to gases/fumes have been reported in seven studies.1 24–26 30–32 The meta-analysis found a statistically significant decline in FEV1 for ever and cumulative exposures to gases/fumes compared with never exposures (figure 2, table 3, online supplemental material figure S1). There was a moderate amount of heterogeneity for ever exposures (I2=45.7%) but cumulative exposures showed little evidence of heterogeneity (I2=0%) between the studies. Funnel plot (online supplemental material figure S3A and online supplemental material S4A) and Egger’s test for small-study effects showed no publication bias in the analysis (p=0.001).
Combined exposures to VGDF and decline in FEV1 were reported in five studies (online supplemental material table S1).1 2 23 30 32 The meta-analysis of both fixed and random-effects models found a statistically significant decline in FEV1 (1.77 mL/year and 3.31 mL/year) for ever exposures to VGDF compared with never exposures (figure 2). The trend was consistent for cumulative exposures to VGDF and decline in FEV1 (table 3, online supplemental material figure S1). There was a large amount of heterogeneity for ever exposures (I2=71.7%) and no evidence of heterogeneity (I2=0%) for cumulative exposures between the studies was found. Funnel plot (online supplemental material figure S3A, S4A) and Egger’s test for small-study effects showed no publication bias in the analysis (p=0.001).
The meta-analysis of ever and cumulative exposures to fungicides, herbicides and insecticides and the decline in FEV1 found consistent results in both models. Ever exposures to fungicides were found to be associated with a 3.11 mL/year decline in FEV1 (figure 3) in the fixed-effect model and a similar trend was observed for cumulative exposures (table 3). However, the association was not statistically significant in the random-effects models for both ever and cumulative exposures. No statistically significant association was found for ever and cumulative exposures to herbicides and insecticides and a decline in FEV1 was found. The heterogeneity between the studies showed small to moderate heterogeneity (figure 3, online supplemental material S2). The funnel plot (nd online supplemental material figure S3B, S4B) and Egger’s test for small-study effects showed no publication bias in the analysis (p=0.18 and p=0.00, respectively).
The decline in FEV1 was significantly associated with the ever and cumulative exposures to aromatic solvents. The pooled estimates of ever exposures to aromatic solvents was found to be associated with a greater decline in FEV1 for both models (6.16 mL/year and 7.35 mL/year, respectively) compared with never exposures (figure 4). Cumulative exposures to aromatic solvents also exhibited a statistically significant decline in FEV1 (0.60 mL/intensity-year) compared with never exposures (table 3, online supplemental material figure S2). No association was found between metals and decline in FEV1. There was a moderate amount of heterogeneity for ever exposures (I2=57.4%) and no evidence of heterogeneity (I2=0%) for cumulative exposures between the studies was found. The funnel plot (online supplemental material figure S3B, S4B) and Egger’s test for small-study effects showed no publication bias in the analysis (p=0.25 and p=0.0, respectively).
Discussion
Our systematic review and meta-analysis assesses the evidence on the association between ever and cumulative occupational exposures and lung function decline in longitudinal population-based studies. Ever and cumulative exposures to gases/fumes, VGDF and aromatic solvents were significantly associated with FEV1 decline. Associations between ever exposures to fungicides and cumulative exposures to biological dust, fungicides and insecticides and decline in FEV1 were also observed in fixed-effect models. Exposures to mineral dust, herbicides and metals and decline in FEV1 were not statistically significant in fixed or random effects models for meta-analysis of both ever and cumulative exposures. However, these occupational exposures appeared to confer a decline in lung function in pooled estimates for both of the models.
