Article Text

Abstract
Objective To compare cancer incidence in Fire Department of the City of New York (FDNY) firefighters who worked at the World Trade Center (WTC) site to incidence in a population of non-WTC-exposed firefighters, the Career Firefighter Health Study (CFHS) cohort, and to compare rates from each firefighter cohort to rates in demographically similar US males.
Methods FDNY (N=10 786) and CFHS (N=8813) cohorts included male firefighters who were active on 11 September 2001 (9/11) and were followed until death or 31 December 2016. Cases were identified from 15 state cancer registries. Poisson regression models assessed cancers in each group (FDNY and CFHS) versus US males, and associations between group and cancer rates; these models estimated standardised incidence ratios (SIRs) and adjusted relative rates (RRs), respectively. Secondary analyses assessed surveillance bias and smoking history.
Results We identified 915 cancer cases in 841 FDNY firefighters and 1002 cases in 909 CFHS firefighters. FDNY had: higher rates for all cancers (RR=1.13; 95% CI 1.02 to 1.25), prostate (RR=1.39; 95% CI 1.19 to 1.63) and thyroid cancer (RR=2.53; 95% CI 1.37 to 4.70); younger median ages at diagnosis (55.6 vs 59.4; p<0.001, all cancers); and more cases with localised disease when compared with CFHS. Compared with US males, both firefighter cohorts had elevated SIRs for prostate cancer and melanoma. Control for surveillance bias in FDNY reduced most differences.
Conclusions Excess cancers occurred in WTC-exposed firefighters relative to each comparison group, which may partially be explained by heightened surveillance. Two decades post-9/11, clearer understanding of WTC-related risk requires extended follow-up and modelling studies (laboratory or animal based) to identify workplace exposures in all firefighters.
- epidemiology
- firefighters
- occupational health
Data availability statement
Reasonable requests for deidentified data will be considered by the investigators and the National Institute for Occupational Safety and Health.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Key messages
What is already known about this subject?
Firefighters are routinely exposed to known carcinogens. Evidence of an increased risk of cancer in firefighters remains mixed. Work exposures for firefighters at the World Trade Center (WTC) site, an especially toxic environment, further complicate risk assessment.
What are the new findings?
WTC-exposed male firefighters had 13% higher all-cancer rates, and younger median age (55.6 vs. 59.4 years) and more localised disease at diagnosis compared with a cohort of non-WTC-exposed male firefighters. Both firefighter cohorts had elevated prostate cancer and melanoma rates compared with demographically similar US males.
How might this impact on policy or clinical practice in the foreseeable future?
Surveillance bias may account for some of the excess cancers identified in both firefighter cohorts compared with similar US males. Two decades post-9/11, clearer understanding of the WTC-related cancer risk requires additional years of follow-up to allow for the reported long latency of some solid tumours. Laboratory-based or animal-based modelling studies should be encouraged to identify and track workplace exposures in WTC-exposed and non-WTC-exposed firefighters.
Introduction
Firefighters are repeatedly exposed to occupational hazards, including known carcinogens.1 2 There have been over 200 peer-reviewed studies of firefighting and cancer, shown in PubMed,3–9 most published since 2000. Despite this proliferation of studies, the degree to which firefighting is associated with cancer incidence remains uncertain. A 2014 National Institute for Occupational Safety and Health (NIOSH) study found that a cohort of nearly 30 000 professional firefighters had a modest elevation in the rate of all-cancers combined (standardised incidence ratio (SIR)=1.09; 95% CI 1.06 to 1.12) compared with the general US population.4 A recent meta-analysis of 25 cohort studies, including the aforementioned NIOSH cohort, however, reported that the all-cancer risk for firefighters was similar to that of the general population (meta-relative risk=1.0; 95% CI 0.93 to 1.07).10
The World Trade Center (WTC) attacks on 11 September 2001 (9/11) exposed over 15 000 Fire Department of the City of New York (FDNY) firefighters and other rescue/recovery workers to carcinogenic substances11–13 including polychlorinated biphenyls (PCBs), polycyclic aromatic hydrocarbons (PAHs), asbestos, sulfuric acid, benzene and arsenic.2 13 14 Studies of WTC-exposed rescue/recovery workers have generally shown modestly elevated cancer rates compared with general populations.15–19
The current study was undertaken to assess if work as an FDNY firefighter at the WTC site conferred a cancer risk above that attributed to firefighting under non-WTC conditions. Our 2016 study20 compared post-9/11 cancer incidence in the FDNY WTC-exposed firefighter cohort to incidence in the aforementioned NIOSH cohort, hereafter called the Career Firefighter Health Study (CFHS), and found no difference between the cohorts in the rate of all cancers, although rates of some site-specific cancers were significantly elevated (eg, thyroid and prostate cancer) in FDNY. The current study extended follow-up to allow for the detection of cancers up to 15 years post-WTC exposure. We also used smoking data, when available, and we provide perspective for findings in firefighters (WTC-exposed and non-WTC-exposed) by comparing characteristics of these cases to those in the general population. This study is of importance to WTC research as it controls for both occupational exposures using a firefighter comparison group and US secular trends. Given the long latency of some cancers, the relationship between WTC exposure, firefighting and cancer is particularly worthy of close examination during this 20th anniversary year of the WTC attacks.
