Article Text

Abstract
Objective The aim of this study was to investigate an integrated mental healthcare and vocational rehabilitation intervention to improve and hasten the process of return-to-work of people on sick leave with anxiety and depression.
Methods In this three-arm, randomised trial, participants were assigned to (1) integrated intervention (INT), (2) improved mental healthcare (MHC) or (3) service as usual (SAU). The primary outcome was time to return-to-work measured at 12-month follow-up. The secondary outcomes were time to return-to-work measured at 6-month follow-up; levels of anxiety, depression, stress symptoms, and social and occupational functioning at 6 months; and return-to-work measured as proportion in work at 12 months.
Results 631 individuals were randomised. INT yielded a higher proportion in work compared with both MHC (56.2% vs 43.7%, p=0.012) and SAU (56.2% vs 45%, p=0.029) at 12-month follow-up. We found no differences in return-to-work in terms of sick leave duration at either 6-month or 12-month follow-up, with the latter being the primary outcome. No differences in anxiety, depression or functioning between INT, MHC and SAU were identified, but INT and MHC showed lower scores on Cohen’s Perceived Stress Scale compared with SAU at 12-month follow-up.
Conclusions Although INT did not hasten the process of return-to-work, it yielded better outcome with regard to proportion in work compared with MHC and SAU. The findings suggest that INT compared with SAU is associated with a few, minor health benefits. Overall, INT yielded slightly better vocational and health outcomes, but the clinical significance of the health advantage is questionable.
Trial registration number NCT02872051.
- occupational health
- psychiatry
Data availability statement
Data are available upon reasonable request.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Key messages
What is already known about this subject?
Sick leave due to anxiety and depression is very frequent, often long term, associated with much suffering for individuals and very costly for societies.
Sick leave duration due to depression can be reduced by workplace interventions combined with clinical and psychological interventions and by improving healthcare, while workplace interventions alone appear to have the opposite effects.
Intervention effects differ greatly between countries with different welfare regimes and support systems.
The effect sizes of the above-mentioned interventions are usually relatively small, while moderate to large effects are observed of lowering the benefit levels or increasing the benefit eligibility criteria, control frequency or intensity.
Only few studies have reported on interventions specifically for persons with anxiety; this group is often only studied in groups with other common mental disorders.
What are the new findings?
Integration of healthcare and vocational rehabilitation yields a higher proportion in work at 12-month follow-up and some health benefits compared with service as usual at 6-month follow-up.
Improved mental healthcare yields some health benefits but no different vocational outcomes compared with service as usual.
How might this impact on policy or clinical practice in the foreseeable future?
While integrating interventions does not hasten return-to-work in the short term, a higher proportion are in work after 1 year.
Subsequently, the goal of a very fast return-to-work is not necessarily beneficial.
Introduction
Background
Anxiety and depression are common mental disorders (CMD) that are widespread and associated with much suffering and functional impairment.1 They account for a large part of the societal economic costs of mental disorders due to their high prevalence and the significant loss of potential labour force through unemployment, sick leave and reduced productivity.1 For most individuals, employment is essential for normal living and can be pivotal to the recovery process after sick leave, especially compared with the effects of unemployment.2
Several factors are important in the return-to-work process among people with CMD, and symptom reduction alone is insufficient.3 Interventions consisting solely of healthcare have shown various vocational outcomes, from no effect4 to small effects.5 In one study, attempts to improve healthcare led to decreased work functioning.6 A recent meta-analysis studied interventions to improve return-to-work among workers with CMD on sick leave. The authors concluded that interventions with multiple components are superior to those with only one component and that the intervention components should include workplace contact and use of graded return-to-work.7 A recent Cochrane review of interventions for depression alone reached somewhat similar conclusions.5
Furthermore, several actors influence both the duration and the quality of the complex return-to-work process.8 Often, healthcare interventions are delivered separately from the vocational rehabilitation services and social insurance provision. This fragmented placement of interventions often entails a lack of coordination, creating frustration among persons on sick leave.8 A 2015 Organisation for Economic Co-operation and Development (OECD) report concluded that there is insufficient coordination between the relevant sectors regarding absentees and has recommended its member countries to ‘experiment with ways to integrate health and employment services’.9
Objectives
The objective of this trial was to investigate the effect of the IBBIS integrated intervention (INT)—an intervention integrating best practice mental healthcare with best practice vocational rehabilitation (IBBIS is a Danish acronym that translates to ‘Integrated Health Care and Vocational Rehabilitation for Sick-Leave Benefit Recipients’). This was compared with two interventions without integration: (1) mental healthcare (MHC), an investigator-directed control group of best practice mental health and standard vocational rehabilitation; and (2) service as usual (SAU), a non-investigator-directed control group of standard mental healthcare and standard vocational rehabilitation. For all outcomes, we hypothesised that INT would yield better outcomes than both MHC and SAU, and MHC better than SAU. The outcomes were time to stable return-to-work, proportion in stable work at follow-up, and self-reported symptoms of anxiety, depression and stress, and functioning level.
