Article Text

Abstract
Objectives Although healthcare workers (HCWs) have been particularly affected by SARS-CoV-2, detailed data remain scarce. In this study, we investigated infection rates, clinical characteristics, occupational exposure and household transmission among all symptomatic HCWs screened by SARS-CoV-2 RT-PCR between 17 March (French lockdown) and 20 April.
Methods SARS-CoV-2 RT-PCR was proposed to symptomatic (new cough or dyspnoea) HCWs at Creteil Hospital in one of the Parisian suburbs most severely affected by COVID-19. Data on occupational profile, living situation and household, together with self–isolation and mask use at home were collected, as well as the number of cases in the household.
Results The incidence rate of symptomatic SARS-CoV-2 was estimated to be 5% (110/2188). A total of 110 (35%) of the 314 HCWs tested positive and 9 (8%) were hospitalised. On multivariate analysis, factors independently associated with positive RT-PCR were occupational profile with direct patient facing (OR 3.1, 95% CI 1.1 to 8.8), p<0.03), and presence of anosmia (OR 5.7, 95% CI 3.1 to 10.6), p<0.0001). Being a current smoker was associated with negative RT-PCR (OR 0.3, 95% CI 0.1 to 0.7), p=0.005). Transmission from HCWs to household members was reported in 9 (14%) cases, and 2 deaths occurred. Overall, self-isolation was possible in 52% of cases, but only 31% of HCWs were able to wear a mask at home.
Conclusion This is the first study to report infection rates among HCWs during the peak of the SARS-CoV-2 epidemic in France and the lockdown period, highlighting the risk related to occupational profile and household transmission.
- hygiene / occupational hygiene
- virology
- health care workers
- viruses
Data availability statement
Data are available upon reasonable request (pascal.andujar@chicreteil.fr or evguenia.krastinova@chicreteil.fr).
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Summary box
W)hat is already known about this subject?
Although healthcare workers (HCWs) have been particularly affected by SARS-CoV-2, no data are available concerning household transmission and the risk of SARS-CoV-2 infection related to their occupational exposure profile (direct or indirect patient facing).
What are the new findings?
To our knowledge, this is the first study conducted during the lockdown period of the epidemic peak in France to report a higher SARS-CoV-2 infection rate among symptomatic HCWs with direct patient facing compared with indirectly exposed HCWs, together with a high risk of household transmission.
How might this impact on policy or clinical practice in the foreseeable future?
Our results should have a real impact on public health and occupational health policies designed to ensure better preparation for another epidemic wave, essentially stock management of appropriate individual and collective protective equipment and efficient contact tracing with, if necessary, home isolation or rehousing to avoid the risk of household transmission.
Introduction
The SARS-CoV-2 epidemic is the worst worldwide pandemic in the last five decades, with more than 40.5 million cases and 1119 283 deaths as of 18 October 2020.1 2 Europe has paid a heavy burden, as 23% (256 540) of all deaths have been registered in Europe1 2 and France is among the 10 countries most severely affected by the pandemic with more than 910 277 cases reported as of 20 October, and 33 623 deaths.3 Collection of data concerning healthcare workers (HCWs) contaminations in France started in May 2020 and a total of 36 266 COVID-19 cases have been reported across 18 French regions since 1 March 2020, including 29 610 (82%) HCWs and 3777 (10%) non-caregivers.4
HCWs have been particularly affected by SARS-CoV-2 all over the world, but data remain scarce with considerable variability, illustrating the complexity of collecting complete data in any country. In February 2020, China reported more than 3300 HCWs with SARS-CoV-2,5 which represented 2.7% of all exposed HCWs. Another review of the literature estimated the incidence in HCWs to be between 1.9% and 29.4%.6 Italy also reported high infection rates among HCWs, as 10% of all COVID-19 cases occurred in HCWs, and 80 doctors and 25 nurses died.7 8 The US Centers for Disease Control and Prevention reported 9282 COVID-19 cases in USA between February and 9 April and stressed that this number was largely underestimated, as 84% of patients had missing data concerning possible HCW status.9 From 27 February to 31 August 2020 in Mexico City’s public database, 16 446 (13.1%) of cases concerned HCWs (28% physicians, 38% nurses and 34% other HCWs) and 321 (1.9%) of them died.10
Few data are available concerning HCW-to-household transmission. We found only one study that pooled data for HCWs and household members. Among 30 individuals sharing a household with a virus-confirmed case of COVID-19, 80% were seropositive.11 This is an extremely high transmission rate, suggesting that members of HCW households actually incurred even greater collateral damage. However, the chronology of transmission and the environmental context (lockdown or no lockdown) were not detailed in this study.
