Article Text

Abstract
Objectives Methicillin-resistant Staphylococcus aureus (MRSA) is an increasing public health concern worldwide. The objective of this study was to calculate a summary odds ratio (OR) of livestock-associated MRSA colonisation and infection in humans, and to determine specific risk factors in livestock production contributing to MRSA colonisation.
Methods We screened PubMed and Embase for studies published from 2005 to 2019 inclusive, reporting livestock-associated (LA)-MRSA colonisation and infection among livestock workers/veterinarians, their families, and community members not regularly exposed to livestock. The primary outcome of interest was the OR of LA-MRSA colonisation comparing exposed and control groups. Quality was assessed according to the Newcastle-Ottawa quality assessment scale. A meta-analysis using a random-effects model was conducted to calculate a pooled OR. The heterogeneity in the meta-analysis was assessed using the I² method, and publication bias was evaluated using funnel plots.
Results A total of 3490 studies were identified by the search, with 37 studies including 53 matched exposed-control groups and 14 038 participants eligible for the meta-analysis. The pooled OR for LA-MRSA among livestock workers and veterinarians is 9.80 (95% CI 6.89 to 13.95; p=0.000; I2 =73.4), with no significant publication bias (Egger’s p=0.66). The OR for swine workers was highest at 15.41 (95% CI 9.24 to 25.69), followed by cattle workers (11.62, 95% CI 4.60 to 29.36), veterinarians (7.63, 95% CI 3.10 to 18.74), horse workers (7.45, 95% CI 2.39 to 23.25), livestock workers (5.86, 95% CI 1.14 to 30.16), poultry workers (5.70, 95% CI 1.70 19.11), and industrial slaughterhouse workers (4.69, 95% CI 1.10 to 20.0).
Conclusions Livestock workers, particularly swine farmers, are at significantly higher risk for LA-MRSA colonisation and subsequent infection. These results support the need for preventive practices to reduce LA-MRSA risk among those who handle and treat livestock.
Trial registration number CRD42019120403.
- meta-analysis
- health and safety
- occupational health practice
- epidemiology
Statistics from Altmetric.com
Key messages
What is already known about this subject?
Methicillin-resistant Staphylococcus aureus (MRSA) carriage is prevalent in livestock farmers, veterinarians, slaughterhouse workers, and butchers. However, whether the MRSA strains were livestock associated (LA) was less well-understood.
What are the new findings?
Livestock workers, particularly swine farmers (with an OR of 15.41), are at significantly higher risk for LA-MRSA colonisation and subsequent infection compared with control populations.
How might this impact on policy or clinical practice in the foreseeable future?
Preventive practices to reduce LA-MRSA risk are recommended among those who handle and treat livestock. In addition, coordinated strategies along livestock supply chains are recommended in farms, especially from regions with high risk of LA-MRSA colonisation.
Introduction
Methicillin-resistant Staphylococcus aureus (MRSA) has become a major cause of antibiotic resistant infections and a broader public health concern worldwide. As one of the most common pathogens in hospital settings, healthcare-associated MRSA (HA-MRSA) is a major cause of skin and soft tissue infections (SSTIs) and severe diseases such as pneumonia and sepsis.1 Twenty-nine per cent of MRSA carriers develop MRSA infection, which increases length of stay in hospitals, additional in-hospital costs and causes thousands of deaths worldwide.2 In the USA, MRSA infections killed over 11 000 hospitalised patients in 2011.3
Since the 1990s, epidemiological characteristics of MRSA have changed greatly. New MRSA lineages have emerged, acquiring different types of the resistance genes responsible for infections occurring in the community (CA-MRSA, community-acquired MRSA).4 MRSA has also become widely distributed among livestock due to routine antibiotic use in livestock farming.5 Livestock-associated (LA)-MRSA strains are different from human MRSA strains, with a higher capacity of establishing and transmitting within livestock herds and potential for spreading and causing infections in humans.6 International trade of livestock has further intensified transmission of LA-MRSA between animals and humans.5 As global meat production and consumption have increased rapidly, farmers are facing pressures to produce livestock more efficiently to meet this demand. Often this involves administration of antibiotics worldwide, which can increase the risk of MRSA associated with livestock production.