The pooled estimates of ever exposures to gases/fumes and decline in FEV1 was observed to be statistically significant compared with never exposures. A meta-analysis of cumulative exposures to gases/fumes also found consistent evidence of the decline in FEV1 for both fixed and random effects models. To our best knowledge, no previous studies have reviewed or meta-analysed these associations. Our systematic review found inconsistent associations between exposure to gases/fumes and FEV1 in population-based studies (online supplemental material table S1). However, the Vlagtwedde-Vlaardingen Dutch cohort found lower FEV1 and FEV1/FVC ratio with high exposure to gases/fumes and the association was significantly stronger for ever smokers.8 Sunyer et al from ECRHS I and II data reported that women had a 3 mL/year greater decline in FEV1 compared with men for high exposure to gases/fumes.31 The association was also stronger for ex-smokers and no association was observed for men.31 In addition, a study from Norway found a greater decline in FEV1 only in men in exposure to sulphur dioxide gases.26 Another study from the Netherlands found faster decline in FVC in exposure to gases/fumes.24
Cross-sectional studies have found that occupational exposure to VGDF was clearly associated with lower level of FEV1 and FEV1/FVC in the general population.10 33 34 The associations between exposure to VGDF and decline in FEV1 are inconsistent in our systematic review (online supplemental material table S1). However, our pooled results showed a strong association between ever and cumulative exposures to VGDF and decline in FEV1. Australian study data used from the TAHS cohort used both pre-BD and post-BD spirometry measurements and found strong associations for high exposure to VGDF and decline in FEV1 in both measurements (we included pre-BD measurement in our meta-analysis).23 A Dutch cohort found a lower level of FEV1 and FEV1/FVC with high exposure to VGDF and the association was strong for ever smokers (96 mL/year decline).8 However, a multicentre study by Zock et al did not find a decline in FEV1 for high exposure to VGDF, but a mean 61 mL/year decline in FEV1 was observed for current smokers.34 VGDF exposure was also associated with a decline in FEV1/FVC ratio reported in two longitudinal population-based studies in our systematic review.1 23
The associations between exposure to herbicides, insecticides and fungicides were inconsistent in the systematic review (online supplemental material table S1). The pooled estimates also showed similar trends for ever and cumulative exposures and decline in FEV1. However, ever exposures to fungicides and cumulative exposures to fungicides and insecticides exhibited an association only in fixed-effect models but the association was attenuated in the random effect models. Similar to our meta-analysis, several workplace-based cross-sectional studies also found lower FEV1 and FVC following exposure to fungicides, herbicides and insecticides in farmers or agricultural workers or pesticide applicators,35–39 whereas a few studies also found no associations.40 41 A recent systematic review and meta-analysis reported a reduction of FEV1/FVC following pesticide (cholinesterase inhibiting) exposure in the general population.42 However, a Dutch cohort study reported that high exposures to fungicides, herbicides and insecticides were associated with significantly lower levels of FEV1 and exposure to fungicides are also related to lower levels of FEV1/FVC.8
The reason for these inconsistencies could be related to spirometric criteria, where some studies reported pre-BD, but others post-BD measurements. The ATS/ERS guideline recommends using post-BD spirometry to distinguish between reversible (asthma) and irreversible (airflow obstruction) obstruction, particularly in younger adults.43 However, none of the studies included used post-BD to measure lung function. The previous NHANES III study described that the use of a bronchodilator might vary the association up to 200% due to differences in spirometric criteria between population-based studies.44
Results from population-based studies have provided evidence of the association between lung function decline and solvent exposures (online supplemental material table S1), which is consistent with several population-based cross-sectional studies.8 45–47 We found a significant association between ever and cumulative exposures to aromatic solvents and FEV1 decline in our meta-analysis compared with never exposures. Two studies from the Australian TAHS cohort found a strong association between exposure to aromatic solvents and decline in FEV1 and FVC, when lung function was defined using pre-BD spirometry and adjusted for all possible confounders, including sex, smoking, socioeconomic status and so on.1 23 However, another study from the same cohort did not find a significant association with post-BD spirometry to define lung function and also did not adjust for smoking in the final model.23 This also indicates that the difference in spirometry and the use of pre-BD measurements could overestimate the results.
The lung function parameters were not uniform across studies, and therefore it was difficult to include all studies in the meta-analysis for pooled estimates of ever and cumulative exposures and lung function decline. Furthermore, several methods have been used to assess occupational exposures in population-based studies, as direct assessment of exposure is difficult in such studies. Most of the studies reported absolute FEV1 as a measure of lung function decline, while a few reported %predicted or the ratio as a measure of lung function decline. Another concern is that the association between occupational exposures and lung function could be confounded by pre-existing occupational or work-exacerbated asthma and co-exposures. Most of our included studies did not adjust for asthma, except Alif et al and Lytras et al and only two studies1 2 included in the meta-analysis were adjusted for co-exposure. To untangle the possible effect of asthma and co-exposure on lung function decline, longitudinal studies should adjust for asthma and co-exposure or use the universal non-exposed group across all exposures in the statistical analysis.