Methods
Study population
Inclusion required that FDNY and CFHS members be actively employed by their respective departments on 11 September 2001. This study followed the Strengthening the Reporting of Observational Studies in Epidemiology guidelines.
FDNY cohort
The FDNY sample consisted of male firefighters who worked at the WTC site at any time between 11 September 2001 and 25 July 2002 (N=10 786). Male firefighters who did not report any WTC exposure (N=82) were excluded, as were WTC-exposed female firefighters (N=28) due to low numbers. Characteristics of the excluded female firefighters are shown in online supplemental table S1.
Supplemental material
CFHS cohort
The CFHS cohort included 29 992 firefighters from the Philadelphia, Chicago, and San Francisco Fire Departments, originally identified from department rosters, as previously described.4 21 We chose this referent group because they were subject to similar pre-hire fitness requirements, worked in urban environments, and worked at departments with retirement policies similar to FDNY’s. Study inclusion was limited to males who were actively employed on 11 September 2001 (N=8813); 585 females were excluded (online supplemental table S1). Since we were missing information on the WTC exposure history of CFHS members, we considered this cohort to be non-WTC-exposed.
Demographic/background information
Data were obtained from employee databases and FDNY medical records, and death information from the Social Security Death Master File and the National Death Index. One additional FDNY death was identified from employee records. Smoking status (current, former or never smoker) and prior military service were ascertained from health surveys completed by FDNY firefighters during medical monitoring examinations. WTC-exposed FDNY members provided their initial arrival time at the WTC site, hereafter referred to as WTC exposure level, on their first post-9/11 health questionnaire.19 A similar health survey collected smoking status, occupational history and other background information from a sample of CFHS firefighters (N=2856, 32.4%).22
Cancer cases
Information on cancer diagnoses was obtained by probabilistic matching to state cancer registries, as described elsewhere.4 19 20 States were selected for linkage based on the residence information of active and retired FDNY and CFHS firefighters. The FDNY population was linked to Arizona, Connecticut, Florida, North Carolina, New Jersey, New York, Pennsylvania, South Carolina and Virginia state cancer registries. The CFHS population was linked to Arizona, California, Florida, Illinois, Indiana, Michigan, New Jersey, Oregon, Pennsylvania, and Washington state. Ninety-eight per cent of FDNY firefighters and 97% of CFHS firefighters resided in one of the states selected for linkage. Cancer cases defined as primary malignant tumours or in situ bladder cancers23 and diagnosed between 11 September 2001 and 31 December 2016 were analysed.
US cancer rates
We used the National Cancer Institute’s Surveillance, Epidemiology and End Results Program (SEER-21) data to obtain rates of all-cancers combined and some site-specific cancers in the US male population.24 Data were grouped by calendar year (2001 to 2016), race/ethnicity (non-Hispanic white, non-Hispanic Black, Hispanic, Asian and Native American) and 5-year age groups (15–19 to 85–89 years), and incidence rates calculated in these strata. We also obtained information on cancer stage at diagnosis24 and median age at diagnosis.25
Statistical analyses
Selected characteristics of each cohort were compared by calculating means (±SD), medians (IQR) or proportions (%). T-tests, Wilcoxon Mann-Whitney U tests or χ2 tests were performed, as appropriate. Follow-up time started on 11 September 2001 and ended on 31 December 2016 or, if earlier, date of death.
