Article Text

Abstract
Objectives To examine age at diagnosis, prognostic factors and survival of prostate cancer (PCa) in Norwegian firefighters and three other occupations undergoing occupational health check-ups, and comparing with PCa cases in the general population.
Methods All PCa cases diagnosed in 1960–2017 were extracted from the Cancer Registry of Norway. Firefighters, military employees, pilots and police officers were identified through occupational data from Statistics Norway. Age at diagnosis, clinical stage, prostate-specific antigen (PSA), Gleason score, performance status and overall survival and PCa-specific survival in cases in these occupations were compared with cases in the general population.
Results Firefighters were significantly younger at PCa diagnosis than cases in the general population in 1960–1993 (mean difference: 2.1 years) and 2007–2017 (mean difference: 4.3 years). At diagnosis, firefighters had significantly lower PSA values, Gleason scores and performance status scores than the general population. Firefighters diagnosed in 2007–2017 had lower risk of all-cause death than the general population (crude HR 0.71 (0.53–0.95)). No difference remained after adjusting for age at diagnosis (HR 1.03 (0.77–1.37)). Firefighters were older at diagnosis in 1994–2006 (mean difference: 3.0 years), but showed no other significant differences in age at diagnosis, PSA values, Gleason scores or performance status compared with military employees, pilots and police officers.
Conclusions Younger age and better prognostic factors at PCa diagnosis among firefighters and other occupations with requirements for health check-ups than cases in the general population may indicate an increased diagnostic intensity, likely contributing to elevated PCa incidence in such occupations.
- firefighters
- military personnel
- occupational health services
- medical oncology
- urogenital system
Data availability statement
Data may be obtained from a third party and are not publicly available.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Key messages
What is already known about this subject?
Firefighters have been shown in meta-analyses to have increased incidence of prostate cancer (PCa) compared with the general population. Firefighters are exposed to many occupational carcinogens, but no chemical agent is considered an established risk factor for PCa. Increased diagnostic intensity through regular health check-ups has been suggested as an explanation for increased PCa risk among firefighters.
What are the new findings?
Norwegian firefighters were younger and had better prognostic markers at PCa diagnosis than the general population, leading to better crude overall survival, although no survival benefit remained after adjusting for age at diagnosis. Other occupations with regular health check-ups (military employees, pilots and police officers) showed similar results.
How might this impact on policy or clinical practice in the foreseeable future?
The benefits of early PCa diagnosis should be weighed against the potential of overdiagnosis and overtreatment in occupations with requirements for health check-ups when guidelines or regulations for such check-ups are made.
Introduction
Meta-analyses of studies of cancer risk in firefighters have found increased SIRs of prostate cancer (PCa), but not elevated SMRs.1–4 Through their occupation, firefighters are exposed to a wide variety of known and suspected carcinogens,1 including monocyclic and polycyclic aromatic hydrocarbons and halogenated organic compounds, some of which have been associated with PCa.5–7 However, no chemical agent is considered as an established risk factor for PCa.
The introduction of the prostate-specific antigen (PSA) test in the late 1980s profoundly changed the diagnosis of PCa, mainly by increasing the possibility of finding low-stage and low-grade tumours.8–10 Studies of PCa aetiology are complicated by the fact that geographic, socioeconomic and/or temporal differences in diagnostic intensity (including rate of PSA-testing) influence incidence measures of PCa.9 10 Firefighters are usually subject to mandatory occupational health check-ups, potentially leading to increased diagnostic intensity of PCa compared with the general population. This is a proposed explanation for the observed elevated incidence of PCa in firefighters.3 11 For Norwegian firefighters, national guidelines for health check-ups were formalised in 1994.12
The aim of this study is to examine age and prognostic factors at diagnosis of PCa and survival after diagnosis in Norwegian firefighters, comparing with cases in the general Norwegian population. If regular occupational health check-ups affect PCa diagnosis, we would expect firefighters to be diagnosed at a younger age and have better prognostic factors at diagnosis than cases in the general population, potentially leading to improved survival after diagnosis. Military employees, pilots and police officers are other workers shown to have increased SIRs of PCa.3 13–16 These workers, like firefighters, usually have requirements for health check-ups. Although possibly exposed to occupational carcinogens, their exposure is not likely to resemble the amount or variety of carcinogens encountered by firefighters. Thus, these occupations represent a valuable reference group when examining firefighters, with a shared possible increased diagnostic intensity than the general population through occupational health check-ups, but minimal exposure to carcinogens encountered in firefighting. These three occupations are therefore included for comparisons in this study.