LA-MRSA strains can be characterised by multilocus sequence typing, consist of S. aureus protein A (spa) and have a transmissible genetic element called staphylococcal cassette chromosome mec, which carries an element for beta-lactam antibiotic resistance.7 An increasing body of evidence demonstrates that livestock workers are a high-risk population for LA-MRSA carriage due to regular close contact with animals, especially in farm-intensive regions. LA-MRSA has emerged in swine production globally. The prevalence of LA-MRSA colonisation varies widely among livestock workers throughout the world, with reported rate in pig workers of 24%%–86% in Europe, 25%%–45% in North America, and 6%%–19% in Asia.8–11 The epidemiology of LA-MRSA strains differs in different geographic regions. In Europe, MRSA ST398 is the predominant clone complex found in livestock workers or veterinarians. Other clones such as ST1 (the USA), ST5 (the USA and Ireland), ST8 (the USA, Denmark and Switzerland), and ST22 (Ireland) were also identified at lower frequencies in livestock operations. In Asian countries, the presence of various clones of LA-MRSA such as ST9, ST63 and ST2359 were reported in livestock workers.12–14
LA-MRSA isolates have a strong adherence capacity to human keratinocytes, and humans working closely with livestock harbouring LA-MRSA isolates may become colonised.15 LA-MRSA can cause severe SSTIs, which mainly occur in persons with occupational exposure to livestock. LA-MRSA is capable of being established in hospital settings via colonised or infected patients, which can lead to nosocomial infections, although the incidence of these infections is rare.7
A prior systematic review summarised the prevalence of MRSA carriage in livestock workers: farmers (18.2%), veterinarians (9.4%), slaughterhouse workers (2.6%) and butchers (5.7%).16 However, whether the MRSA strains were human-associated or livestock-associated was not distinguished, and the extreme heterogeneity of the results (I2 =96.9%) called into question whether a pooled prevalence estimate such as they provided offered a meaningful statistic. In another study, a 760-fold higher risk of MRSA colonisation was found among a group of regional pig farmers compared with the general population.17
What has already been uncovered about the risk of livestock-acquired MRSA comes from individual studies examining, mostly, the impact of one type of occupation (eg, swine producer, cattle producer and veterinarian) on the risk of LA-MRSA colonisation. These studies range across multiple different species and multiple different occupations, providing a range of odds ratios (ORs) and relative risks when comparing the exposed population to a control population.
The objective of the current study is to calculate a summary OR of LA-MRSA colonisation and infection in humans who are occupationally exposed to livestock and to determine specific risk factors in livestock production contributing to MRSA colonisation. Our unique contribution in this manuscript is to bring together these studies in a systematic review and meta-analysis: to examine and quantify overall risk of occupational LA-MRSA from multiple different nations worldwide and to pool the data from existing studies on each type of occupation to determine that livestock-related occupations result in the highest LA-MRSA risk.
