Article Text

Abstract
Objectives Work disability management is a problem globally. This study was designed to find out whether the initiation, process and outcome of health check-ups (HCUs) follow the national legislation and whether supervisors and occupational healthcare (OHC) units act according to the legislation-based recommendations.
Methods Data of 1092 employees with reduced work ability were collected during 2013–2018 in 15 OHC units across Finland. Nine reasons for HCUs, eight process activities and three recommendations were analysed. Cross-tabulation and multinomial logistic regression analysis were used in the analyses.
Results Employees themselves initiated an HCU for early support more often (OR with 95% CI 2.37; 1.04 to 5.40) compared with supervisors. Personnel in OHC units initiated an HCU in musculoskeletal disorders more often (OR 1.58; 95% CI 1.05 to 2.37) and in mental disorders less often (OR 0.52; 95% CI 0.35 to 0.76) compared with supervisors. These findings were reflected in the recommendations after the HCU, where rehabilitation was recommended for employees with musculoskeletal disorders more often than for employees with mental disorders (ORs 5.48; 95% CI 1.91 to 15.67 and 1.59; 95% CI 0.74 to 3.43, respectively).
Conclusion Supervisors and OHC units followed the recommendations for management of work disability to a great extent. Employees were active in looking for help early when they had problems with work ability. This positive finding should be promoted even more. OHC units did not initiate HCUs or recommend rehabilitation in mental disorders as actively as they did in musculoskeletal disorders. Support of employees with mental disorders should be improved and studied more.
Registration of the study
The study protocol was approved and registered on 22 September 2017 by the Doctoral Program of Health Sciences, Faculty of Medicine, University of Eastern Finland, registration no. 189067.
- Rehabilitation
- Health services research
- Occupational Health Services
- Retirement
- Disabled Persons
Data availability statement
Data are available on reasonable request. Requests to access data should be addressed to the second author: klas.winell@conmedic.fi. Anonymised participant data will be available on request, from February 2023 to January 2029, to researchers who provide a methodologically sound scientific proposal that has been approved by an ethics committee and the scientific board of Conmedic Ltd.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
WHAT IS ALREADY KNOWN ON THIS TOPIC
Premature retirement due to disability and management of work disability issues are major socioeconomic challenges globally.
Targeted health check-ups may be useful to uncover risks of sickness absence and to launch the process to support work ability.
WHAT THIS STUDY ADDS
Supervisors and occupational healthcare followed the legislation-based recommendations for management of work disability to a great extent.
In mental health and alcohol problems, supervisors were most active in launching the health check-up process.
Employees were active to get early support to their work ability problem.
The occupational healthcare personnel were more active to initiate disability management in musculoskeletal problems than in mental problems.
HOW THIS STUDY MIGHT AFFECT RESEARCH, PRACTICE OR POLICY
Support of occupational healthcare should be improved and studied in mental disorders.
Employees can be encouraged to launch the disability management process when they experience reduced work ability.