To examine trends over time, we graphed cancer incidence rates by calendar year in FDNY, CFHS and US males (SEER-21) using output from Poisson regression models of year and group predicting cancer cases, with the log of person-years as an offset, controlling for race/ethnicity and 5-year age group. To provide context for the interpretation of cancer risk in firefighters, with and without WTC exposure, our primary analyses involved estimating SIRs and 95% CIs for all-cancer sites combined (all cancers) and some site-specific cancers23 between 11 September 2001 and 31 December 2016, comparing each firefighter cohort with SEER-21.24 We used Poisson regression models with observed numbers of FDNY cancer cases as the outcome variable and the log of the expected case count in each demographic stratum, calculated by multiplying the stratum-specific SEER-21 rate with the number of person-years belonging to that stratum in the FDNY cohort, as an offset. We then reran these models using CFHS in place of FDNY data. Site-specific cancers were chosen based on our previous work examining post-9/11 cancer incidence in FDNY firefighters.19 20
Additional primary analyses fit Poisson regression models assessing the associations between firefighter cohort and cancer rates, controlling for age on 9/11 and race/ethnicity. Adjusted relative rates (RRs) and 95% CIs were estimated using cohort as the independent variable, cancer cases as the outcome, and log of person-years as the offset. The RR for melanoma was estimated from non-Hispanic white males (N=16 238) due to limited cases in non-whites. A sensitivity analysis assessed differences in FDNY and CFHS cohort cancer rates when only first primary cancer cases were included as the outcome; this analysis excluded individuals whose first cancers were diagnosed prior to 9/11 (N=229) and ended follow-up at the first diagnosis date.
Secondary analyses addressed possible surveillance bias, as previously described.19 20 Briefly, WTC-exposed FDNY firefighters undergo free health monitoring exams without copays, including for blood testing, and chest CT scans, as indicated, even after retirement. FDNY cancers could therefore be diagnosed earlier due to screenings that are not widely available to others. Accordingly, we categorised cases of lung, liver, thyroid or kidney cancer or Hodgkin or non-Hodgkin lymphoma diagnosed ≤6 months after chest CT scans and cases of prostate or haematological cancers diagnosed ≤6 months after routine blood tests as cases identified by screening (N=204), repeating the primary analyses after delaying the diagnosis dates of these cancers by 2 years. This time delay was chosen based on the 2-year average lead time for prostate cancers diagnosed in participants of a randomised cancer screening study who received annual screening.20 26 We also performed sensitivity analyses delaying diagnosis dates by 5 years.
We conducted two additional secondary analyses: we analysed the subset of 10 723 FDNY and 2856 CFHS firefighters for whom we had smoking information, repeating the RR analyses comparing FDNY and CFHS cancer rates with smoking status (ever vs never) included as a covariate in the Poisson regression models. We then explored a possible dose–response relationship between WTC exposure level and cancer within the WTC-exposed FDNY cohort only (N=10 786), redoing the RR analyses with an ordinal WTC exposure level variable ranging from lowest to highest-level WTC exposure group19 (table 1) in the models.
Population characteristics
All analyses were performed in SAS (V9.4, SAS, Institute Inc., Cary, NC, http://www.sas.com). Yearly incidence rate graphs were created via PROC SGPLOT using a locally weighted smoothing (LOESS) function for estimates generated from the first Poisson regression models described above.
Results
Selected characteristics of 10 786 WTC-exposed FDNY and 8813 CFHS firefighters are shown in table 1. FDNY firefighters were younger, on average, more likely to be white and never-smokers, and less likely to be combat veterans compared with CFHS firefighters (p<0.001 for all). The FDNY cohort was also consistently younger at diagnosis compared with CFHS: for all cancers (median (IQR)=55.6 (50.2–60.2) vs 60.0 (54.4–64.8) years) and for every cancer subtype examined. Since 9/11, 92.7% of WTC-exposed male FDNY firefighters have had at least 1 prostate-specific antigen (PSA) test, 98.8% at least 1 complete blood count and 47.7% at least 1 chest CT. While we lack comparable data for the CFHS, 96% of those who completed the CFHS health survey reported a visit to a medical doctor within the previous 2 years.
Between 11 September 2001 and 31 December 2016, we identified 915 and 1002 incident cancer cases in 841 FDNY and 909 CFHS firefighters, respectively. Prostate cancer was the most common site-specific cancer in both groups (N=332 and N=358 in FDNY and CFHS, respectively), followed by melanoma of the skin (N=96) and non-Hodgkin lymphoma (N=55) in FDNY and lung cancer (N=83) and melanoma (N=70) in CFHS.
Cancer rates in firefighters (FDNY and CFHS) compared with US males (SEER-21)
Comparing median age at diagnosis across the three groups, we found that generally, FDNY firefighters had the youngest median age and SEER-21 the oldest.25 Similarly, there were differences in cancer stage at diagnosis: FDNY firefighters were usually diagnosed at an earlier, more localised disease stage (table 2).