Methods
Data sources and search strategy
We performed a systematic review and meta-analysis of the risk of livestock contact in increasing the incidence of MRSA colonisation in occupational workers and veterinarians. A literature search was conducted on PubMed and Embase databases from 31 October to 21 October 2019. The search terms included combinations of: (“methicillin-resistant Staphylococcus aureus” OR “MRSA”) AND (“livestock” OR “pig” OR “swine” OR “hog” OR “cattle” OR “poultry” OR “farmer” OR “worker”). Retrieved publications were reviewed by examining titles and abstracts, and all potentially relevant articles were subsequently screened as full text. In addition, the search was extended by examining the reference lists of retrieved publications to find more relevant studies linking MRSA carriage with livestock farming or care. No study type or language restriction was imposed. The meta-analyses were conducted according to Preferred Reporting Items for Systematic reviews and Meta-Analyses (PRISMA) guidelines (research checklist). The leading author (CC) screened the search results and identified relevant papers by reviewing retrieved studies. The quality assessment of included studies was conducted by both authors together. Any discrepancies on inclusion were resolved by joint reevaluation of the original full text by both authors. Studies reporting the occurrence of LA-MRSA colonisation among workers/veterinarians and control populations were included in the analysis. The microbiological method based on strain typing was a criterion for presence of LA-MRSA. Studies without control groups, or that did not differentiate between LA-MRSA and other types of Staphylococcus aureus, were excluded. This systematic review is registered with PROSPERO.
Data extraction
The primary outcome of interest was LA-MRSA colonisation among study participants who had close contact with livestock, determined by LA-MRSA strain isolation from nasal, oropharyngeal, or axillary samples. The participants in the eligible studies were divided into exposed and control groups according to their occupational contact with livestock. The exposed group includes the following populations who have direct contact with animals: livestock farmers and veterinarians (including veterinary students) with occupational exposure to various animal species, and slaughterhouse workers including butchers, industrial hog operation and industrial livestock operation workers. The control populations are those who have close proximity to colonised animals but no or minimal direct contact with them, including household and community members of farmers, employees working on farms (eg, salesmen and administrative personnel), antibiotic-free livestock operation workers, and employees not working on farms or treating livestock. These categories allowed the examination of OR of LA-MRSA colonisation among occupations with different levels of exposure to different livestock species.
The following data were extracted from each study: authors, year of publication, study location, study period and duration, study design type, population size, participants’ gender and age (range), type of occupations, strain type and genotype identified, and LA-MRSA colonisation rate and infections among exposed and control participants. In addition, the details of the screening including sampling sites (nasal, oropharyngeal or axillary swabs), MRSA isolation method (culture or PCR), genotyping of isolates, carriage status definition and timeframe of the screening process were retrieved from the studies. Regarding detection methods of microbial isolates, two studies applied a culture method (enrichment broth, sheep blood and chromogenic medium) to screen for carriage of MRSA isolates, which is less sensitive than PCR assays to determine the genotype of MRSA. They were excluded from the analysis. When needed, authors were contacted via email to request additional information.
To ensure that only LA-MRSA strains are included in the meta-analysis, numbers of carriers with spa types not of animal origin were subtracted from the LA-MRSA positive persons.18–20 The secondary outcome of interest was the OR of developing MRSA infections among exposed and control populations. In addition, an index year of each eligible study was determined to model the time trend of LA-MRSA colonisation among participants.
Study quality assessment
Quality assessment of included studies was conducted by both authors according to the Newcastle-Ottawa Scale, a star-based scoring system. Studies that received at least five stars were considered of adequate quality for eligibility.
Data analysis
The OR is a comparison of the odds of an event after exposure to a risk factor (colonisation of LA-MRSA in this analysis) with the odds of that event in a control situation. For each study, matched exposed-control groups were identified, from which ORs and 95% CIs could be calculated between the different exposed and control groups. A random-effects model meta-analysis was conducted to calculate the pooled OR and the associated 95% CI from the eligible studies. Heterogeneity among the selected studies was evaluated using the Cochran’s Q value calculated from the Mantel-Haenszel method and I2 statistic. Sensitivity analyses were conducted by removing each study in turn, and the remaining studies were analysed to determine if the results were significantly impacted by a particular study. The effect of the index year of the study as a covariate on OR of LA-MRSA colonisation was explored through meta-regression analysis for each continent. P values for OR comparisons were calculated using the Fisher’s exact test. Bias in meta-analysis was evaluated by asymmetry in funnel plot and related statistical analyses. All statistical analyses were conducted in Comprehensive Meta-Analysis Software V.2.0.