Introduction
Management of work disability is a universal problem,1 2 while premature termination of careers due to work disability is one of the major socioeconomic challenges globally.3 However, the solutions and the activity to manage work disability may differ across countries.1 2 4 Generally, the emphasis of occupational healthcare (OHC) is to promote healthy workplaces and prevent accidents and hazards in workplaces,5 but the ageing of the workforce also calls for active preventive interventions of OHC units.6
In Finland, targeted health check-ups (HCUs) in OHC are a way to identify work disability risks,7 but they are at the same time interventions to verify and promote employees’ work ability.8 Work disability due to work-related or other illnesses and injuries account for some 80% of the HCU interventions in Finland.9 Mental and musculoskeletal disorders are responsible for a major part of all disability pensions.10 Moreover, hazardous alcohol use is associated with disability retirement due to mental disorders.11 Therefore, HCUs may be useful to uncover risks of sickness absence12 and disability retirement.13
Some two-thirds of employees participate annually in the regular targeted HCUs in Finland,9 which is more than in many other countries.14–16 HCUs are regulated either by the Occupational Health Act17 or the Government Decree on Health Checks for Hazardous Work.18 Targeted HCUs should include the identification of the disability risk, a return-to-work plan, and a health promotion plan, and have predictive value.19 Targeted HCUs for employees with work disabilities, followed by health promotion and workplace interventions in both musculoskeletal and mental disorders, may reduce disability20 and be effective in improving work participation.21 Furthermore, targeted HCUs for ageing employees may be effective in reducing sickness absence, especially among men.8
The loss of productivity through disability retirement and sickness absence may be threefold compared with the expenses of work ability management.22 Factors that reduce disability costs are co-operation of employers, employees and personnel in OHC units without barriers, visibility of the goals of work ability management, ability to focus the work ability management processes to the highest work disability risks, and the facilitation of multiactor co-operation through coordination and communication.22 This means an active collaboration between the workplace and OHC unit in the work ability management process.23 24 Employers’ (supervisors’) level of activity in work ability management differs, being lowest in small enterprises and low-wage service-oriented sectors.4 Supervisors’ activity and skills affect work-related sickness absence and disability retirement incidence.25 According to the report of the Organisation for Economic Co-operation and Development from 27 countries in 2010, a combination of obligations and financial incentives for employers can reduce both sickness absence and disability rates.3