Proportion of cancers* in localised, regional, distant or unknown stage at time of diagnosis (%)
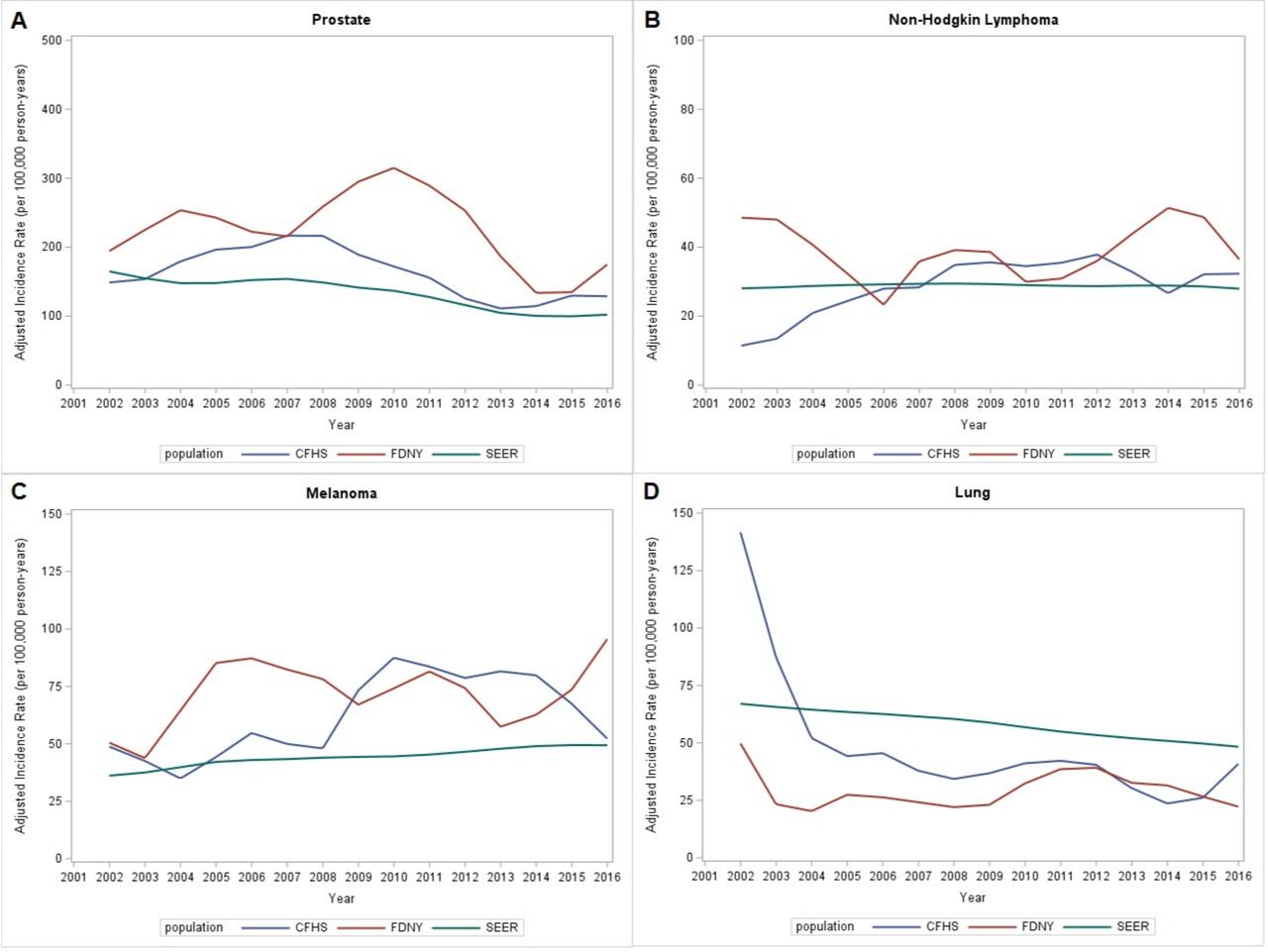
Figure 1 displays the race/ethnicity-adjusted and age group-adjusted cancer incidence rates by calendar year in the FDNY, CFHS and SEER-21 populations. Rates of prostate cancer (figure 1A), non-Hodgkin lymphoma (figure 1B) and melanoma of the skin (figure 1C) were consistently elevated in the FDNY cohort compared with US males; this was especially evident for prostate cancer rates after 2007. Prostate cancer and melanoma rates also appeared to be elevated in CFHS versus US males. In contrast, rates of lung cancer were lower in both firefighter cohorts than in US males (figure 1D).