The COVID-19 pandemic has resulted in a surge of patients exceeding available human and physical resources in many settings, triggering the implementation of crisis standards of care. Unpreparedness, lack of resources (masks and anaesthetic supplies) made the crisis difficult to manage for HCWs. In addition, some authors have hypothesised that high stress levels due to long working hours with a high emotional load could make HCWs abnormally susceptible to infection.12
Furthermore, France was unprepared and inexperienced to face the burden of the epidemic, especially during the early phases, leading to the need for a general lockdown that was implemented on 17 March in order to contain the epidemic. The peak of the epidemic in France occurred between 31 March and 3 April. The north-eastern region of France and the greater Paris area were severely hit by the epidemic.13 Lockdown modalities differed from country to country. In metropolitan France, lockdown consisted of banning all outdoor activities, for example, schools were closed, meetings, museums, public transport were very limited, except with a special waiver, such as HCWs.
Few studies have detailed the clinical characteristics and risk factors of HCWs with coronavirus disease,9 14 with high missing data rates.9 At the beginning of the epidemic, lack of awareness, training and shortages probably contributed to viral spread.15 According to the study by Burrer et al,9 various factors interacted and probably contributed to infection in HCW patients, such as: reported contact with patients with COVID-19 in healthcare, household and community settings.
In this study, we investigated symptomatic infection rates, clinical characteristics, occupational exposure, living conditions and household transmission of symptomatic HCWs screened by SARS-CoV-2 RT-PCR between 17 March (date of French lockdown) and 20 April.
Patients and methods
Screening was proposed to all HCWs with SARS-CoV-2 symptoms, defined as the presence of fever and/or respiratory symptoms (new cough or dyspnoea) between 17 March and 20 April at Creteil Hospital (Centre Hospitalier Intercommunal de Créteil). Three groups were defined in order to investigate the occupational profile of HCW: (1) Directly patient facing (eg, nurses, doctors, allied health professionals, porters, etc), (2) Non-patient facing but potentially at higher risk of nosocomial exposure (eg, domestic and laboratory staff), and (3) Non-clinical (eg, clerical, administrative, information technology, secretarial, etc). Screening was not mandatory, but was highly recommended for symptomatic HCWs. Non-opposition consent was obtained from all participants.
Nasopharyngeal (NP) specimens were obtained by using the eSwab collection system (COPAN, Brescia, Italy). SARS-CoV-2 reverse transcription (RT)-PCR was performed on the automated Seegene STARlet system, according to the manufacturer’s instructions using the CE marked Allplex 2019-nCoV RT-PCR assay (Seegene, South Korea) which targets N-gene (viral nucleocapsid protein) and RdRP-gene (RNA-dependent RNApolymerase), both SARS-CoV-2-specific genes, and the sarbecovirus specific E-gene (viral envelope).
Temperature, blood pressure and O2 saturation were recorded by a trained nurse, who also performed the NP swab. Clinical interview and, when necessary, physical examination, were performed by the physician. Occupational profile was recorded together with the date of onset of symptoms, smoking status, height, weight, treatments, clinical symptoms at illness onset and the day of screening. Pre-existing risk factors and chronic medical conditions defined as: age >65 years, chronic kidney disease on dialysis, NYHA (New York Heart Association (NYHA) Functional Classification) classes III or IV heart failure, cirrhosis, complicated insulin-dependent diabetes, chronic respiratory disease at risk of decompensation, asthma, immunosuppression (immunosuppressive treatment, cancer, haematological malignancies, transplant,<200 CD4), obesity defined by body mass index (BMI) ≥30) were gathered by the physician.