Several amendments were introduced to the Employees’ Pension Act in 2006 in Finland. For example, an employee is entitled to receive appropriate vocational rehabilitation to prevent disability and improve working capacity.26 Some important amendments were introduced to the Occupational Healthcare Act and Health Insurance Act in 2012. The legislation obligates supervisors to inform their OHC unit when an employee has been on sick leave for 30 or more calendar days (the 30-day rule) and to send a bill on daily allowance to the Social Insurance Institution (Kela) within 60 days. An HCU by an occupational physician is required if work disability persists for more than 90 compensated days (the 90-day rule). This check-up should include an examination of work disability, as well as remaining work ability and identification of potential job design and rehabilitation possibilities in order to prevent unnecessary prolongation of absence from work. OHC units have a coordinating role in tripartite negotiations about work modifications with the employee and the supervisor. For the employee, concerning the support of work ability, there are no other obligations in the Finnish law but to participate in HCUs due to hazardous work or disability problems and to cooperate with supervisors and OHC personnel.24 All the guidelines for OHC, such as the Good practice in OHC and HCUs in OHC, are strongly based on the legislation.
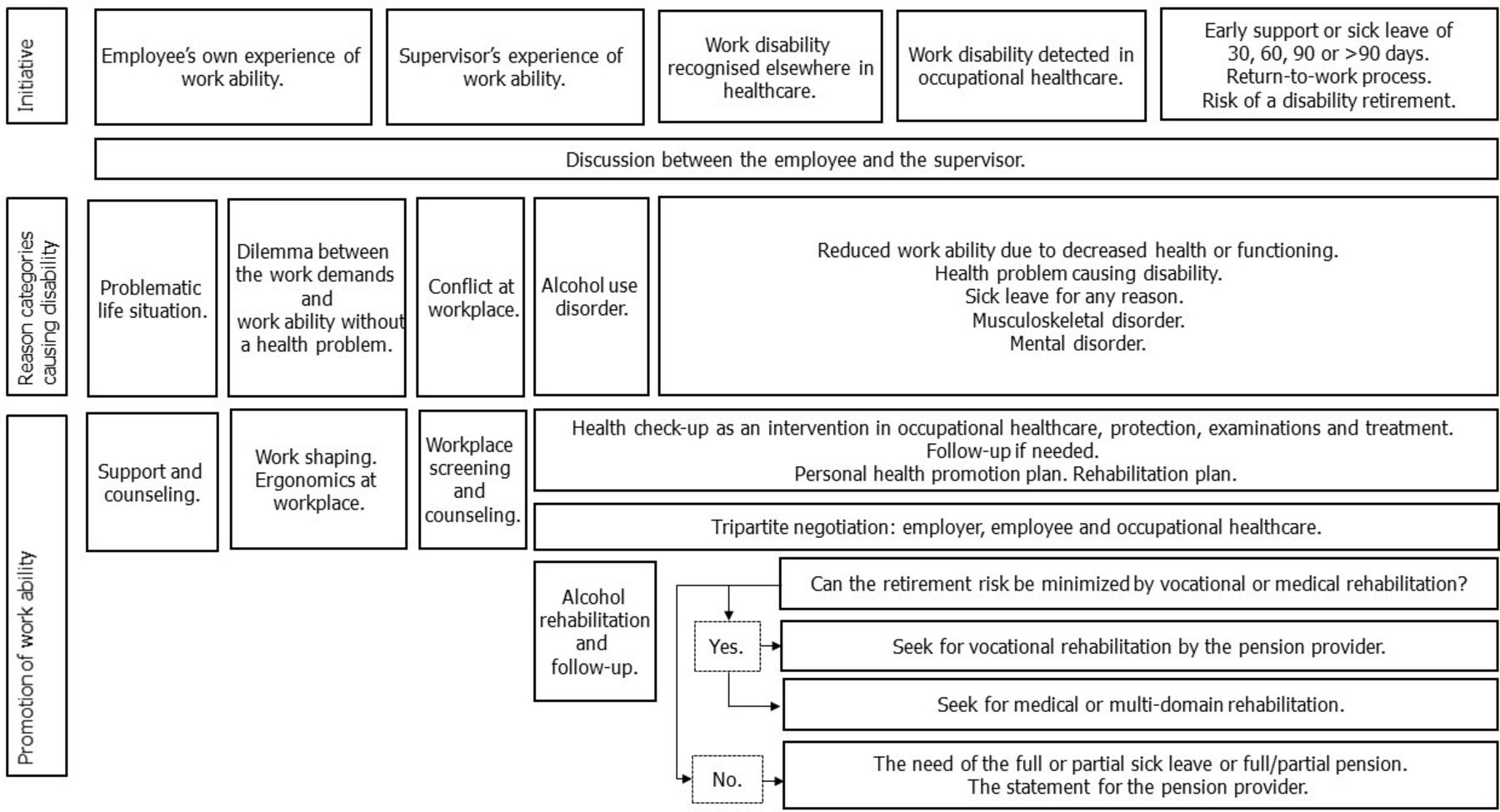
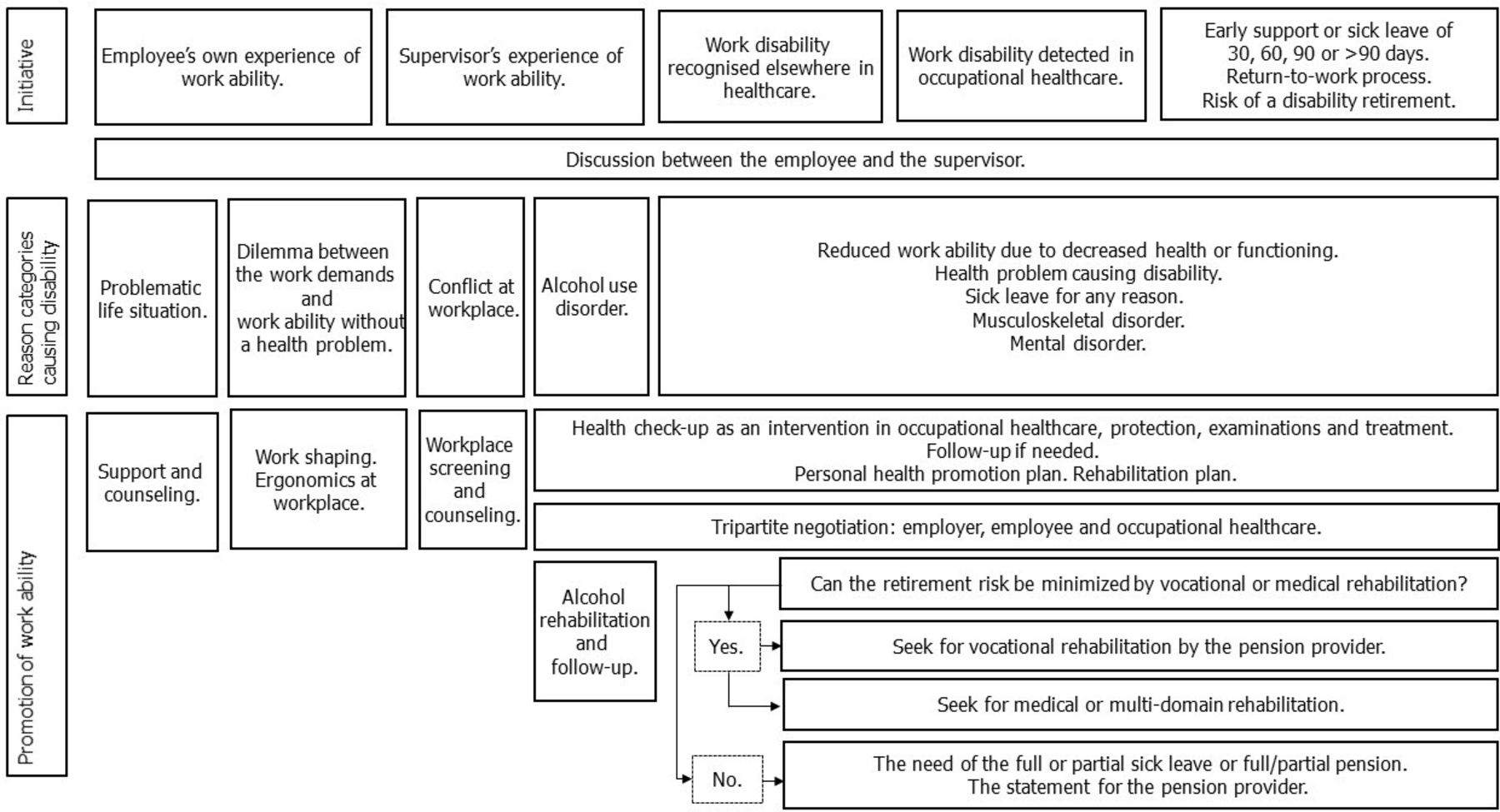
Information is scarce on how the activity of employees, supervisors and personnel of OHC units in managing work disability in real life affects the HCU process and support of employees with work disability problems. Different possibilities in achievement of work support for employees with reduced work ability in Finland are presented in figure 1. We hypothesised that the initiation, process and outcome of HCUs differ depending on which partner initiated the HCU process.
{kind=link}
Different possibilities in achievement of work support for employees with reduced work ability in Finland are presented in figure 1. HCU, health check-up.
Our research questions were: #1: Do the initiation, process and outcome of HCU differ depending on which partner initiated the HCU process? #2: Do the OHC personnel and employers perform their recommended tasks in the HCU process?
Materials and Methods
Data collection