Methods
We extracted all cases of PCa from the Cancer Registry of Norway (CRN) diagnosed 1 January 1960 through 31 December 2017. The following variables were available for all cases: date of diagnosis, age at diagnosis, morphology and vital status (alive, deceased or emigrated per 31 December 2018). Emigration date was available for all emigrated, and date and cause of death were available for all deceased. In addition, region of residence at the time of diagnosis was available for virtually all cases (>99.9%), and >90% of cases had information on the clinical stage of disease. As the frequency of diagnosis of PCa is heavily influenced by the PSA test,8 we divided year of diagnosis into the following three periods: 1960–1993, 1994–2006 and 2007–2017, representing the pre-PSA, early-PSA and late-PSA eras in Norway, respectively. The cut-offs at 1993/1994 and 2006/2007 account for additional possible changes in diagnostic intensity for Norwegian firefighters. In 1994, national guidelines for smoke divers were implemented, including guidelines for health check-ups,12 while in 2007, the International Agency for Research on Cancer (IARC) classified work as a firefighter as possibly carcinogenic,1 potentially increasing the awareness among firefighters of an elevated cancer risk.
From the National Prostate Cancer Registry, the following information was available for cases diagnosed in 2004 or later: PSA value, Gleason score, Tumor/Node/Metastasis (TNM) staging, and WHO performance status (also known as the Eastern Cooperative Oncology Group score17). PSA values were categorised as <5, 5–9.9, 10–19.9 or >20; Gleason scores as <7, 7 (3+4), 7 (4+3), 8 or >8 and WHO performance status scores as 0–1 (ability of regular activities of daily living) or >1 (reduced ability of daily life functioning).
Clinical stage of disease is classified as local (cancer confined to the prostate), regional (metastasis to regional lymph nodes or tumours extending through the prostatic capsule) or distant disease (metastasis to non-regional lymph nodes or other organs). For cases with registered TNM stage, but missing clinical stage of disease, we defined local disease as T1–T2, N0, M0; regional disease as T3–T4 and/or N1, M0; and distant disease as any T, any N, M1. Cases with ‘Metastasis present, but unknown location’ were classified as distant disease.
Employment data for all cases were collected by linkage to Statistics Norway using Norwegian residents’ unique personal identification numbers. Occupation was extracted from complete national censuses conducted in 1960, 1970 and 1980, a partial national census in 1990, and yearly employment registrations from 2004 through 2018. Occupational codes in the censuses and later registrations were based on Norwegian adaptations of the International Standard Classification of Occupations.18–20 The occupational codes were used to identify cases that had worked as firefighters, military personnel, pilots or police officers. We defined the general population as men not registered with any of these four occupations before PCa diagnosis. In this article, we refer to the group of military employees, pilots and police officers combined as ‘the reference occupations’. Statistics Norway also provided information on marital status (unmarried, married or widower/divorced/separated) at the time of diagnosis for all cases.
Study sample
The CRN contained 137 536 cases of PCa diagnosed from 1 January 1960 through 31 December 2017. We excluded 11 cases with age at diagnosis <20 years, as they lacked the opportunity to enter an occupation before diagnosis; 34 recurrent cancers erroneously registered as new cases; 6452 cases with no registered occupation at any census and age >40 years in 1960, as these were regarded likely to have had an occupation undeterminable to us before the earliest available census and 12 685 cases with unspecified morphology or morphology other than adenocarcinoma.