{kind=link}
Incidence of site-specific cancers by calendar year in World Trade Center (WTC)-exposed firefighters, non-WTC-exposed firefighters and US males. Shown are the adjusted incidence rates over time of selected site-specific cancers, estimated by applying a locally weighted smoothing function to output from Poisson regression models of calendar year and cohort predicting cancer cases. (A) Shows estimated incidence rates of prostate cancer by calendar year in WTC-exposed Fire Department of the City of New York (red) and non-WTC-exposed Career Firefighter Health Study male firefighters (blue) versus in US males based on Surveillance, Epidemiology and End Results Program data (green). (B–D) Show estimated yearly incidence rates for non-Hodgkin lymphoma, melanoma and lung cancer, respectively, in the above three populations. Rates were adjusted for race/ethnicity and 5-year age group. CFHS, Career Firefighter Health Study; FDNY, Fire Department of the City of New York; SEER, Surveillance, Epidemiology, and End Results Program.
Table 3A displays results of SIR analyses comparing cancer incidence in the FDNY and CFHS cohorts with expected numbers based on SEER-21 rates. In the FDNY cohort, SIRs for all cancers, prostate cancer, thyroid cancer, melanoma of the skin, and non-Hodgkin lymphoma were significantly elevated, whereas among CFHS firefighters, prostate cancer and melanoma SIRs were significantly elevated. Lung cancer incidence was significantly lower than expectation in both cohorts.
Standardised incidence ratios (SIRs) of cancers in male FDNY and CFHS firefighters versus US males,24 11 September 2001–31 December 2016
After correction for possible surveillance bias by delaying the diagnosis dates of certain cancer cases by 2 years, the FDNY all-cancer incidence remained higher than expected compared with the US male population (SIR=1.09; 95% CI 1.02 to 1.16), as did the incidence of prostate cancer, thyroid cancer and melanoma (table 3B). In a sensitivity analysis that delayed diagnosis dates by 5 years, all-cancer incidence was no longer significantly elevated in the FDNY cohort versus the US male population. SIRs for prostate and thyroid cancer were attenuated, but continued to show modestly higher rates in the FDNY cohort (data not shown).
Standardised incidence ratios (SIRs) of cancers in male FDNY firefighters versus US males,24 11 September 2001–31 December 2016, after 2-year adjustment for potential surveillance bias
Cancer rates in FDNY compared with CFHS
Comparing the FDNY and CFHS cohorts directly, the FDNY cohort had significantly higher rates of all cancers, prostate and thyroid cancer (table 4). A sensitivity analysis that included only first primary cancer cases when estimating RRs showed similar associations between firefighter cohort and all cancer, prostate and thyroid cancer rates (data not shown). Race/ethnicity was generally not associated with cancer in the above models, although non-Hispanic Black race was significantly associated with prostate cancer (RR vs non-Hispanic white=1.89, 95% CI 1.55 to 2.31).
Adjusted relative rates (RR) and 2-year surveillance bias-adjusted RR of cancers in WTC-exposed male FDNY firefighters versus male CFHS firefighters, 11 September 2001–31 December 2016
Table 4 also shows results corrected for potential surveillance bias in FDNY using a 2-year lag in diagnosis dates of certain cancers: after correction, the RRs were slightly attenuated, but prostate and thyroid cancer rates remained significantly elevated in FDNY firefighters. In sensitivity analyses which used a 5-year lag in diagnosis dates, the RRs were further attenuated for all cancers and for prostate, lung and thyroid cancer (data not shown). Rates of prostate and thyroid cancer in the FDNY cohort, while still elevated, were no longer significantly different from the CFHS rates.
In the analysis restricted to individuals for whom we had smoking information (N=13 579), the all-cancer RR was 15% higher in ever smokers versus never smokers, controlling for demographics and cohort membership (95% CI 1.02 to 1.30). Overall, >80% of lung cancer cases in this subpopulation (43/52) were reported in ever smokers. After controlling for smoking status and demographics, FDNY members had higher rates of all cancer and of prostate cancer compared with CFHS (RR=1.26, 95% CI 1.09 to 1.45 and RR=1.29, 95% CI 1.05 to 1.59, respectively.) Finally, when restricting our primary RR analyses to the FDNY population (N=10 786) we did not observe an association between increasing WTC exposure level and cancer rate (all-cancer RR=1.00, 95% CI 0.94 to 1.07).