If necessary, a complete physical examination, including respiratory examination, was performed. All consultants were given 24 hours sick leave and written advice about self-isolation and hygiene. Results were provided by phone by a physician in less than 24 hours and a short clinical evaluation was performed, comprising respiratory rate, temperature and the presence of clinical symptoms. All patients with positive SARS-CoV-2 RT-PCR were also followed by phone at Day(D)5, D7, D10 and D14 after illness onset using the same survey. Data on living situation (apartment or house, number of rooms and square metres) and household (other people sharing the same home) together with self-isolation and mask use at home were collected. The presence of SARS-CoV-2-positive members in the household and the date of symptom onset were also recorded. As the median incubation period is 5.2 days (95% CI 4.1 to 7.0), potential HCW-to-household transmission was considered when the time interval between symptom onset was ≥7 days.16 Thus, transmission was considered true only if a household member developed COVID-related symptoms ≥7 days after the HCW sharing the same house and testing positive for COVID-19. Details concerning occupational profile, health restrictions and telecommuting during the study period were recorded for a total of 2588 people working at Creteil hospital.
Statistical analysis
Baseline characteristics were compared with χ2 test or Student’s t-test, as appropriate. Multivariate analysis was performed with a logistic regression model. Variables were included in the multivariate analysis when a value of p≤0.2 was observed in the bivariate analysis. Based on predictors identified in bivariate and multivariate analyses, we also constructed receiver operating characteristic (ROC) curves and calculated the corresponding area under the curve (AUC). Values of p<0.05 were considered to denote statistically significant differences. All analyses were performed with Stata V.14 software.
Results
A total of 2588 people usually work at Creteil hospital (1352 in group 1; 603 in group 2 and 233 in group 3). During the study period, 151 were telecommuting and 249 (10%) were identified with risk factors for COVID-19 and were sent home. Finally, a total of 2188 people were working and present in the hospital. The overall observed incidence rate of symptomatic SARS-CoV-2 infection was 5.0% (110/2188); 6.4% (87/1352) in group 1; 2% (12/603) in group 2; and 3% (7/233) in group 3. No significant difference was observed between groups 2 and 3, but these two groups were significantly different from group 1 (p<0.0001 and 0.01, respectively). A total of 110 (35%) of the 314 symptomatic HCWs tested between 17 March and 20 April, 2020 were found to be SARS-CoV-2-positive; 9 (8%) of them were hospitalised and 2 were admitted to the intensive care unit. No deaths occurred among SARS-CoV-2-positive HCWs. During the same period, 371 patients were hospitalised for COVID-19 in the hospital and 61 of them died. High participation and response rates were observed, as all participants completed the survey. After systematic screening of the reasons for time off work by the occupational medicine unit, only 11 HCWs tested outside the hospital (n=11/110; 10%) were identified. Each participant also completed the survey and follow-up.
Nine (8%) HCWs with positive SARS-CoV-2 RT-PCR were hospitalised, including eight HCWs directly facing patients (eg, doctors, nurses and allied health professionals) and one working as a cleaner (classified in group 2). Hospitalised SARS-CoV-2-positive patients were more frequently older than 50 years than non-hospitalised patients (56% vs 18%, p=0.01). Fifty-six per cent had a BMI ≥30 vs 30% of non-hospitalised patients, p=0.1. The sex ratio was five women to four men. Five of the hospitalised HCWs had hypertension, two had diabetes and one had asthma. The mean length of hospital stay was 15 days (range: 3 days to 24 days). Two HCWs were discharged, then readmitted to the ICU following deterioration (one had bilateral pulmonary embolism and one had acute respiratory distress syndrome).