We checked the date of diagnosis for all cases among firefighters and the reference occupations to ensure they had been working in the occupation in question prior to PCa diagnosis. If diagnosis occurred before the earliest registration of the occupation, that case was moved to the general population (20 cases). Prior to 2015, only one occupation was recorded per person per year. From 2015 through 2018, all occupations held per year were registered. Cases registered with ≥2 years in one of the selected occupations between 2015 and 2018 were considered likely to have been working part-time in the given occupation before 2015, and were therefore assigned that occupation for earlier years (occurred only for firefighters, 37 cases). Cases registered as having worked both as a firefighter and one or more of the reference occupations were included only in the occupation held last before PCa diagnosis (30 cases).
The final study sample comprised 118 354 men with PCa: 487 firefighters, 4734 in the reference occupations (3776 military employees, 183 pilots and 775 police officers) and 113 133 men in the general population.
Statistical analysis
Mean age at diagnosis with 95% CI was calculated for each group. Likewise, we calculated proportions with 95% CIs for the categories of clinical stage of disease, PSA values, Gleason score and WHO performance status. We performed regression analyses to investigate whether there were statistical interactions between occupation and period of diagnosis for the variables age at diagnosis (linear regression) and clinical stage of disease (ordinal logistic regression). As we found significant interaction in both analyses (p<0.001), we present results stratified by period of diagnosis. We performed χ2tests to compare clinical stage (for each period of diagnosis), PSA, Gleason and WHO performance status in firefighters with the general population and the reference occupations.
To illustrate how age at diagnosis of PCa has changed over time, we derived 1-year averages in each group. Locally weighted smoothing (bandwidth 0.8) was used to create a graph based on these data.
We made Kaplan-Meier curves of overall survival and cumulative mortality curves of PCa-specific death for each group, by period of diagnosis.
Cox regression, with time since diagnosis as time variable, was used to estimate HRs with 95% CIs for the association between group and risk of death from all causes and risk of death from PCa. We censored for emigration in all analyses and for death of other causes in the analysis of death from PCa (standard competing risk framework in Cox regression). End of follow-up was 31 December 2018.
Although possibly influencing PCa diagnosis and/or risk of death, region of residence and marital status were not considered to be confounders as we deemed these variables unlikely to affect whether one entered one of the four occupations. Thus, in our main analyses, we did not include any covariates. However, to illustrate the contribution from early diagnosis, we present results from Cox regression analyses adjusted for age at diagnosis.
A significance level of 5% was used. All analyses were performed using Stata V.16.1 (Stata Corp, College Station, TX, USA).
Ethics
The Regional Committees for Medical and Health Research Ethics approved the study and considered it exempt from needing informed consent from the participants (ref. 2019/542).
Results
Mean age at diagnosis was lower in firefighters and the reference occupations than in the general population (table 1). A higher proportion of cases in both groups was diagnosed in 2007–2017 compared with the general population.
Characteristics of prostate cancer cases diagnosed in Norway 1960–2017
Firefighters were significantly younger at diagnosis compared with the general population for cases diagnosed in 1960–1993 and 2007–2017 (mean difference (95% CI) 2.1 (0.3 to 3.8) and 4.3 (3.2 to 5.3) years, respectively), but not 1994–2006 (1.1 (–0.4 to 2.6)) (table 2). In cases diagnosed during 1994–2006, firefighters were significantly older at diagnosis than the reference occupations (−3.0 (–5.0 to –0.8)). A smoothed curve of average age at diagnosis each year for firefighters, the reference occupations and the general population illustrate these changing trends (online supplemental figure S1).