The anonymous data on HCUs (N=2908) were collected annually to the electronic platform over the course of 2 weeks by OHC physicians and nurses when performing HCUs. The target population of HCUs were employees with potential work hazards and those with work ability problems. Data on HCUs were collected for quality improvement purposes in 15 OHC units of the Finnish Occupational Health Quality Network in all parts of Finland during the years 2013–2018. Data only from patients with work ability problems (N=1092) were included in this study. An annual sample of 1%–2% of employees registered in OHC unit was considered to power the quality measurement analyses of the OHC unit. In this cross-sectional questionnaire-based study, the principal occupational sectors comprised administration, planning, research, office, customer service, health, social work, education, culture, technique, production and security were represented in both public and private sectors. The size of the enterprises varied from small, having less than ten employees, to large, having over 1000 employees. The mean age in the study population varied, being 45.6 years in 2016 in the most active OHC unit. We did not have more detailed socioeconomic data of employees, because our main study target was to investigate the activity of the employers and OHC personnel in the process.
The quality measurement checked the performance of OHC personnel in the HCUs of employees with reduced work ability, working despite permanent work disability, on sick leave or at risk of needing sick leave (early support). The initiative to perform an HCU came from one of the three partners: supervisor, employee or OHC personnel. There is a legislative request in Finland that the supervisor should be active in initiating an HCU if the employee has problems with work ability. The data gathered included the reason for HCU, making a health promotion plan, checking the possibility of partial sick leave, tripartite (ie, employee, employer and OHC) negotiation performed, checking the need for a rehabilitation plan, and return-to-work activity started. Additional data on HCU process activities was collected from the OHC units in 2016–2018 (N=790). The items gathered in data collection and the data flow are described in online supplemental figure 1. A thorough description of the Finnish Occupational Health Quality Network and data collection has been published previously.27
Supplemental material
We followed the STROBE (strengthening the reporting of observational studies in epidemiology) statement in the set up of the study.28
Data variables
Nine reasons for HCUs, eight process activities and three outcomes were compared in the analyses (table 1). All of the outcome and predictor variables were categorical.