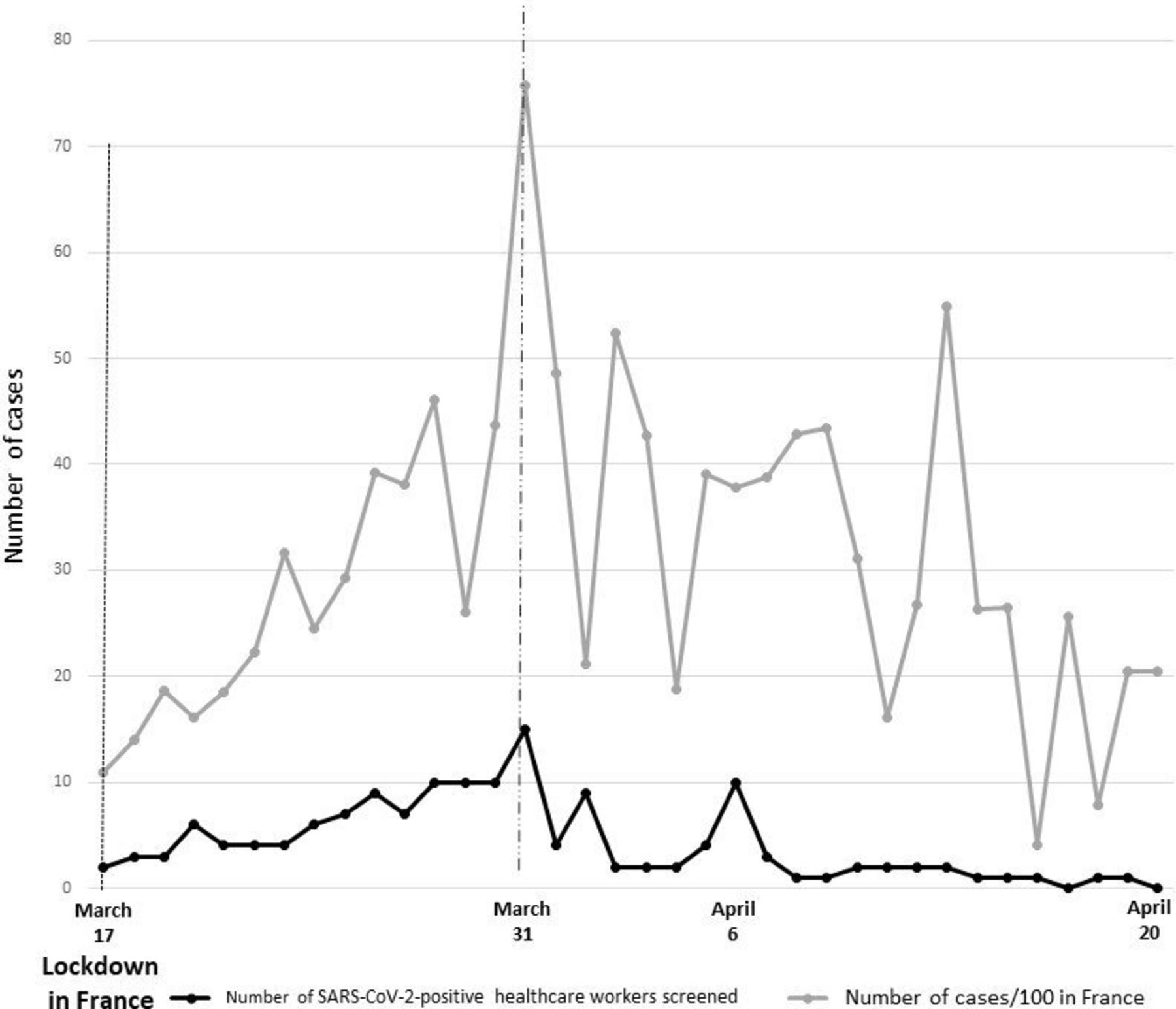
The growth of the number of positive SARS-CoV-2 RT-PCR tests over time among HCWs between 17 March (beginning of the French lockdown) and 20 April (last COVID-19 case identified among HCWs) is illustrated in figure 1. The RT-PCR positivity rate was initially 18 (27%) of 65 HCWs tested during week 1, then rose to 33 (40%) of 82 HCWs tested during week 2, 26 (31%) during week 3, 22 (36%) during week 4 and 8 (21%) at week 5. On 31 March, a