Supplemental material
{kind=link}
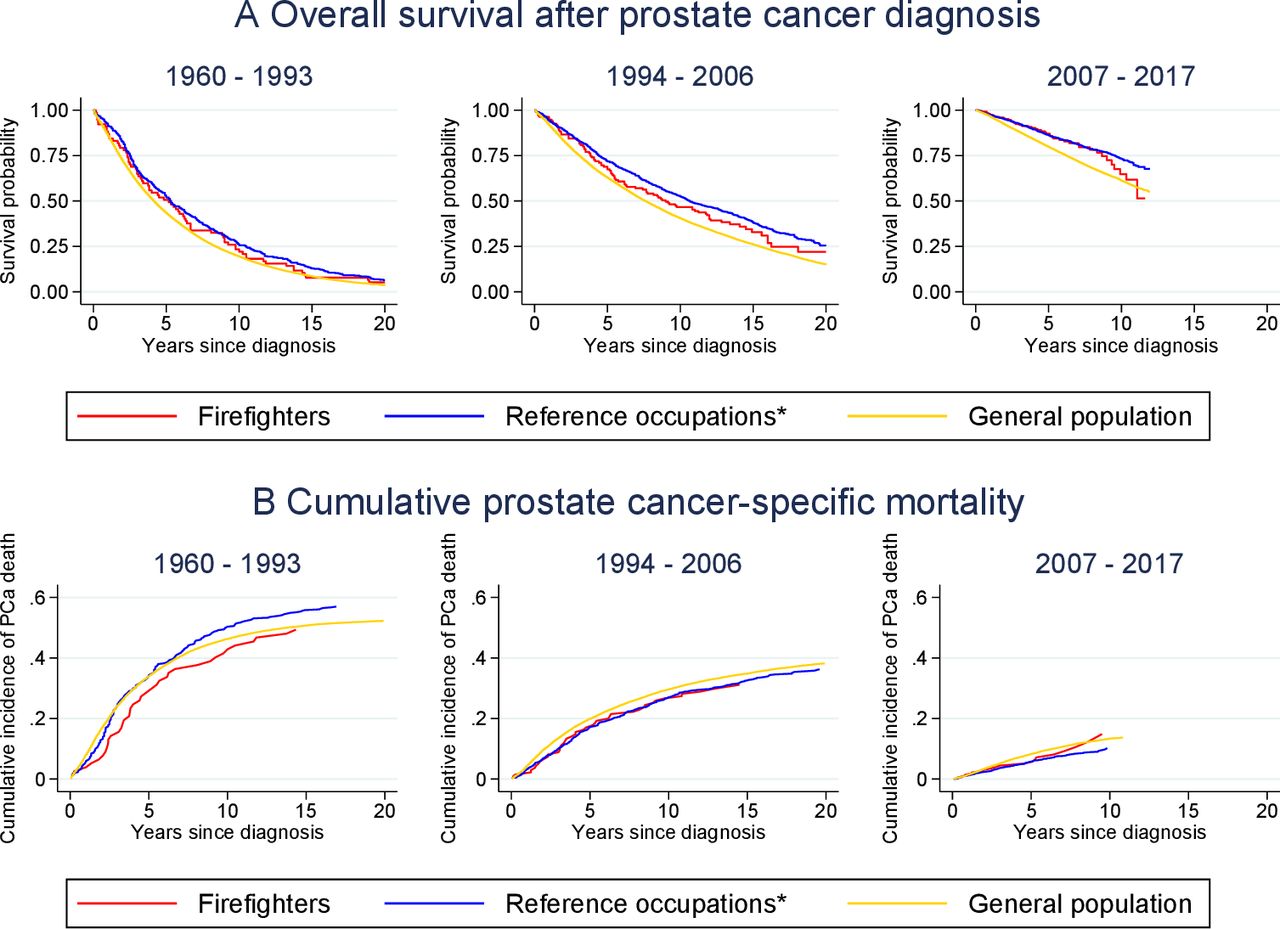
(A) Kaplan-Meier curves of overall survival after PCa diagnosis in Norway, by period of diagnosis. (B) Cumulative mortality curves of PCa-specific deaths in Norway, by period of diagnosis. PCa cases diagnosed in Norway during 1960–2017, n=118 354 men. End of follow-up is 31 December 2018. *Military employees, pilots and police officers. PCa, prostate cancer.