Discussion
On this, the 20th anniversary of 9/11, we set out to compare cancer rates in two firefighter cohorts, the WTC-exposed FDNY cohort and the non-WTC-exposed CFHS cohort, to each other and to rates among demographically similar men in the US population (SEER-21). The current investigation extended our previous study, which used CFHS data to estimate excess risk in WTC-exposed firefighters through 2009.20 Consistent with the previous study, we continue to report evidence of excess thyroid and prostate cancer risk in the FDNY firefighters compared with CFHS firefighters. Unlike in the previous study, however, we now also report excess risk for all-cancers combined.
We documented modest excesses of cancer risk in the WTC-exposed FDNY cohort in relation to each comparison group. First, comparing FDNY to the CFHS cohort, we found a 13% excess risk for all cancers, largely driven by prostate and thyroid cancer. After correction for possible surveillance bias in FDNY by delaying diagnosis dates of certain cancer cases by 2 and then 5 years, excess risks were substantially reduced. Some proportion of the excess prostate cancer risk may be due to WTC exposure on top of usual firefighting risks, as some chemicals, like PCBs, commonly found at building sites including the WTC, are known endocrine disruptors, interfering with androgen metabolism.27 This may have elevated the bioavailability of androgen, which could have been a factor in prostate cancer initiation. However, non-WTC-exposed firefighters may also be at risk of PCB exposure through usual firefighting exposures.2 There is little biological evidence for increased thyroid cancer risk from exposures to environmental risk factors other than ionising radiation,28 which was not detected at the WTC site. There is some evidence regarding thyroid cancer in pesticide-exposed workers29–31; pesticides, however, were also not reported at the site.11–13 Alternatively, high rates of some cancers, including thyroid and prostate cancers, could have resulted from non-biological factors like enrollment in screening programmes,32 especially WTC-related health programmes.17–20 33–35 Evidence for non-biological factors due to screening include younger median age at diagnosis among the FDNY cohort for all cancers and cancer subtypes compared with CFHS and SEER-21.25 While the median ages at diagnosis were lowest for FDNY, CFHS median ages were also generally lower than SEER-21. Additional support for non-biological factors can be found in the staging data: cancers reported in SEER-21 were less likely to be classified as localised at time of diagnosis, although data from SEER-21 contained more unknown stages than either FDNY or CFHS. Occupational and WTC-related health programmes are designed for the early detection of cancer to minimise harm and improve survival. They clearly succeed in this mission, but may also overdiagnose occult, asymptomatic cancers.17–19 34 36
Previous evidence from five non-WTC-exposed firefighter studies consistently supports excess risks of prostate cancer and melanoma in firefighters.4 8–10 37 In our analyses, both firefighter cohorts had elevated rates of prostate cancer and melanoma relative to US males, although the SIRs for FDNY were higher. We proposed possible reasons for excess prostate cancer in firefighters above. As for melanoma, beyond UV exposure, melanoma has also been associated with PAH, PCB, aromatic hydrocarbons and other chemicals identified as present at the WTC11 13 and at non-WTC-related fires.38
Compared with US males, the FDNY cohort also had significantly elevated SIRs for all cancer, non-Hodgkin lymphoma and thyroid cancer. The elevated all-cancer risk was driven by prostate cancer. After correcting for possible surveillance bias, we similarly observed elevated, although attenuated, SIRs. Despite our control efforts, surveillance bias concerns remain, as the US general population lacks access to comprehensive, no-copay healthcare like the WTC Health Program.34
The comparison group of CFHS firefighters is based on a subset of the original NIOSH cohort of 29 992 career firefighters.4 Cancer data from the original cohort study accrued from 1985 to 2009, whereas our study began and ended later, covering the time period between 9/2001 and 12/2016. Thus, the current CFHS cohort markedly differs from the original study cohort, which likely explains differences observed. For example, compared with the US population, the earlier study found an all-cancer SIR of 1.09 (1.06–1.12) and lung cancer SIR of 1.12 (1.04–1.21),4 whereas we report CFHS SIRs of 1.05 (0.98–1.12) and 0.71 (0.57–0.89), respectively. We attribute these differences to our use of the truncated cohort (those active on 9/11), which resulted in a younger and more recently employed group.
Notably, both firefighter groups had lower than expected rates of lung cancer when compared with US males, probably due to lower current smoking rates: 3.5%, 6.6% and 15.0% in the FDNY, CFHS, and US male populations, respectively.39 Among firefighters with smoking data, ever smokers demonstrated higher overall cancer rates than never smokers. Differences in incident cancers may also be attributed to a previously described secular trend of declining cancer rates in firefighters hired since 1970, generally attributed to better personal protective equipment (PPE).10
Regular assessment of cancer risk in firefighters remains imperative because firefighting continues to be a common career and volunteer activity. Building contents (synthetics and plastics), fire suppression materials and PPE change over time and over geographic regions—facts which may explain inconsistent cancer results from previous studies.3–10 37 For example, The International Agency for Research on Cancer has classified perfluoroalkyl, a chemical used during suppression activities, as possibly carcinogenic to humans,40 but has not yet fully evaluated this possibility. Differences in rates should also be considered in the context of observed behavioural changes (eg, diet, smoking, alcohol use and sunblock use) and in diagnostic testing (access and technology).