total of 13 HCWs tested SARS-CoV-2-positive on the same day in France and 7578 cases were declared. Figure 1 illustrates the epidemic curve in France during the same period (the number of cases has been divided by 100 to facilitate reading).10
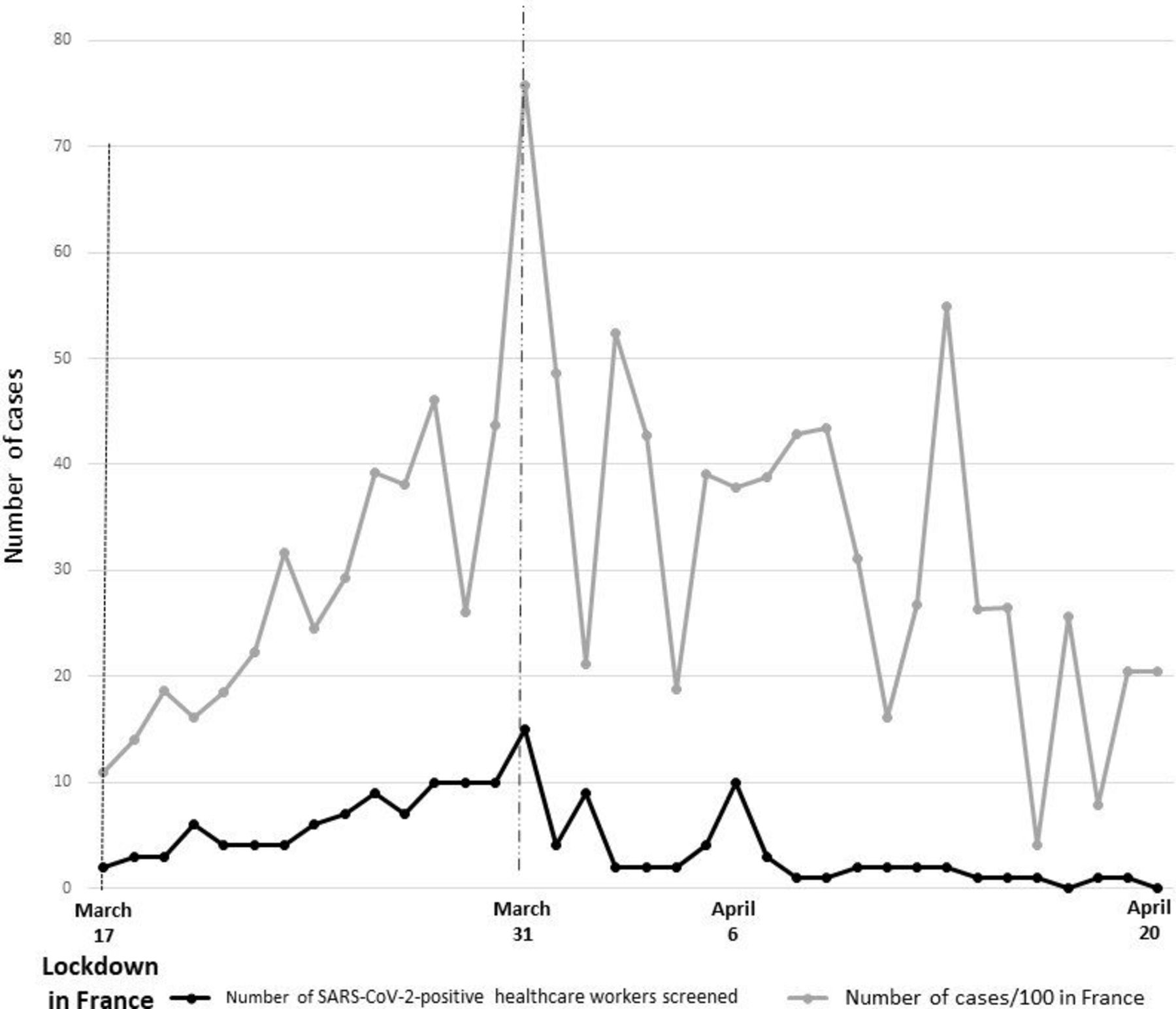
Number of positive SARS-CoV-2 RT-PCR tests per day in the general population in France (divided by 100) and among screened healthcare workers at Creteil Hospital between 17 March and 20 April.