Methods
Study setting and context
This study took place in four municipalities in the Capital Region of Denmark, a country with a comprehensive system providing social security10 and healthcare free of charge.11 Compensation for lost work capacity, called sick leave benefit, is governed by municipal jobcentres and is reimbursed to the employer or directly to the person on sick leave if the citizen is unemployed. All sick leave benefit case-handling starts with a meeting at the jobcentre, from where absentees could be referred for study eligibility assessment.
Study design and participants
This study was a randomised controlled trial (RCT). A few minor changes occurred after commencement and these are all described in online supplemental file 1. The design is thoroughly described in a study design article12 and is therefore described only briefly here; further details can be found in online supplemental file 2.
Supplemental material
Supplemental material
Those eligible for participation were aged ≥18 years and in receipt of sick leave benefit for ≥4 weeks due to depression, generalised anxiety disorder, social phobia or panic disorder. Diagnosis and all other eligibility criteria were evaluated by the clinical research staff, guided by the Mini International Neuropsychiatric Interview.13 Participants were required to provide written consent. Those who were ineligible were pregnant, at moderate or higher risk of suicide, had substance abuse disorder, had an unstable medical condition or showed signs of dementia.
Randomisation and masking
A research staff member usually performed the eligibility assessment, inclusion and subsequent randomisation; however, if the assessor was a blinded researcher, randomisation was performed by another staff member. Allocation was performed immediately after assessment using an online service. The allocation sequence was computer-generated with concealed, varying block size and was stratified for diagnosis, municipality and employment status. Only the researchers were blinded until all 12-month analyses were completed, not the staff or the participants at any time.
Procedures
Participants were assessed at baseline and followed up at 6, 12 and 24 months, completing self-report outcome questionnaires. At every follow-up we retrieved register-based data with information per week of the type of received benefit and salary. To monitor protocol adherence regarding intervention implementation, we conducted fidelity reviews. We used a fidelity scale developed for this study, inspired by the one used in the individual placement and support (IPS) intervention.14 It included four categories: integration, organisation, mental healthcare and vocational rehabilitation (see online supplemental file 3 for details). Post-hoc, we counted the total use of services inside and outside the study, respectively (see online supplemental file 3).
Supplemental material
Participants in the SAU group received all services as usual: standard vocational rehabilitation in municipal jobcentres and mental healthcare through their general practitioners (GP). Vocational rehabilitation in the SAU group primarily consists of various short-term programmes, where participants would receive instruction and support for job applications, including how to form a resume, cover letter or application. Some could also have taken part in unpaid internships as a step towards gaining competitive employment.
Participants in the INT group received all interventions via IBBIS. The interventions were (1) best practice vocational rehabilitation and (2) best practice mental healthcare. These two kinds of interventions were integrated: early in each course, at least one physical meeting took place including the participant, the care manager and the employment consultant, together forming a joint plan. Additionally, all team members were co-located, had common training and received regular joint supervision. Best practice vocational rehabilitation in INT consisted of the same support in the job application process, from their employment consultants, as in the SAU group, but also included a much closer support throughout the process, as well as mentoring regarding job interviews, problem solving and how to manage job and illness in their return to work.