Finally, assessment of cancer risk in FDNY firefighters who worked at the WTC site remains complex; these firefighters were subject to carcinogenic exposures, while also enduring enormous physical and mental burdens related to the attacks. Examination of longitudinal FDNY, CFHS and SEER-21 data by calendar year shows elevated cancer rates in the FDNY cohort, particularly prostate cancer between 2008 and 2012. While these increased rates may be driven by higher participation in medical monitoring after 2007, they could also reflect prostate cancer latency.41 Evidence is slowly accruing about cancer and other long latency illnesses in relation to WTC exposure, although much remains to be determined. Molecular epidemiological studies of biomarkers may provide better understanding of chronic disease development in firefighters, both WTC-exposed and non-WTC-exposed.
Strengths of this study include the use of two different comparison groups to assess excess cancer risk in the WTC-exposed FDNY cohort, an achievement that no other group that we know of has been able to claim. Thus, we were able to report WTC-exposed firefighter cancer risk versus risk in other firefighters and WTC-exposed risk versus risk in demographically similar US males. In addition, we restricted analyses to firefighters actively employed on and after 9/11 not only to allow for WTC exposure comparison, but also so that findings would be relevant to firefighting in modern structures and PPE. Additional strengths include the lengthy follow-up time for each cohort (~15 years), and that smoking history was accounted for in those with available information.
Weaknesses include limitations common to all observational studies, that confounding may be insufficiently controlled in analyses, especially as we had more data from FDNY than from CFHS. For example, smoking history was available for nearly all FDNY firefighters but only for the 32% of CFHS firefighters who completed the CFHS survey. Similarly, we had incomplete information on WTC exposure in the CFHS cohort. If CFHS firefighters who volunteered at the WTC site had exposures similar to those of active duty FDNY firefighters, misclassifying these CFHS members as non-WTC-exposed would have biased our estimated cancer RRs towards the null. Another limitation was that correcting for surveillance bias by lagging FDNY diagnosis dates of certain cancers was an imperfect way to mitigate screening effects, as the 2-year lag time may be insufficient. We found that applying a 5-year delay to the diagnosis dates mostly removed the excess cancer incidence observed in WTC-exposed FDNY firefighters. Asymptomatic cases in the US population, and to a lesser extent in the CFHS cohort, may go undiagnosed without regular physical exams or adherence to screening programmes. However, as cancer screening guidelines such as those from the US Preventive Service Task Force (USPSTF)42 and the American Cancer Society43 become more widely accepted, these differences should become less pronounced. For firefighters, these cancer screening guidelines have been recommended since 1997 by the International Association of Firefighters.44 Although the fire departments represented in the CFHS cohort have had far less funding for cancer screening than FDNY, adjustment for surveillance bias only in the FDNY cohort could have led to an overestimation of this bias if the other departments’ screening practices are similar. Alternatively, if the fire departments in CFHS followed the 2012 USPSTF prostate cancer screening guidelines recommending against PSA screening between 2012 and 2016,45 while FDNY continued to carry out PSA screening throughout the follow-up period, the estimated RR for prostate cancer may have been biased away from the null. In a future study, we plan to further address potential surveillance bias by examining cause-specific mortality in the FDNY and CFHS populations, particularly among those diagnosed with cancer, as our current study found that the proportion of firefighters alive at the end of follow-up was greater in FDNY than in CFHS.
Clearer understanding of the WTC-related cancer risk for firefighters requires progress in at least two directions: additional years of follow-up to allow for the suspected long latency of some solid tumours; and, modelling studies (laboratory or animal based) to identify and track workplace exposures in WTC-exposed and non-WTC-exposed firefighters. These steps may aid our understanding of the complex relationships between WTC exposure, firefighting and cancer.
Data availability statement
Reasonable requests for deidentified data will be considered by the investigators and the National Institute for Occupational Safety and Health.
Ethics statements
Patient consent for publication
Ethics approval
This study was approved by the Albert Einstein College of Medicine Institutional Review Board.