Results
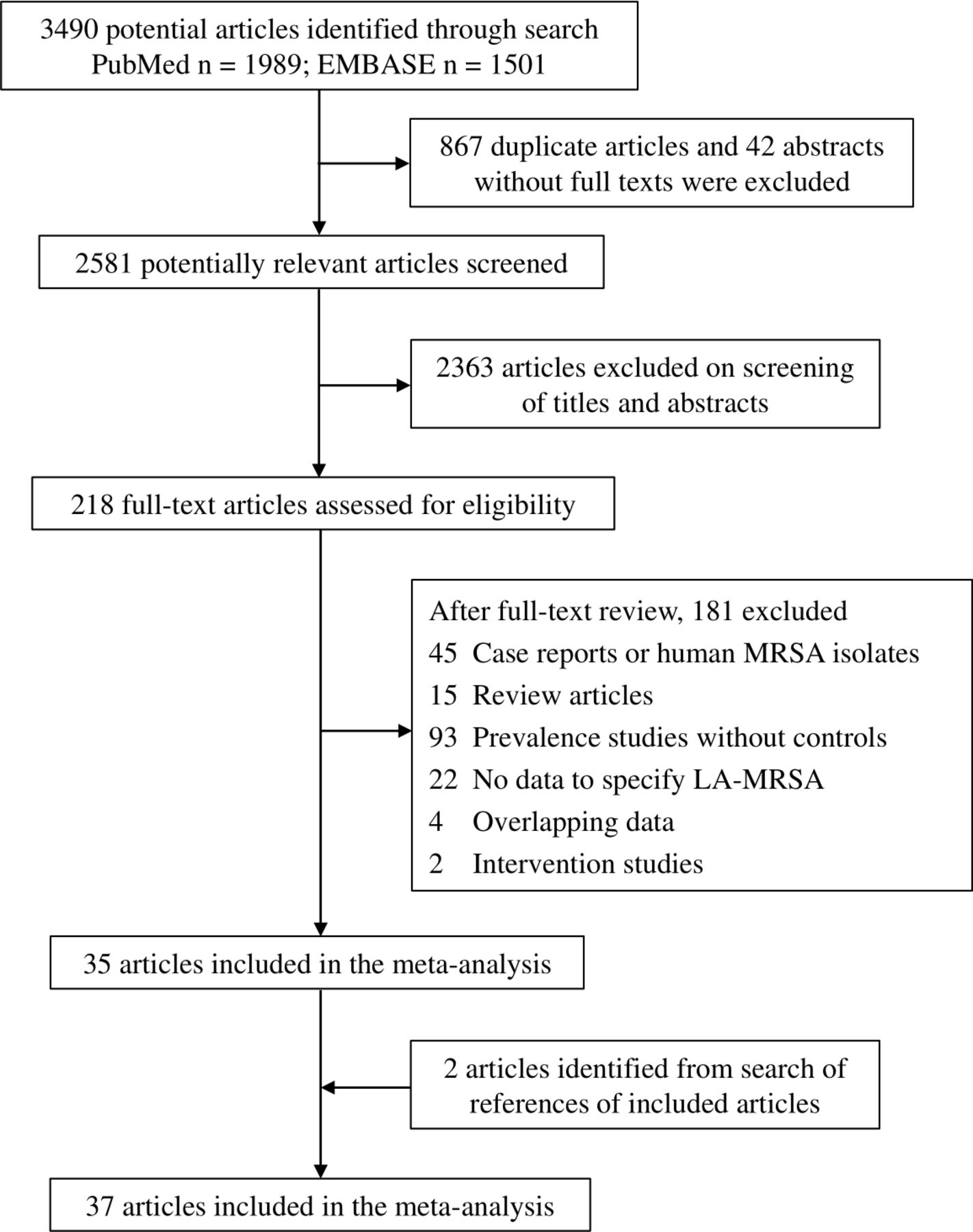
Our literature search retrieved 3490 studies based on our search terms (figure 1). After applying the eligibility criteria described above at the title and abstract level, 2363 studies were excluded. We then retrieved and read the full texts of the remaining 218 studies, from which 35 were selected for sufficient data for our systematic review and meta-analysis. Two of the contacted authors were able to provide information included in the analysis. Two additional articles were identified from search of the references of the 35 included studies. Finally, 37 studies were included in this systematic review and meta-analysis.12–14 18 21–53 Six studies were of six stars, 32 received five stars (online supplemental material table S1).