Mean age (95% CI) at diagnosis of prostate cancer in Norway during 1960–2017, by period of diagnosis
For cases diagnosed in 1960–1993, firefighters showed little difference in clinical stage of disease compared with the general population (p=0.70; table 3). However, firefighters had better clinical stage than the general population for cases diagnosed in 1994–2006 and 2007–2017 (p=0.08 and 0.04, respectively). Firefighters also had significantly more favourable PSA levels (p<0.001) and Gleason scores (p=0.01), and better WHO performance status scores (p<0.002). No significant differences were found for any of these factors when comparing firefighters with the reference occupations.
Prognostic factors at diagnosis of prostate cancer in Norway in 1960–2017, by period of diagnosis
The Kaplan-Meier curves show better survival for PCa cases in firefighters and the reference occupations in all periods of diagnosis compared with cases in the general population (figure 1A). Crude risk of death from all causes was significantly lower in firefighters than in the general population for cases diagnosed in 2007–2017 (HR 0.71, 95% CI (0.53 to 0.95)), but not significantly lower in 1960–1993 (HR 0.93 (0.74 to 1.16)) or 1994–2006 (HR 0.83 (0.68 to 1.02)) (table 4). The reference occupations had a significantly lower crude risk of death after PCa diagnosis than the general population in all three periods of diagnosis. Adjusting for age at diagnosis generally reduced the differences between the two groups and the general population, and the significantly reduced risk of death in firefighters diagnosed in 2007–2017 was no longer present (HR 1.03 (0.77 to 1.37)).
HRs* and 95% CIs for risk of death from all causes and risk of death from PCa, by period of diagnosis for PCa cases diagnosed in Norway 1960–2017, crude and adjusted for age at diagnosis
Similar patterns were found for PCa-specific death (figure 1B, table 4), but risks of death (crude or adjusted for age at diagnosis) were not significantly lower in firefighters compared with the general population in any period.
Discussion
In this study of PCa in Norway during 1960–2017, firefighters were diagnosed with PCa at a younger age than men in the general population, most pronouncedly so for cases diagnosed during 2007–2017. PSA level, Gleason score and WHO performance status scores were available from 2004, and we found more favourable values for PCa cases in firefighters than for cases in the general population. Risk of death of all causes was significantly lower in firefighters than in the general population when diagnosed in 2007–2017. A reduced risk of death of PCa, though not statistically significant, was also found in this period in firefighters compared with the general population. These reduced risks of death were not present after adjusting for age at diagnosis. Firefighters were older at diagnosis in 1994–2006, but we found no other differences between firefighters and the reference occupations in age at diagnosis or prognostic factors. Patterns in risk of death, both overall and PCa-specific, were also comparable between firefighters and the reference occupations.
Based on Nordic occupational codes from census data in 1960, 1970 and 1980, Pukkala et al 21 investigated the incidence of PCa among firefighters with follow-up through 2003, 2004 or 2005 depending on country. They observed a non-significantly increased SIR in Norwegian firefighters (1.16, 95% CI 0.97 to 1.37) compared with the Norwegian general population. For Nordic firefighters overall, there were significantly increased SIRs in ages 30–49 years (SIR 2.59) and 50–59 years (SIR 1.16) throughout the whole observation period, and for all ages combined in the later part of the follow-up (1991–2005; SIR 1.15). A study in American firefighters (follow-up 1985–2009) found an elevated PCa incidence in firefighters aged <65 years (SIR 1.21), but not in firefighters aged ≥65 years (SIR 0.96).22 A recent meta-analysis of international data reported increasingly higher SIRs of PCa for firefighters first employed during <1950, 1950–1970 or >1970 respectively, with significantly elevated values for the two latter categories compared with the general population.11 Our study is not designed to investigate incidence rates, and thus the SIRs cannot be directly compared with our results. Nonetheless, we also find a lower age at diagnosis among firefighters and a higher proportion of cases diagnosed in the later periods compared with the general population. These findings suggest that firefighters still in working age are more likely to be diagnosed with PCa than other men their age, possibly because of increased diagnostic intensity through occupational health check-ups, and that the introduction of the PSA-test three decades ago has enhanced this susceptibility.