Acknowledgments
We thank the 15 state cancer registries for carrying out record linkages: Arizona Cancer Registry Department of Health Services (DOHS); California Cancer Registry, Department of Public Health (DPH); Connecticut Tumor Registry, Connecticut DPH; Florida Cancer Registry, Florida Department of Health (DOH); Illinois State Cancer Registry, Illinois DOH; Indiana Cancer Registry, Indiana State (DOH); Michigan Cancer Registry, Michigan Department of Health and Human Services (MDHHS); New Jersey State Cancer Registry, New Jersey DOH and Rutgers Cancer Institute of New Jersey; New York State Cancer Registry, Bureau of Cancer Epidemiology, New York State DOH; North Carolina Central Cancer Registry, North Carolina State Center for Health Statistics; Oregon State Cancer Registry, Oregon Health Authority Division of Public Health (OHA DPH); Pennsylvania Cancer Registry, Bureau of Health Statistics and Research, Pennsylvania DOH; South Carolina Central Cancer Registry, South Carolina Department of Health and Environmental Control (DHEC); Virginia Cancer Registry, Virginia DOH, and Washington State Cancer Registry, Washington DOH. Additional Acknowledgements and Disclaimers from individual State Cancer Registries: The collection of cancer incidence data used in this study was supported by the California Department of Public Health pursuant to California Health and Safety Code Section 103885; Centers for Disease Control and Prevention’s (CDC) National Program of Cancer Registries, under cooperative agreement 5NU58DP006344; the National Cancer Institute’s Surveillance, Epidemiology and End Results Program under contract HHSN261201800032I awarded to the University of California, San Francisco, contract HHSN261201800015I awarded to the University of Southern California, and contract HHSN261201800009I awarded to the Public Health Institute. The ideas and opinions expressed herein are those of the author(s) and do not necessarily reflect the opinions of the State of California, Department of Public Health, the National Cancer Institute, and the Centers for Disease Control and Prevention or their Contractors and Subcontractors. The Connecticut Department of Public Health Human Investigations Committee approved this research project, which used data obtained from the Connecticut Department of Public Health. The Connecticut Department of Public Health does not endorse or assume any responsibility for any analyses, interpretations or conclusions based on the data. The authors assume full responsibility for all such analyses, interpretations and conclusions. The Florida cancer incidence data used in this report were collected by the Florida Cancer Data System (FCDS), the statewide cancer registry funded by the Florida Department of Health (DOH) and the Centers for Disease Control and Preventions National Program of Cancer Registries (CDC-NPCR). The views expressed herein are solely those of the author(s) and not necessarily reflect those of the DOH or CDC-NPCR. The Institution will acknowledge the “Illinois Department of Public Health, Illinois State Cancer Registry” as the data source in any and all publications and presentations based on these data. The Institution will state in any publication which quotes the Data provided that the conclusions, opinions, or recommendations in the article are not necessarily the conclusions, opinions, or recommendations of the Department. Furthermore, the Institution will not make any verbal or written representations or statements in any forum that his or her study, publication, or research findings are promoted, endorsed, or supported by the Department. The collection of New York cancer incidence data used in this study was funded in part by the Centers for Disease Control and Prevention’s (CDC) National Program of Cancer Registries through cooperative agreement 6NU58DP006309 awarded to the New York State Department of Health (NYSDOH) and by the National Cancer Institute (NCI), National Institutes of Health, Department of Health and Human Services, under Contract 75N91018D00005. The contents are solely the responsibility of the authors and do not necessarily represent the official views of the NYSDOH, CDC or NCI. This research article is in part based on cancer data provided by the Oregon State Cancer Registry, one of the participating registries funded by the National Program of Cancer Registries (NPCR) under the Centers for Disease Control and Prevention (CDC). These data were supplied by the Bureau of Health Statistics & Registries, Pennsylvania Department of Health, Harrisburg, Pennsylvania. The Pennsylvania Department of Health specifically disclaims responsibility for any analyses, interpretations or conclusions.
References
Footnotes
Contributors MPW designed the study, with significant input from DJP and RZ-O. RZ-O, AS, JS, NJ, RDD and MS acquired the data. RZ-O, AS, CBH and DGG analysed and interpreted the data. MPW drafted the manuscript, with critical revisions from DJP, RZ-O, AS, JS, CBH, RDD and MS. DGG validated the analyses. All authors approved the final manuscript. RZ-O and AS had full access to all the data in the study and take responsibility for the integrity of the data and the accuracy of the data analysis.
Funding This research was supported through the National Institute for Occupational Safety and Health (NIOSH) cooperative agreement numbers U01 OH011309 and U01 OHO11934 and contracts (200-2011-39383, 200-2011-39378, 200-2017-93426, 200-2017-93326).
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.