Supplemental material
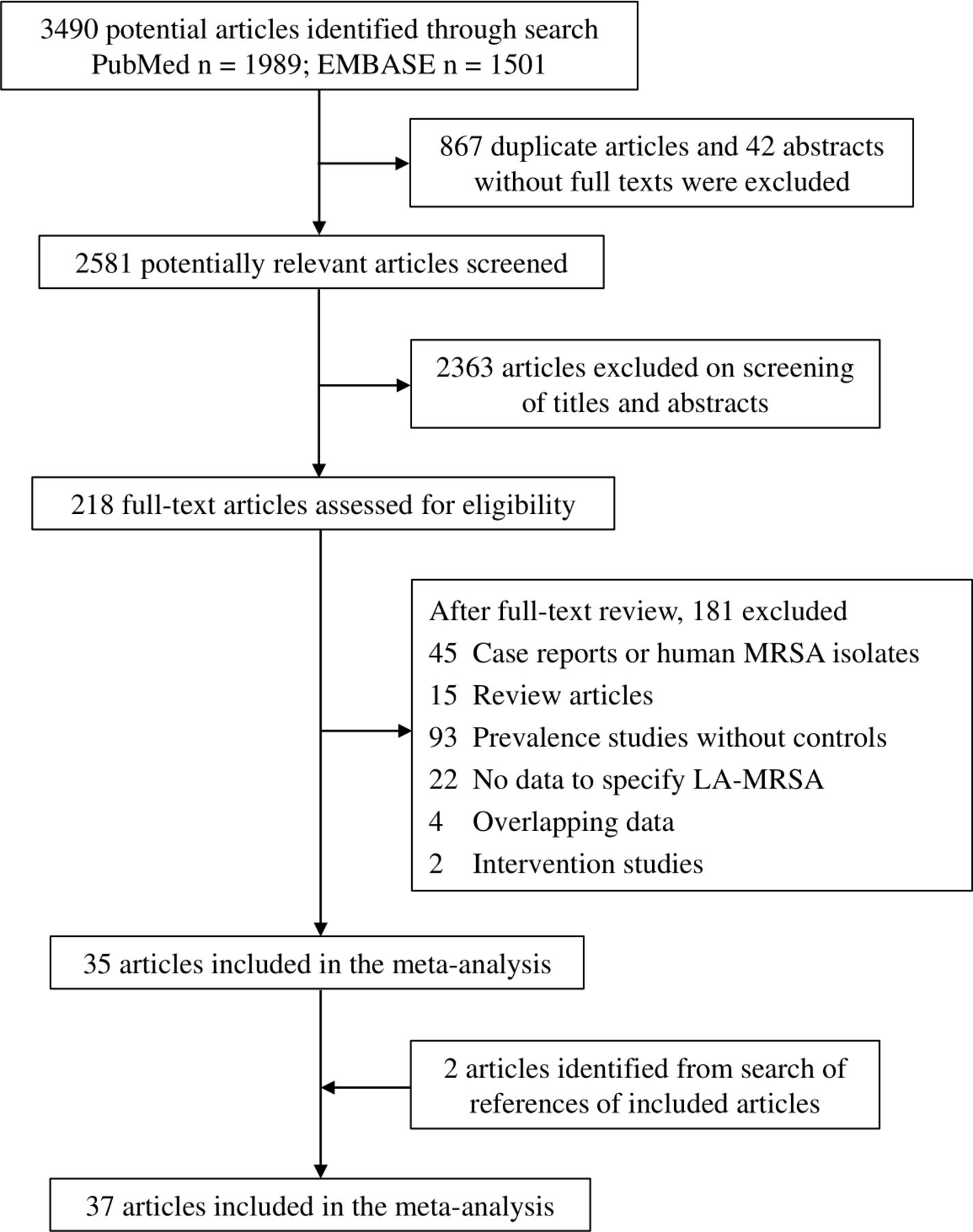
Study selection flow chart. LA-MRSA, livestock-associated methicillin-resistant Staphylococcus aureus; MRSA, methicillin-resistant Staphylococcus aureus.