The reasons for health check-up (HCU), process activities of HCU and outcomes of HCU that were tested to determine how the activity of the supervisors (employers) and occupational healthcare in work ability management in real life affects the HCU in 15 occupational healthcare units in Finland during 2013–2018 (N=1092)
Statistical methods
We calculated ORs for partners to initiate an HCU using the supervisor initiative and 30-day sick leave as references to find out if the activity of initiation differed in the nine reasons for HCUs.
ORs were also calculated to find out if the activity to perform the eight process activities differed during the HCU process depending on the reason for HCU, using the sick leave of more than 90 days HCU and process activity not performed as references.
Finally, ORs were calculated for the outcomes (recommendations) of HCU, and the medical reasons (musculoskeletal disorder, mental disorder or alcohol use disorder) for HCU and activities performed in HCUs to reach the outcome. As reference, we used 30-day sick leave and not getting a recommendation.
Due to the lack of adjustment variables, only models with one dependent variable and one predictor variable were used. To make this even more clear, our dependent variable was often multinomial (multiple groups), leading to multinomial logistic regression model. In the model, one response variable level works as a reference, and the other levels are compared with it. If there are only two response variable levels, the result is only one OR with its CIs, and the model works as a binary logistic regression model. Thus, univariate multinomial regression model leads to multiple ORs reported in the tables. Cross-tabulation was used to confirm that the interpretations were valid.
The classes which lacked data so much that the model fitting algorithm did not converge are reported in the tables with the abbreviation NA. The abbreviation NE means that the process is not expected to be done with the employee due to the category of disability problem. The analyses which report ORs should be considered as complete case analysis, which ignores the missing data mechanism and essentially assumes that our sample is representative.29
Statistical analyses were run with multinomial logistic regression analysis by using R programming language V.4.2.030 and multinom-function in nnet-package.31 The p values <0.05 were addressed as statistically significant.
Results
Both personnel in the OHC units (OR with 95% CI 0.23; 0.12 to 0.46) and employees (OR 0.10; 95% CI 0.03 to 0.29) initiated the HCU less often compared with supervisors when the employee had alcohol use disorder. OHC personnel also initiated HCUs less often (OR 0.52; 95% CI 0.35 to 0.76) compared with supervisors when the employee had a mental disorder (table 2). OHC personnel initiated the HCU more often when the employee had permanently reduced work ability (OR 6.36; 95% CI 2.81 to 14.43), had been on sick leave 90 days (OR 5.97; 95% CI 2.02 to 17.67) or longer (OR3.51; 95% CI 1.47 to 8.38), or had a musculoskeletal disorder (OR 1.58; 95% CI 1.05 to 2.37). Employees were more active in initiating an HCU for early support (OR 2.37; 95% CI 1.04 to 5.40) compared with supervisors (table 2).
The ORs with a 95% CI and p values of the activity of employees and occupational healthcare compared with supervisors (employers) in initiating a health check-up (HCU) in different situations of work ability/disability; preventive care; problems with work ability; and illness in 15 occupational healthcare units in Finland during 2013–2018
In the process activities of an HCU, employees on 60-day sick leave and with permanently reduced work ability had a personal health promotion plan made more often (OR 2.10; 95% CI 1.01 to 4.37 and 1.87; 95% CI 1.22 to 2.88, respectively) than other employees with disability. With employees on 90-day sick leave had tripartite negotiation taken place less often than with those with a longer-than-90-day sick leave (OR 0.40; 95% CI 0.21 to 0.77). Even their work ability maintenance started less often (OR 0.36; 95% CI 0.19 to 0.69) and they received fewer recommendations for work ability maintenance during the HCU compared with those on a longer-than-90-day sick leave (table 3).