Population characteristics are detailed in table 1. Women represented 81% of the screened population. No difference was found in terms of age, sex, BMI. The median time interval between illness onset and NP swab was 4 days IQR3–7 and did not differ according to the screening result. Positive HCWs were followed for a median of 7 days. At the time of screening, 5 (2%) SARS-CoV-2-negative HCWs were taking corticosteroids compared with 5 (5%) SARS-CoV-2-positive HCWs, p=0.2). Three HCW patients were taking non-steroidal anti-inflammatory drugs and 1 of them tested SARS-CoV-2-positive. Current smokers were less likely to be positive: 53 (27%) SARS-CoV-2-negative HCWs versus 8 (8%) SARS-CoV-2-positive HCWs, p<0.0001. HCWs with an occupational profile directly facing patients more frequently had positive SARS-CoV-2 RT-PCR (82% vs 68%, respectively, p=0.03).
Characteristics of healthcare workers who performed screening according to SARS-CoV-2 RT-PCR results
A large number of clinical symptoms were reported by the patients at clinical onset (table 1). Clinical symptoms significantly associated with positive RT-PCR were fever (48% vs 27%, p<0.0001) and the presence of anosmia (29 (28%) vs 18 (10%), p<0.0001). At screening, no difference was found in terms of heart rate, O2 saturation, temperature or patient self-reported clinical symptoms except for the presence of anosmia, which was reported in 48 (45%) of the SARS-CoV-2-positive HCW patients versus 26 (14%) SARS-CoV-2-negative HCWs (p<0.0001). Patient characteristics 7 days after onset were compared with characteristics at screening in order to assess the clinical course of the illness (table 1, part 3). Tiredness was reported more frequently at day 7 than at screening (71% vs 63%, p=0.01) together with anosmia (70% vs 45%, p<0.0001), diarrhoea (22% vs 15%) and chest pain (14% vs 7.5%). The area under the curve (AUC) of the ROC curve for the presence of anosmia and fever at illness onset was 0.596 (95% CI 0.54 to 0.66) and 0.640 (95% CI 0.57 to 0.71), respectively (figure 2). The two curves were not significantly different (p=0.38). The highest AUC was found with a composite predictor combining the presence of anosmia and/or fever at illness onset (AUC=0.689; 95% CI 0.62 to 0.75) (figure 2).

{kind=link}
{kind=link}
Receiver operating characteristic (ROC) curve of anosmia, fever and a composite predictor (anosmia and/or fever) at illness onset.
Concerning living conditions and entourage, SARS-CoV-2-positive HCWs lived in a median floor space of 70 m2 IQR (50-100) with a median number (IQR) of 3 (2–5) other people (range: 1 to 7). Of the 65 HCWs who reported not living alone, self-isolation (a separate room) was possible in only 49 (52%) HCWs and only 29 (31%) HCWs were able to wear a mask due to general shortages. Among the 65 HCWs not living alone a total of 9 (14%) potentially transmitted SARS-CoV-2 to members of their household based on the date of onset of the symptoms (≥7 days after HCW). Among these nine HCW-to-household transmissions three could self-isolate and among the three only two had the possibility to wear a mask at home. In contrast, three (5%) HCWs probably acquired SARS-CoV-2 from their household. Two deaths occurred among HCW companions, one of whom may have contracted COVID-19 from his HCW companion.
In multivariate logistic regression (table 2), three parameters were identified as being independently associated with a positive RT-PCR test: occupational profile with direct patient facing (OR 3.1 95% CI 1.1 to 8.8), p<0.03), presence of anosmia (OR 5.7, 95% CI 3.1 to 10.6, p<0.0001), while being a current smoker was less likely to be associated with a positive RT-PCR (OR 0.3 95% CI 0.1 to 0.7), p=0.005).