An overview of the eligible studies is listed in table 1, including the year(s), location and study type; number and occupation of participants and their gender and age; sample type and measurement of colonisation; spa type; number of LA-MRSA carriers in exposed and control populations; and the number of MRSA infection cases. The 37 eligible studies on LA-MRSA colonisation and occupational livestock exposure consist of 26 cross-sectional studies, 5 prospective cohort studies, 3 case–control studies and 3 longitudinal studies published between 2005 and 2019 from nine countries, comprising 53 exposed-control groups and 14 038 participants. Twenty-one studies assessed the risk of MRSA carriage in occupational pig workers, 10 in veterinarians, 7 in cattle workers and 5 in poultry workers.
Summary of studies included in the meta-analysis (n=37)
The overall pooled OR of LA-MRSA carriage among exposed populations based on the random-effects model was 9.80 (95% CI 6.89 to 13.95; p=0.000; I2 =73.4) compared with control populations, among 53 exposed-control subgroups, indicating that livestock contact is a significant risk factor for LA-MRSA colonisation in humans. Stratifying the studies by geographical regions, the pooled OR from Asian countries (farm workers vs non-farm workers) was 4.03 (95% CI 1.44 to 11.29; p=0.15; I2 =46.9). Among European countries, the pooled OR was 9.56 (95% CI 6.90 to 13.25; p=0.000; I2 =76.5). A relatively lower OR (4.69, 95% CI 1.10 to 20.05; p=0.94; I2 =0.000) was found in the USA. Figure 2 shows classifications and population size of subgroups according to their occupational contact with livestock farming and the forest plots for the pooled OR and 95% CI of LA-MRSA colonisation among all exposed subgroups.

Forest plots of the OR and 95% CI for studies of LA-MRSA colonisation among subgroups who have contact with different animal species. The squares indicate or estimate within each subgroup; the diamond at the bottom indicates the pooled OR estimate in the meta-analysis according to the random-effects model.
When stratifying occupations of the study participants by different animal species, the highest OR was seen in pig workers (15.41; 95% CI 9.24 to 25.69; p=0.000; I2 =68.7), followed by cattle workers (11.62, 95% CI 4.60 to 29.36; p=0.000; I2 =79.0), veterinarians (7.63, 95% CI 3.10 to 18.74; p=0.000; I2 =77.9), livestock workers (5.86, 95% CI 1.14 to 30.16; p=0.23; I2 =32.6), poultry workers (5.70, 95% CI 1.70 to 19.11; p=0.006; I2 =72.3) and industrial operation workers (4.69, 95% CI 1.10 to 20.0; p=0.94; I2 =0.000). Horse workers were 7.45 times (95% CI 2.39 to 23.25; p=0.17; I2 =47.6) more likely to be colonised by LA-MRSA compared with control participants based on two relevant studies. One study reporting risk of LA-MRSA colonisation among patients with sheep contact did not show a different risk (1.0, 95% CI 0.14 to 7.24) than control population.
Medium to substantial heterogeneity (I2 ≥50) was observed in the subgroups of cattle farmers, veterinarians and poultry workers. The sensitivity analyses show that excluding the most heavily contributing study resulted in significantly reduced heterogeneity within these subgroups (figure 3).