A lower age at diagnosis was also observed for firefighters and the reference occupations in the pre-PSA era. Though Norwegian national guidelines for health check-ups in firefighters did not exist before 1994, most large fire departments had routines for health check-ups going back to the 1950s (unpublished material gathered for23). Increased diagnostic intensity through regular health check-ups could have been, and can still be, mediated in other ways than through higher rates of PSA-testing. Men may be more inclined to report or be asked about lower urinary tract symptoms when required to talk to a physician regularly. A digital rectal examination may also have been a part of a physical examination in lieu of PSA-testing.
Three recent meta-analyses found non-significantly increased PCa mortality among firefighters compared with the general population.3 4 11 We have found no studies comparing case fatality rates between firefighters and the general population. Our results showed lower risk of death among firefighters with PCa compared with cases of PCa in the general population, that is, a lower case fatality rate. This does not necessarily mean that the PCa SMR would be lower in Norwegian firefighters. If the incidence of PCa is higher in Norwegian firefighters than the general population, the SMR could still be increased even though the case fatality rate is lower.
We found no studies presenting other prognostic factors than age at diagnosis when reporting on PCa among firefighters, military employees, pilots or police officers. However, our results are comparable to those reported in studies of men attending PCa screening programmes.24
Our findings suggest that increased diagnostic intensity of PCa in Norwegian firefighters compared with the general population leads to diagnosis at a younger age, with better prognostic markers and improved crude overall survival. In particular, the classification by the IARC in 2007 of firefighting as possibly carcinogenic may have led to increased attention to PCa risk, which may explain the observed lower mean age at diagnosis and better crude overall survival among firefighters for cases diagnosed in 2007–2017 compared with 1994–2006.
By looking at the Kaplan-Meier curves (figure 1A), the benefit of survival after PCa diagnosis for firefighters compared with the general population seem to be equal to the difference in age at diagnosis. This relationship between age at diagnosis and difference in length of overall survival seems to hold true for all three periods. When adjusting for age at diagnosis in the Cox regression analyses, risk of death for firefighters diagnosed 2007–2017 was no longer significantly lower than in the general population. This raises the possibility that our observed better survival among firefighters is related to a lead-time bias. Similar findings were seen when comparing the reference occupations with the general population.
Even though our findings suggest that diagnostic intensity may affect the diagnosis of PCa in firefighters and the reference occupations, our study does not allow us to say whether increased diagnostic intensity fully explains the increased incidence of PCa observed in these occupations. Higher diagnostic intensity is likely to increase the observed incidence of PCa, but we cannot exclude the possibility that occupational exposures, either common to the four occupations or specific for any of them, also contribute to increased incidence.
An important strength of our study is the large amount of data on occupation and disease gathered from high-quality and independent national sources. We obtained information on all PCa cases registered in Norway in 1960–2017, including detailed clinical information from the National Clinical Registry of Prostate Cancer from 2004 onwards. Statistics Norway provided data on occupation for all cases. The Norwegian Cause of Death Registry provides the CRN with information about date and cause of death for all deceased cancer cases. We therefore regard the data in our study to encompass virtually all relevant available data on Norwegian PCa cases.