Multivariate analyses of factors associated with positive SARS-CoV-2 RT-PCR
Discussion
To our knowledge, this is the first French study to report occupational exposure, household transmission, symptomatic infection rates, clinical characteristics and outcome among HCWs during the peak of the SARS-CoV-2 epidemic in France during the lockdown period that started on 17 March. France as a whole was unprepared to deal with the epidemic, especially at the beginning of the COVID-19 pandemic, which required implementation of a general lockdown. Although disposable protective equipment, such as masks, was available in French hospitals, the use FFP2 (filtering facepiece) masks had to be strictly limited to high-risk situations.15 The risk of a potential shortage of protective equipment made working conditions more stressful. As already reported, the inexperience for certain HCWs made it even more difficult to deal with this health crisis.16
The local epidemic curve among HCWs was parallel to that of the general population (figure 1), reflecting the same pattern as that of community transmission. Similar results have been observed in other countries, for example, in London hospitals,17–19 although no difference was observed between occupational profile groups. In our study, the overall observed rate of symptomatic SARS-CoV-2 infection was 5.0% and varied according to the occupational profile from 6.4% in group 1, 2% in group 2% and 3% in group 3. The occupational profile with direct patient facing (group 1), such as nurses, doctors, allied health professionals, was also independently associated with symptomatic positive SARS-CoV-2 RT-PCR (table 2). The COVID-19 pandemic resulted in a surge of patients exceeding available human and physical resources, which probably contributed to the higher rate of COVID-19 patient-to-HCW transmission in this group. Hospitals may also amplify an epidemic and epidemics may overwhelm a hospital’s capacity to deliver healthcare services.20 HCW-to-HCW transmission may also have been a possibility, at least at the beginning of the epidemic, as protective measures (such as face mask, eye protection, physical distancing) were not applied during lunch or coffee breaks and at meetings. Some HCWs were also not specifically trained to deal with airborne communicable diseases, in contrast with Asian countries.17 We can also speculate that groups 2 and 3 were more frequently telecommuting and were therefore less exposed to public transport and contacts with colleagues, but unfortunately no data were available.
It is not easy to provide evidence that COVID-19 contamination is a transmission from HCW to household member.21 However, our study provides important insight into HCW-to-household transmission, as we observed 9 (14%) cases of potential transmission based on the date of onset of symptoms (interval ≥7 days between onsets). The choice of the 7-day time interval was based on the median incubation period of 5.2 days (95% CI 4.1 to 7.0).22 23 The upper limit defined for the CI probably even underestimated the real number of HCW-to-household transmissions. A mode of transmission other than HCW-to-household transmission was unlikely, as all outdoor activities were banned during the metropolitan France lockdown, for example, schools were closed, meeting, public transport was very limited, except with a special waiver, such as HCWs. The observed shortage of protective equipment at home (only 39% of SARS-CoV-2-positive HCWs were able to wear a mask at home) and the impossibility of self-isolation (52%) reflect shortages in basic equipment outside hospital settings, at least at the beginning of the epidemic. Genome sequencing could not be performed on HCW household members during the French lockdown in this study. Further genome sequencing might be useful to identify the circulation and transmission of viral subtypes.24
In our study, multivariate analysis showed that anosmia was associated with positive SARS-CoV-2 RT-PCR in symptomatic HCWs. However, the AUC of the ROC curve of anosmia at illness onset was poorly discriminative (AUC=0.596). The composite predictor combining the presence of anosmia and/or fever at illness onset had a better AUC=0.689 (95% CI 0.62 to 0.75) (figure 2). Results of anosmia were concordant with those reported in the literature, as anosmia has been frequently described in patients with SARS-CoV-2.25–27 The new finding reported by this study was the follow-up clinical data, illustrating that anosmia was not a premonitory symptom, as already reported elsewhere,26 but rather tended to occur after several days together with other symptoms such as diarrhoea. The study by Spinato et al 25 focused exclusively on mild forms, which might explain the different interpretation of anosmia. The association of anosmia and hypogeusia and the presence or absence of previous ENT disorders were studied by Benezit et al,27 who found a sensitivity of 42% (95% CI 27% to 58%) and a specificity of 95% (95% CI 90% to 98%) when combining the presence of both symptoms (hypogeusia and anosmia) in patients with no history of ENT disorders.27 Benezit et al 27 reported a retrospective study, associated with a risk of memory bias. Based on our results and those reported in the literature, anosmia has a good specificity and a poor sensitivity for the diagnosis of COVID-19 and should not be recommended as a first-line symptom screening, but more data are needed.