The subjects in most of our included studies had a wide age range, and a few of them included young adults in their thirties.2 26 31 The decline in FEV1 and FVC may accelerate with age and is also exacerbated by smoking.19 Several cross-sectional48 49 and longitudinal studies reported that lung function parameters such as FEV1 and FVC decline with age.50 51 Because some factors such as loss of lung elasticity weakened respiratory muscles and decreased surface area for alveolar gas exchange, these were invariably accompanied by ageing.19 For example, the ECRHS reported that high exposure to VGDF was associated with 61 mL lower FEV1 in current smokers34 whereas the LifeLines cohort Study from the Netherlands found 96 mL lower FEV1.8 These differences might related to younger average age of the ECRHS sample (range 20–44 years) compared with the LifeLines cohort (range 18–89 years).8 Therefore, age is an important factor for change in lung function, as lung function decline is evident above the age of 30,52 moreover the variability of individual measurements around the median is not uniform across all ages and heights.53 There was a variation in mean age across the studies which could underestimate the pooled estimate the FEV1 in our meta-analysis. Furthermore, the inclusion of population-based studies reduced the number of exposed people could have further restricted the number of studies to detect an association. Most of our included studies did not present their results stratified by age. Therefore, it was not possible to conduct age specific subgroup analysis in the meta-analysis. Lung function declines with age in normal, asymptomatic adults with higher rates of decline in FEV1 and FVC in men compared with women.19 Some studies also reported that sex was a modifying factor; however not all studies reported stratified analysis by sex, which prevented us from conducting subgroup analysis.
The strengths of this review are the inclusion of the longitudinal population-based studies with objective measurements of lung function and a minimum of 1 year of follow-up with adjustment for important confounders such as smoking, age and sex. We have attempted to use standardised classification of exposure and outcome definition. We have focused on FEV1 as a parameter of lung function decline, preferably with pre-BD measurement as most of the studies reported it. All studies in the meta-analysis of ever and cumulative exposures used similar spirometry measurements to control the heterogeneity except one study29 used without BD in the meta-analysis of cumulative exposures. Another important thing is that the consistent exposure-outcome associations existed between ever and cumulative exposures.
Our review used consistent exposure assessment as most of the included studies used ALOHA plus JEM to assess exposures. This is a useful method for occupational exposure assessment because JEM consistently assigns exposures, irrespective of the disease status of an individual, which helps to reduce differential information bias.11 The advantages of JEM helped to evaluate the possible effect with greater precision. However, a few studies also used less reliable self-reported exposure assessment,25–27 which was not included in the meta-analysis. Follow-up time is of great importance, and in order to reliably assess lung function decline, several years of follow-up are required to achieve robust estimates, as argued by Burrows et al,54 and supported by an official statement from the ATS/ERS on spirometry in the workplace.55 In our systematic review and meta-analysis the follow-up ranged from 4.5 years to 25 years.
There are a few limitations in our study. JEM-based exposure assessment includes crude categories of ever exposures; therefore, we are unable to identify the specific gases, fumes, fungicides, herbicides, insecticides, aromatic solvents, chlorinated solvents, and metals or fibres and the exact duration of exposure responsible for lung function decline in individuals. The number of studies included in the meta-analysis was small due to strict inclusion and exclusion criteria. The inclusion of small numbers of studies in our meta-analysis might restrict statistical power to detect the association in pooled estimates and affect the generalisability of the results. Reporting bias may also be of concern due to the known risk of publication of studies with significant results. We assessed publication bias by visual inspection of funnel plots and did not observe any clear trends of bias. We were also unable to perform any subgroup analysis because the studies did not consistently provide results stratified by factors of interest, for example, age and sex. The response rate in our included studies varied from 11% to 93%, and two studies did not report their response rates.2 28 As the cut-off at 50% to define a satisfactory response,12 the loss of follow-up was unlikely to introduce bias in the included studies.
Conclusion
In this systematic review and meta-analysis, we found significant evidence that occupational exposures to gases/fumes, VGDF and aromatic solvents were associated with a greater decline in lung function. This trend was also persistent in the meta-analysis of cumulative exposures and lung function decline. In addition, this study also finds the relationship between ever and cumulative exposures to several exposures such as fungicides, insecticides and biological dust and lung function decline. Although, there was a significant decline in lung function parameters for some exposures, there was a high degree of heterogeneity between studies which limits the interpretation in terms of causal association. In addition, due to inconsistent exposure assessment tools and reporting in the individual studies and lack of data in subgroups, we were unable to conduct subgroup analysis, which future studies should focus on.
Ethics statements
Patient consent for publication
Ethics approval
Not applicable.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Contributors SMA developed the concept, design and the instruments to conduct the study. GR and NN performed the database search, and screened the articles, GR and SMA extracted the data, and GR performed the meta-analyses. GR and SMA drafted the manuscript and all authors provided critical input. All authors read and approved the final version of the manuscript for publication.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests MJA holds investigator-initiated grants from Pfizer, Boehringer-Ingelheim, Sanofi and GSK for unrelated research. He has undertaken an unrelated consultancy and received assistance with conference attendance from Sanofi. He has also received a speaker’s fee from GSK. SCD holds investigator-initiated grants from GSK. All other authors declare no conflicts of interest.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.