In the MHC group, participants received mental healthcare in IBBIS and vocational rehabilitation in municipal jobcentres, without integration. Best practice mental healthcare in the MHC and INT groups complied with the guidelines from the UK National Institute for Health and Care Excellence,15 delivered by care managers who were mostly nurses trained for the study purpose, all of whom had previous experience with mental healthcare.
Outcomes
The primary outcome was time from randomisation to return-to-work, which is the start of a period of stable work, measured at 12 months. Stable work is defined as a period of ≥4 successive weeks without sick leave benefit and with any salary during those weeks, regardless of employment status at baseline. The secondary outcomes were time to return-to-work, measured both at 6 and 24 months, proportion in work at 12 months, and time from first day of return-to-work until possible recurrent sick leave (24-month follow-up). Self-reported secondary outcomes were symptoms of depression, anxiety and stress, and functioning level, measured at 6 months by validated scales.16–19 The predefined exploratory outcome was the total number of weeks at work at 12 months and at 6-month, 12-month and 24-month follow-up the following self-report outcome scales: Four-Dimensional Symptom Questionnaire,20 Karolinska Exhaustion Disorder Scale,21 Illness Perception Questionnaire (IPQ),22 EQ5DL,23 Quality of Life Scale,24 Return to Work Self-Efficacy,25 Generalized Self-Efficacy Scale,26 Stanford Presenteeism Scale,27 and at 6-month follow-up only the Client Satisfaction Questionnaire.28 All 24-month outcomes will be presented elsewhere, along with health economic evaluation.
Statistical analysis
From observations in a similar study population, we expected a mean return-to-work time of 210 days29 and set an HR of 1.5 as the relevant minimal difference. Due to the three-armed design, we set α to 0.0167, while β was set to 0.1. Thus, with an allocation ratio of 1:1:1, we needed 609 participants. All primary and secondary analyses adhered to the intention-to-treat principle. For all time to return-to-work outcomes, we performed Cox regression to calculate hazard rate ratios. For proportion-in-work outcomes, we calculated the OR using logistic regression. For self-reported outcomes, linear mixed-effects models with unstructured covariance yielded group differences. Subgroup analyses were preplanned and performed in the following strata: per diagnosis, per employment status, per IBBIS team, and per first and last half of the participants. Further, all analyses were performed adjusted for the interaction of diagnosis and intervention. Sensitivity analyses were performed in a best-case/worst-case scenario manner. All main and subgroup analyses were performed according to a statistical analysis plan, preregistered at ClinicalTrials.gov.
Results
Enrolment took place between April 2016 and April 2018. A total of 2635 sick leave absentees were referred for assessment of mental health and eligibility. Attempts were made to contact all individuals and 2144 individuals were left for eligibility assessment. Of those assessed, 1513 were excluded from this study; 666 of these had stress-related disorders and were randomised in a parallel RCT. Of those assessed, 760 were not eligible for any of the two RCTs due to them having other mental health disorders. In total, 609 were randomised and included in the intention-to-treat analysis; 22 were erroneously randomised and only included in the sensitivity analyses. The Consolidated Standards of Reporting Trials diagram in figure 1 depicts the participant flow.

Participant flow. IBBIS, Integrated Health Care and Vocational Rehabilitation for Sick-Leave Benefit Recipients; INT, integrated intervention; MHC, mental healthcare; RCT, randomised controlled trial; SAU, service as usual.
Baseline data
Three times as many women as men were enrolled. The mean age was 41.9 years (SD 10.8) and the mean sick leave duration was 11.1 weeks (SD 4.17). There were more participants who were employed than unemployed, and a primary diagnosis of depression was more frequent than anxiety (see table 1 for details).
Baseline characteristics
Implementation and delivery of interventions
The IBBIS mental healthcare was implemented with good fidelity, whereas the IBBIS vocational rehabilitation and integration of services were implemented with fair fidelity. The INT group received less vocational rehabilitation service and integration of services in IBBIS than was planned in the study protocol. Participants in the SAU group received mental healthcare outside the study to an extent that was probably sufficient.