Risks factors associated with severe forms of SARS-CoV-2 were consistent with those reported in the literature.14 Hospitalised patients were more frequently older than 50 years than non-hospitalised patients. Comorbidities were also frequent, as previously described. In our study, current smokers were less likely to have a positive SARS-CoV-2 RT-PCR. These results should be interpreted with caution, as our study was not designed to address this question. To our knowledge, no published peer-reviewed studies have evaluated the risk of SARS-CoV-2 infection among smokers. Such a research question would require well-designed population-based studies controlling for age and relevant underlying risk factors. A review of the literature also identified smoking as a risk factor of more severe forms of the disease.28
One of the strengths of this study is the high participation and response rate. The high participation rate can be explained by the circumstances, as few screening centres were available outside hospitals during the study period and the easiest way to be screened was to go to the hospital at which the HCW worked. Survey questions mainly concerned clinical presentation, which, together with the occupational status, probably explains the high response rate.
A limitation of our study was that, by definition, only symptomatic patients were tested so that the real number of cases was underestimated by excluding asymptomatic cases, who could represent 6%–23% of all SARS-CoV-2 infections.29 30 Asymptomatic cases may have contributed to spread the epidemic among HCWs, at least at the beginning of the epidemic before strict implementation of barrier measures. False-negative RT-PCR results have also been described.31 In the meantime, during the review process of this paper, free serological screening has been proposed to all HCWs since serological testing has been available in France (29 May 2020). Preliminary data, not shown here, estimated an overall prevalence of SARS-CoV-2 (symptomatic or asymptomatic) forms in HCWs of about 12%. This prevalence was obtained after adding symptomatic HCWs with positive PCR to those with positive serology. Some authors recommend that serological testing, RT-PCR swabs and symptom monitoring should be performed in all HCWs.32 However, frequency of testing, feasibility, acceptability and cost should be taken into account.
Conclusion
This is the first French study to report SARS-CoV-2 infection rates among HCWs during the peak of the first wave (spring 2020) of the SARS-CoV-2 epidemic in France and the lockdown period and the risk related to the occupational profile. Our results highlight the risk of HCW-to-household transmission and the lack of protection in households during the peak of the epidemic. Collateral damage to households should be studied in more detail in future research and public health measures should be implemented, such as hotel isolation of SARS-CoV-2-positive HCWs. Now, in October 2020, France is approaching the peak of a second wave of the epidemic, which, according to the Institute for Health Metrics and Evaluation (Washington University) modelling predictions, is expected to be reached between November 2020 and January 2021.33 Although the interval between the two waves was less than 6 months, we hope that we are now better prepared and that the lesson has been learnt allowing a better public health emergency response in terms of equipment, contact tracing, isolation, medical training and protection of household members. Hotel isolation should be proposed to all SARS-CoV-2-positive HCWs not living alone and who are unable to correctly self-isolate at home.
Data availability statement
Data are available upon reasonable request (pascal.andujar@chicreteil.fr or evguenia.krastinova@chicreteil.fr).
Ethics statements
Ethics approval
The study was approved by the local Ethics Committee (n°2020-05-26).
References
Footnotes
Correction notice This article has been corrected since it was published Online First. An additional affiliation has been added for EK.
Contributors EK, CJ, J-CP and PA conceived and designed the analysis. EK, VG, M-TL, AC, EV, ID, AS, MS, MC, BM, J-CP and PA collected the data. EK, J-CP and PA contributed data or analysis tools. EK and PA performed the analysis. EK, J-CP and PA wrote the paper.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.