The ORs with a 95% CI of occupational healthcare’s activity in performing recommended activities in 790 health check-ups (HCUs) to assess and promote employees’ work ability, depending on the reason for HCU (early support, duration of sick leave or permanently reduced work ability), compared with patients attending an HCU for more than 90-day sick leave (N=122) in 15 occupational healthcare units in Finland during 2016–2018
There were small differences in the process activities performed during the HCU while preparing for the OHC physician’s recommendation. Tripartite negotiation took place more often among those who were recommended for partial or full pension (OR 4.5; 95% CI 1.14 to 17.68) (table 4). A musculoskeletal disorder was a strong predictor of a recommendation for rehabilitation (OR 5.48; 95% CI 1.92 to 15.67) and partial or full disability pension (OR 3.04; 95% CI 1.04 to 8.91). A mental disorder did not predict a recommendation for rehabilitation (OR 1.59; 95% CI 0.74 to 3.43).
The ORs with a 95% CI of the outcomes (recommendation of rehabilitation by the occupational healthcare physician, continued sick leave or pension), medical reasons for the outcomes and process activities performed in 1092 health check-ups (HCUs) to reach the outcomes compared with patients on 30-day sick leave and those who did not get a recommendation in 15 occupational healthcare units in Finland during 2013–2018
Recommendations for rehabilitation became more frequent the longer the sick leave. ORs at 90-day and longer-than-90-day sick leaves were 9.60; 95% CI 1.84 to 62.13 and 5.88; 95% CI 1.11 to 31.15, respectively (table 4).
There were also many non-significant or negative findings in this study. The employees’ and supervisor’s activity to initiate an HCU did not differ in work ability problems due to mental or musculoskeletal disorder, OR 0.97, 95% CI 0.64 to 1.47 and OR 0.72, 95% CI 0.47 to 1.1, respectively (table 2). A negative finding was that the need for a partial sick leave was not assessed when the patient had a sick leave of 30 days (OR 0.32, 95% CI 0.13 to 0.80) (table 3).
Discussion
One of our main findings was that employees often initiated an HCU to get early support for their work ability. In alcohol use disorder, supervisors were active in initiating the HCU, and OHC initiated HCUs of employees with long sick leave and permanently reduced work ability. OHC was not active in initiating HCUs of employees with mental disorder. OHC physicians actively recommended rehabilitation at 90-day and longer sick leaves, and rehabilitation recommendations took place often with musculoskeletal disorders.
Employees looked for early support almost 2.5 times more often than their supervisors sent them to an HCU for early support. This was a very positive finding, because it means that employees understand they must thrive to keep up their work ability and must build resilience to disabilities in work.32
Supervisors were most active in initiating an HCU when the employee had an alcohol use disorder. The explanation may be that employees with alcohol use disorder tend to miss working days due to illness, injury and days skipped.33 Supervisors are often the first to notice the problems in work results.34 Supervisors might also think that alcohol use disorder is a significant risk factor for permanent work disability.35 Finland even has legislation supporting workplaces in maintaining their alcohol and substance abuse prevention programmes,17 where OHC plays a crucial role.
OHC actively initiated HCUs for employees with permanently reduced work ability and long sick leaves (90 days or more). This is also what we expected to happen. OHC especially follows up on musculoskeletal problems, which is understandable because musculoskeletal disorders are a major risk factor for sickness absence36 and disability pension.37 However, OHC was clearly less active in organising HCUs for employees with mental disorders, which we did not expect, because there have been national guidelines for years from the Finnish Institute of Occupational Health to support the work ability of employees with depression in OHC.38 One possible reason behind this finding could be insufficient implementation of the guideline. One can also speculate whether there are less resources in OHC for supporting employees with mental disorders compared with those with musculoskeletal disorders, as has previously been shown for primary healthcare in Finland.39 These findings were also reflected in the recommendations after the HCU, where employees with musculoskeletal disorders received a recommendation for rehabilitation more often than employees with mental disorders.