Vocational outcomes
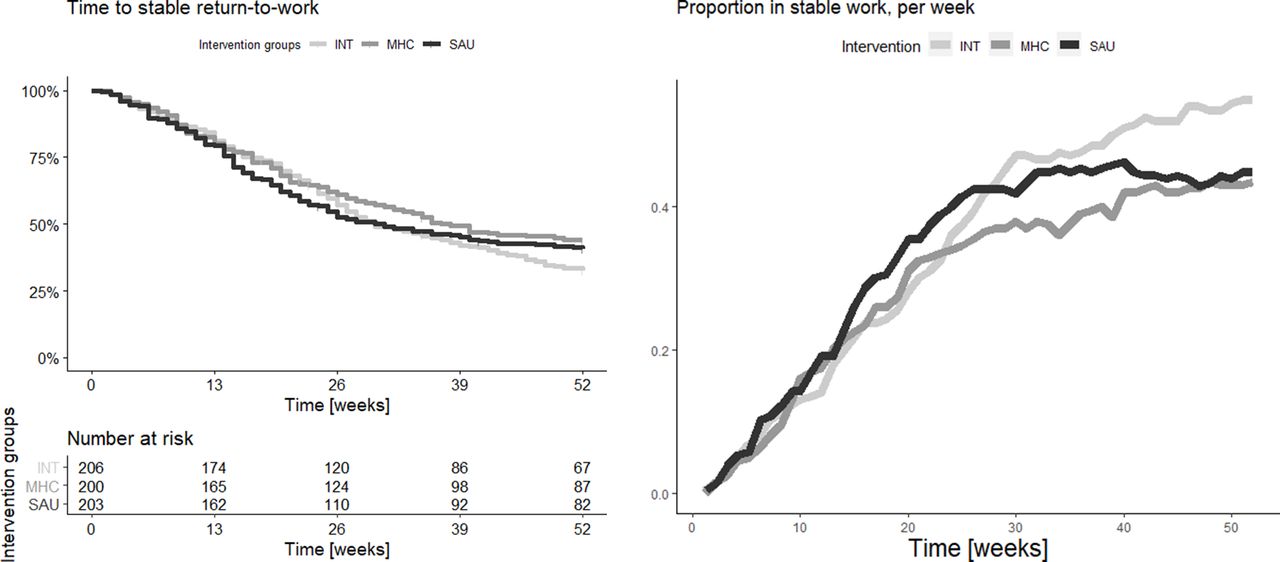
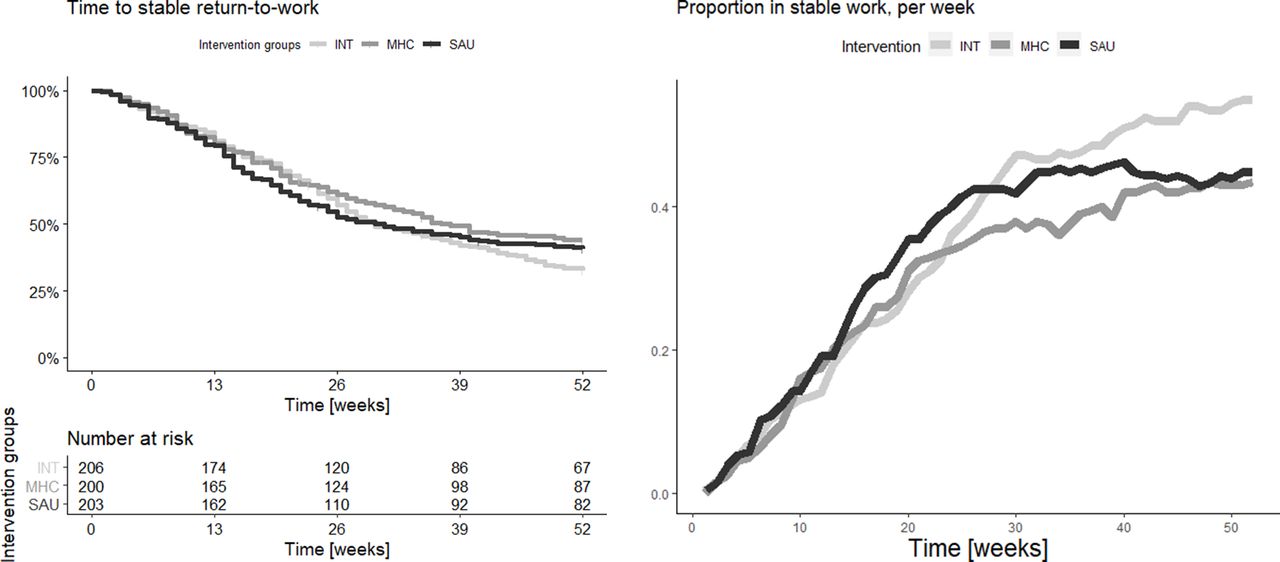
For the primary outcome, time to return-to-work at 12-month follow-up, no differences were found between the groups. There were also no differences found with the similar secondary outcome at 6-month follow-up. However, INT had a higher proportion in work (56.2%) compared with MHC (43.7%) and SAU (45.0%) (MHC vs INT: OR 0.59, p=0.012, 98.3% CI 0.36 to 0.98; SAU vs INT: OR 0.64, p=0.0293, 98.3% CI 0.39 to 1.05); MHC did not differ from SAU. No differences were found for weeks in work. Post-hoc, we produced the graph on the right panel in figure 2 displaying proportion in stable work per group over time but conducted no further statistical tests for differences. All vocational outcome estimates are displayed in table 2, while a Kaplan-Meier curve displaying return-to-work is shown on the left in figure 2.