{kind=link}
{kind=link}
{kind=link}
Forest plots for one-study-removed meta-analysis of OR among cattle workers (A), poultry workers (B) and veterinarians (C). The plots show the OR estimate when each study is removed from the meta-analysis. The deviation from the full analysis indicates the sensitivity of the full analysis with respect to each study, indicating the weight a particular study contributes to the meta-analysis. LA-MRSA, livestock-associated methicillin-resistant Staphylococcus aureus.
The time trend plot (online supplemental material figure S1) on the basis of index year of the eligible studies indicated that a decreasing trend of LA-MRSA colonisation among livestock workers existed only in European countries (fixed effect, p=0.046), but not in North America (p>0.5) or Asia (p>0.5). Three of the selected studies recorded SSTI among the participants. The risk for MRSA infections based on these studies was 3.44 (95% CI 0.20 to 58.3; p=0.015; I2 =76.1) among occupational livestock workers. In hospital settings, infections with more serious symptoms and outbreaks caused by LA-MRSA among persons with occupational livestock contact have also been reported.
Publication bias was assessed by a funnel plot (online supplemental material figure S2). The associated statistical test (Egger’s test p=0.66) of funnel plot asymmetry indicated that publication bias was not a serious limitation in our meta-analysis.
Discussion
Our analysis indicates that livestock-exposed populations were 9.80-fold more likely to be colonised by LA-MRSA than the control population. In particular, pig farmers had the highest OR for LA-MRSA colonisation of 15.41. The differences in ORs for different livestock species may result from differences in basic facilities and operations across the species, or differences in transmissibility of LA-MRSA between each of these species and humans.
Our study has several limitations. The prevalence of LA-MRSA carriage in human population is associated with animal-to-human transmission, human-to-human transmission and airborne route.54 Intensive contact with livestock allows LA-MRSA to persist in workers, and transmission events can occur on farms and beyond farms. Thus, the long-term persistence of the carriage is considered to play a key role in the transmission dynamics of LA-MRSA.55 In this regard, a main limitation of our analysis is that the transmission dynamics of LA-MRSA was not taken into account when using the association between cause and effect in epidemiology. For the majority of the selected studies, whether the LA-MRSA carriage patterns were intermittent or persistent was not identified in studies that took cross-sectional nasal and/or throat samples; only six studies examined samples longitudinally at multiple time points in which occurrence of MRSA carriage over time is associated with the use of antibiotics and other determinants.21 26 45 50 51 New evidence suggests that colonisation of ST398 in humans is potentially more persistent; the transmission from farm workers to their household members occurs at a low but consistent percentage.2 23 Therefore, we assumed the carriage of LA-MRSA being in equilibrium, although this state is practically subject to change due to population dynamics and stochastic events in the transmission. Nonetheless, the weight of evidence shows that occupational livestock contact puts the workers at higher risk for LA-MRSA colonisation.56
We should take into account that a single nasal or throat swab is not a proof of colonisation of LA-MRSA, which has been shown to be a relatively weak coloniser in humans, where carriage of MRSA can disappear in the absence of animal exposure. However, in the majority of the selected studies, nasal and/or throat swab samples were collected for the detection of LA-MRSA carriage, except two studies in which the strain isolates were collected from patients infected with LA-MRSA, which may overestimate the number of positive individuals and therefore is another limitation of our study. Moreover, colonisation of ST398 in humans has the potential to be more persistent and a strong link exists between occupational animal contact and persistent LA-MRSA colonisation.2 44 Participants in the studies reviewed here generally have long-term repetitive contact with livestock, which is a major risk factor for persistent LA-MRSA carriage in humans.