Our results also support previous results from a randomised controlled trial that early detection of musculoskeletal problems is important in decision making and improvement of ergonomics.40
An interesting finding was that a recommendation for partial or full pension was made so often at HCUs for 60-day sick leave. This finding is not what we expected because there is seldom a need to make a recommendation in such an early phase of sick leave. The result may be due to the small number of recommendations altogether or due to a serious condition like stroke or cancer in the employee.
The findings in the analysis of the process activities during HCUs followed what we expected to happen to a great extent and were thus positive, with the exception of 90-day HCUs, where we saw fewer personal health promotion plans and less work ability maintenance than expected.
Strengths of the study included the study population covering employees across Finland, several OHC units participating and the data we used being real-life data. Still another strength was that we were able to meet the targets of our study that is, to answer about the initiation of HCU and performance of the work ability support process.
To our knowledge, this kind of study has not been performed in Finland before, which also is a strength. Previously, a qualitative study based on 18 interviews in OHC in Finland showed that the personnel did not systematically follow evidence-based recommendations in medical care.41 That study did not explore the matters of work ability maintenance. Our data are genuine from real life, which makes it especially valuable when comparing the results to previous research. Therefore, our findings, although being cross-sectional, brought new results. One of these positive results was that OHC personnel were not the party to initiate work ability support in mental disorders and alcohol use disorder but supervisors did it most often. A novel result was that the legislation-based recommendations were followed to a great extent.
We think that the secondary use of quality improvement data was both a strength and weakness at the same time. A strength was that we gained real-life data. A weakness was that, due to the primary use of data, we did not have many of the important background or adjustment information, for example, socioeconomic status, age, sex, occupational group, size of enterprise. Lack of this information restricted our possibilities to adjust the results and also to assess which factor may or may not have affected the findings. This individual socioeconomic and other background information might have influenced supervisors and OHC personnel’s behaviour in their work.
The risk of an exit from employment due to health issues varies between different occupational groups,42 which is why our results may not be generalised to all occupational groups. The size of the enterprise influences the activity of both OHC and supervisors. To conclude, further research is needed to evaluate to what extent the condition and background of the patient affects the decisions made during the disability management process of OHC. An information bias connected to self-reporting can also exist in this study,43 although we think it is minor because physicians and nurses mainly reported matters that should have taken place earlier and leaving out information was not possible due to the obligatory questions.
Conclusions
Supervisors and OHC personnel followed the legislation for maintenance of work ability to a great extent. Employees were active in looking for help early when they had problems with work ability. This is positive and should be encouraged. Personnel in OHC units were not active in initiating HCUs in mental disorders. This should be improved and studied more.
The targeted HCUs used as interventions are an important component of the Finnish OHC processes. They may work as triggers for interventions to support employees with reduced work ability, while they can also work as interventions themselves. Early detection of problems in work would be beneficial for decision making—for example, to improve working ergonomics.
Data availability statement
Data are available on reasonable request. Requests to access data should be addressed to the second author: klas.winell@conmedic.fi. Anonymised participant data will be available on request, from February 2023 to January 2029, to researchers who provide a methodologically sound scientific proposal that has been approved by an ethics committee and the scientific board of Conmedic Ltd.
Ethics statements
Patient consent for publication
Ethics approval
An ethical review statement from a human sciences ethical committee is not required in this particular study, which is based solely on anonymous documentary data, according to The ethical principles of research with human participants and ethical review in the human sciences in Finland (2019). The study was conducted in accordance with the Declaration of Helsinki.
Acknowledgments
The authors extend their thanks to Mr. Aidan M. Lewis, who provided language and proofreading help.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Contributors JKu and KW have planned the study conception and design, analysed the results, and prepared the manuscript. KW and JKo extracted the data from the registers and prepared it for the analyses. JKo carried out the statistical analyses. KR commented on the manuscript draft. All authors have read and approved the final version of the manuscript to be published. All the authors participated in the agreement to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved. JKu is reponsible of the contents and acts as the guarantor of the article.
Funding JKu has received a grant from Jalmari and Rauha Ahokas Foundation.
Competing interests KW is the owner of Conmedic. The company runs quality improvement networks on a non-profit basis. JKu has received a grant from Jalmari and Rauha Ahokas Foundation. JKo and KR declare no conflicting interests.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.