{kind=link}
{kind=link}
Vocational outcome graphs. Left: Kaplan-Meier curve of time to stable return-to-work. Right: proportion in stable work per week. INT, integrated intervention; MHC, mental healthcare; SAU, service as usual.
Vocational outcomes: group values and pairwise comparison
Self-report data outcomes
With regard to secondary self-report outcomes, we saw only two differences, with one only borderline statistically significant: INT and MHC showed lower perceived stress compared with SAU (SAU vs INT: difference 1.46, p=0.034, 98.3% CI −0.19 to 3.12; SAU vs MHC: difference 1.66, p=0.0147, 98.3% CI 0.03 to 3.3). Among the remaining explorative outcomes, both INT and MHC showed better illness-related self-efficacy (IPQ) compared with SAU. INT showed a tendency towards better work-related self-efficacy than did MHC (p=0.045), and with regard to client satisfaction INT was better than SAU (p<0.005), MHC was better than SAU (p<0.005), and INT tended to be better than MHC (p=0.045). All other outcomes at 6 months and all outcomes at 12 months showed no differences (see table 3).
Self-report data outcomes
Subgroup and sensitivity analyses
Subgroup analyses showed variations in vocational outcomes between the first and last half of the RCT. The proportion of participants in work at 12-month follow-up increased from 39% to 51% in SAU but decreased in INT from 66% to 47%. In MHC, it was consistent at 44%. The interactions between the interventions and time were statistically significant in the comparison of SAU versus INT (p=0.001) and of MHC versus INT (p=0.024). Diagnosis interacted with the intervention: in the depression subgroup, we observed no differences with regard to time to return-to-work, but in the anxiety subgroup SAU had faster return-to-work than did MHC at 12-month follow-up (HR 1.65, p=0.020, p=0.021 for interaction) and at 6-month follow-up (HR 1.89, p=0.009, p=0.041 for interaction). A detailed report on the subgroup analyses can be found in online supplemental file 5.
Supplemental material
The results of the sensitivity analyses did not give us reason to lower the level of confidence in our conclusions from the main analyses of vocational outcomes. However, with regard to self-report outcomes, due to a higher proportion of missing questionnaire data in the SAU group (24%) than in the INT (13%) and MHC (17%) groups, confidence was lowered slightly. All best-case/worst-case scenario sensitivity analyses are reported in online supplemental file 4.
Supplemental material
Harms
There were fewer than five psychiatric admissions in each group. The rates of having hospital-based psychiatric outpatient contacts were similar in all three groups (INT: 29, 14.1%; MHC: 21, 10.5%; SAU: 26, 12.8%). There were no psychiatric emergency room contacts, suicides or episodes of self-harm or suicide attempts.