Our study has some limitations. Employment records were not registered annually by Statistics Norway until 2004. Earlier occupational data are based on censuses carried out in 1960, 1970, 1980 and a partial census in 1990. In addition to the 10-year gaps between the earlier censuses, there is a potential 24-year gap between 1980 and 2004. Any person with PCa with the occupation of firefighter, military employee, pilot or police officer within these gaps, but not in the census years, will not have been identified as having had the occupation in question. Additionally, Norwegian firefighters are often employed in part-time positions, especially in rural areas. From 2015, all positions are registered in the employment records, but before this, only the highest percentage position was registered. Thus, we may have been unable to identify some men with the occupation of firefighter (full-time or part-time), military employee, pilot or police officer. We would expect this misclassification, if anything, to decrease the difference between the four occupations and the rest of the population. We identified no confounders among the available variables, but cannot exclude the presence of unmeasured confounders, such as family socioeconomic status. Finally, we have no individual data on whether cases attended occupational health check-ups and if so, whether the PCa diagnosis was suspected or confirmed through such check-ups.
Guidelines for occupational health check-ups and baseline diagnostic intensity of the general population may differ between countries and over time, and such geographic and temporal variations should be considered before generalising our findings. With increased diagnostic intensity (eg, more PSA-testing) in the general population, or less stringent regulations for occupational health check-ups, we would expect more similar age at diagnosis, prognostic factors and survival of PCa in firefighters or other occupations with health check-ups compared with the general population.
The influence from diagnostic intensity, particularly PSA-testing, complicates aetiological research on PCa. In future studies of PCa in firefighters or other occupations with requirements for health check-ups, researchers should consider differentiating aggressive and indolent PCa cases, for instance, by clinical stage or cases leading to fatal disease. In this way, researchers may filter out low-risk cases possibly caused by high diagnostic intensity rather than occupational carcinogen exposure. Furthermore, a cut-off at retirement age as used by Daniels et al 22 would help differentiate cases diagnosed in working age, and thus still exposed to regular occupational health check-ups, from those diagnosed after retirement. Firefighters and physicians performing occupational health check-ups should be aware that increased attention to PCa risk may lead to higher diagnostic intensity, and possibly overdiagnosis and/or overtreatment.
Conclusion
Norwegian firefighters were younger at PCa diagnosis than the general population, and also had lower PSA levels and Gleason scores at diagnosis. Age at diagnosis and prognostic factors in firefighters were similar to the reference occupations. These findings would be expected in the presence of an increased diagnostic intensity, which thus seems likely to contribute to elevated PCa incidence among firefighters. Improvements in crude overall survival in the four occupations compared with the general population seemed similar to the lead time of diagnosis, and a lowered overall risk of death in firefighters diagnosed in 2007–2017 compared with the general population was not evident after adjusting for age at diagnosis. This suggests that requirements for occupational health check-ups can affect the timing of PCa diagnosis, but it is uncertain if earlier diagnosis has a positive effect on overall survival besides contributing lead time.
Data availability statement
Data may be obtained from a third party and are not publicly available.
Ethics statements
Patient consent for publication
Acknowledgments
We thank Tor Åge Myklebust, Jan Ivar Martinsen and Nathalie Støer for help with statistical analyses. We also thank Leif Aage Strand, Anthony Wagstaff and Bjørn Aage Granhus for input regarding guidelines and practices for health check-ups of Norwegian military employees, pilots and police officers, respectively.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Twitter @MaritBVeierod
Contributors JJ managed the data, carried out statistical analyses and drafted the paper. TKG and KK originally planned the study. MBV provided guidance for the statistical analyses. TKG, MBV SDF, BH and KK all contributed to the design of the study and revised the drafted paper.
Funding The first author’s research position, and thus this article, is funded by a grant from the Dam Foundation (grant number 2019/FO247424).
Competing interests JJ, TKG and KK are part of a research project at the Cancer Registry in Norway on cancer in Norwegian firefighters. The project has received funding from the following organisations: Gjensidige Foundation, the Norwegian Union of Municipal and General Employees, the Norwegian Confederation of Trade Unions, the Norwegian Cancer Society, Oslo Brannkorpsforening, Norwegian Firefighters Fight Cancer and the Norwegian Labour Inspection Authority. However, the funding has not covered the present article, and none of the mentioned organisations has had any part in the design, analysis or writing of the present article.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.