Discussion
Main findings
This study aimed at testing the effects of different intervention compositions on the return-to-work process after sick leave due to anxiety and depression. We compared an intervention of integrated vocational rehabilitation and health mental care (INT) with service as usual and with improved mental healthcare. The effects were measured on vocational outcomes and health status. The results partially support our hypotheses: INT did not show consistently better results than the other groups across all outcome domains. However, compared with MHC, INT showed a higher proportion of individuals in work at 12 months and yielded better intervention satisfaction (a predefined exploratory measure), but no other differences were found in any other outcome. Compared with SAU, INT showed a higher proportion of individuals in work at 12 months and a slightly lower stress level, slightly better work and social functioning and personal self-efficacy, and much higher intervention satisfaction. Compared with SAU, MHC showed no different vocational outcomes but a slightly lower stress level and personal self-efficacy. INT was the only group not showing worse outcomes in any domain, compared with any of the two other groups.
Other studies
The Norwegian At Work and Coping (AWaC) study compared an integrated intervention with a usual care group.30 The intervention integrated job support with healthcare, consisting primarily of cognitive behavioural therapy (CBT). However, unlike ours, the CBT was focused on work situations; in our study, job support was inspired by the IPS approach. The AWaC study showed that integration increased the proportion in work at 12 months compared with usual care (44.2% vs 37.2%, difference 6.9%, p=0.015). The effect found in the AWaC study was somewhat smaller than the effect of INT compared with SAU in our study, and especially when compared with MHC. Participants were not all on sick leave at baseline; they could also be occupationally struggling and a positive outcome was maintained work. The findings showed an even larger effect for long-term benefit recipients (24% vs 12%, p<0.05); however, we did not have the power to replicate this finding in our subgroup of baseline unemployed participants, who we believe were similar (40% (INT) vs 31.1% (SAU), p=0.38). Some aspects of health had improved and some health-related problems had diminished through the interventions, although on different scales: Perceived Stress Scale in our study versus Hospital Anxiety and Depression Scale and EQ5DL in the other. The combined results indicate positive effects of the integrated interventions, perhaps even more pronounced among persons with a complicated occupational history. Their reported larger health benefit could be explained by their CBT being work-focused.
One other study, by Lammerts et al31, compared integration of healthcare with occupational rehabilitation with usual occupational healthcare without such integration. A similarity with our study was the use of participatory return-to-work intervention: planning round-table meetings and early intervention. Contrary to our study, benefit case-handling and vocational rehabilitation were not handled by the same professional (employment specialists) but by two different stakeholders. Across all vocational and health-related outcomes, they found no differences at all, in line with the findings of our study. The few effects on health-related outcomes in our study might be explained by the fact that healthcare in our study was best practice healthcare, being primarily conventional CBT, whereas their healthcare was of an occupational nature. Furthermore, the intervention in their study was standard vocational rehabilitation, with some elements of integration; in our study we tested a new kind of vocational rehabilitation integrated with mental healthcare.
Interpretation of findings
Our findings suggest that neither INT nor MHC hastened return-to-work or led to more weeks in work, but INT did help more people achieve return-to-work at 12 months, compared with both other groups. Possible explanations for the missing effects of INT on time to return-to-work could be that the interventions in INT were not delivered as protocolled: the participants were offered fewer meetings with employment consultants than had been planned and the workplace contact was not implemented satisfactorily, yet these two types of contact are essential according to the IPS approach. Furthermore, participants in the SAU group received a far higher quantity of vocational rehabilitation courses outside the IBBIS study, compared with the quantity in the INT group. Hence, even though we might have improved the quality of the interventions in INT compared with SAU by adding an integrative element, this might have been offset by the lower quantity of vocational rehabilitation services in the INT group. Moreover, the integration activities were not implemented with consistently high fidelity and the results could be due to programme failure, rather than theory failure.
Regarding healthcare in the SAU group, we expected that SAU would not imply sufficient treatment,32 33 and we expected insufficiency to hamper return-to-work potential. Nevertheless, 85% of the participants in the SAU group had received mental healthcare at 6-month follow-up. The mean number of treatment sessions in this group was 9.5, which we consider sufficient for the disorders in question. Hence, there might not have been much possibility of improving vocational outcomes through improving treatment. The lack of positive effects on return-to-work rates might also be due to lack of specific focus on work functioning in the IBBIS healthcare in the INT and MHC groups. The INT group showed higher proportion in work at 12 months compared with the MHC group, and we know from the process evaluation that care managers in MHC sometimes downplayed the importance of vocational goals.34 This dynamic may have been more pronounced in the MHC group due to mitigation of the same through the integration activities in the INT group.
Harms
We found no evidence of harm attributable to any of the three interventions.
Strengths and limitations
The strengths of this study include the preplanned sample size being reached, a priori registration of a detailed statistical analysis plan, systematic reporting of all outcomes and only minor protocol deviances, all exhaustively reported. The limitations include participants and intervention providers not being blinded, perhaps introducing expectation bias in either direction. Furthermore, fidelity reviews indicated moderate deviation from the protocol, creating doubt whether the results should be ascribed programme or theory failure.
Implications
The heterogeneity of the results indicates that the optimal time for returning to work might not necessarily be the shortest, since fastest return-to-work, at 6 months, was observed with SAU, although this was accompanied by a probability of this group to experience decreasing proportion in work at 12 months. This perhaps indicates a too rapid return-to-work initially. Further, MHC shows poorer work outcomes than does INT, while not showing compensatory lower levels of symptoms. Accordingly, further studies are needed to elicit which outcomes encompass an ideal return-to-work process.
Furthermore, since INT included both integration and a new vocational rehabilitation, the results cannot be ascribed to either; distinguishing the effects of these elements would require new studies. Furthermore, the generalisability of the results to different legal and cultural contexts is uncertain.
Conclusion
This study trialled an integrated intervention, integrating vocational rehabilitation and mental healthcare, by comparing it with service as usual, as well as with improved mental healthcare. The INT group showed better vocational outcomes in one secondary outcome—proportion in stable work at 12 months—but not in the primary, return-to-work rates at 12 months. Additionally, it yielded some minor health benefits, making INT overall slightly better than SAU. Although MHC showed no different vocational outcomes compared with SAU, it did show some minor health benefits, making it overall better. The results from the fidelity assessment and the intervention delivery indicate that the integration of services in IBBIS was not implemented as planned. On this background, the effects of the IBBIS interventions might be different if ideally implemented. Since no other study has investigated these specific interventions, replication is needed to determine stability.
Data availability statement
Data are available upon reasonable request.
Ethics statements
Patient consent for publication
Ethics approval
The regional medical ethics committee deemed formal approval of the project unnecessary, and subsequently it did not undergo ethical scrutiny external to the research group.
Acknowledgments
We thank the participants for participating in the trial. We thank the clinical and trials staff for their indispensable help in conducting the trial. We thank all the jobcentre staff in the partaking municipalities for recruiting the participants. We thank Bea Ebersbach, Lisa Poulsen and Sara Mundy Skriver for their essential help in administering the economy and collection of self-report data, and Siv Bogevik Bjørkedal for crucial support in preparing and administering submission of the manuscript. We thank the Danish Agency for Labour Market and Recruitment and the collaborating municipalities for their financial and resource contributions, without which the trial could never have been conducted.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Twitter @andreashoffdk
Contributors AH: guarantor, data curation, formal analysis, investigation, methodology, software, supervision, validation, visualisation, writing - original draft, writing - review and editing. JF: data curation, formal analysis, investigation, methodology, software, validation, writing - review and editing. RMP: conceptualisation, data curation, funding acquisition, investigation, methodology, project administration, resources, validation, writing - review and editing. CH: formal analysis, methodology, supervision, validation, writing - review and editing. NR: project administration, resources, supervision, writing - review and editing. MM: supervision, validation, writing - review and editing. ABB: data curation, formal analysis, methodology, software, validation, visualisation, writing - review and editing. LFE: conceptualisation, funding acquisition, investigation, methodology, project administration, resources, supervision, validation, writing - review and editing.
Funding The study was funded by the Danish Agency for Labour Market and Recruitment with 38.102.321 DKK and by contributions from the collaborating Danish municipalities that delivered the vocational rehabilitation interventions. None of these funding organisations had any influence on the interpretation of the results, or on the writing or review of the manuscript. Further, no funding organisation saw the manuscript before submission. The collaborators contributed to developing the study protocol, which included population definition and determining the outcomes.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.