Because no associations of the risk of LA-MRSA colonisation were found for demographic information (dietary preferences, exposure to raw meat, smoking, contact sports and travel) and medical history (exposure to healthcare facilities and antibiotic usage),12 23 26 these variables were not considered as risk factors in our meta-analysis. In intensive farming, some livestock workers take preventive measures during work to reduce the risk of bacterial infection. Unfortunately, these measures have not been broadly successful for preventing occupational acquisition of LA-MRSA. For example, the majority of industrial hog operators wear protective footwear, long sleeves, long trousers or coveralls when working in operation areas.35 However, the OR (4.69) of LA-MRSA colonisation among this group was still significantly higher than control population. Moreover, implementing nationwide eradication programmes has proven difficult.54 Although the majority of LA-MRSA colonisation cases in occupationally exposed persons may be asymptomatic, a quantitative association between LA-MRSA carriage and infection still needs to be investigated in the future research.
The time trend analysis shows a decreasing risk of LA-MRSA colonisation among livestock workers in European countries. This may be due to multiple different phenomena. Farming practices may be improving to reduce LA-MRSA transmission risk, including methods to keep animals healthy without the need for antibiotics; such as the use of vaccines, nutritional supplements, prebiotics, probiotics or synbiotics, and waste management strategies.57 Veterinarians are more informed than ever about the risks of antimicrobial resistance; hence, they are careful in their own use of antibiotics with animals as well as the advice that they provide to livestock and poultry farmers. However, changes in the prevalence in control populations may also contribute to the change in risk of colonisation over time. We calculated the time trend of the risk difference of LA-MRSA carriage between populations with intensive animal contact and those in the control population and found that the risk difference remains stable over time (p>0.1) based on a meta-regression analysis, which might suggest an equilibrium of prevalence of LA-MRSA between the exposed and control groups.
Most (28 out of 37) of the selected studies are originated from European countries, but the risk of LA-MRSA colonisation varied widely among countries. This may be because of different regulations or enforcement of regulations regarding animal operations (including antibiotic use) across countries or because of differences in climate (temperature and precipitation) that could affect MRSA transmission rates. Trading colonised animals between countries is a vehicle and considered as another major risk factor for transmission of LA-MRSA between humans and pigs.58 In MRSA-free areas, livestock imports should be considered an important route of introduction of LA-MRSA into livestock populations.59 The LA-MRSA strains in pig supplying farms from regions with high risk of LA-MRSA colonisation can highly affect the MRSA status of the recipient farms. In addition, associations have been observed between MRSA infections and high-density livestock production.7 Coordinated strategies along livestock supply chains are recommended to control and prevent LA-MRSA in livestock farming and trade.
The source of heterogeneity in the meta-analysis is also a limitation. Many studies providing the prevalence of LA-MRSA among livestock workers without a control population were excluded, prohibiting a calculation of an OR. Currently, there is lack of consensus on validated markers for detecting livestock-associated S. aureus, which may be a source of heterogeneity in our analysis. Absence of scn, positivity of mecA and tetracycline resistance are recognised as main indicators of livestock association among MRSA isolates.35 However, these characteristics have also been found in other lineages. Some strains of LA-MRSA appear to be phylogenetically originated in humans and evolved a variety of adaptations via transmission and spread among hosts.60 As a result, some strains of LA-MRSA may be human associated. Second, no selected studies originated from Africa or South Asia, which influences the representativeness of our analysis but highlights the need for further research in these regions.
The risk of developing LA-MRSA colonisation among livestock workers and veterinarians is also affected by other risk factors: livestock density and the type of farm or stage of animal production (eg, LA-MRSA transmission risk was higher in sows than finishing pigs), antimicrobial use history, hospital admission, working on farms with MRSA-positive animals, herd size and sanitary conditions.23 46 56 These factors vary among individuals and different geographical regions, representing additional source of heterogeneity. However, these variables have not been measured in the majority of the selected studies. Our analysis summarised a combined estimate of the OR but was not able to identify the contributions of these risk factors to LA-MRSA colonisation among study participants.
The principal strength of our study is the analysis of the OR of LA-MRSA colonisation and infection among livestock workers and veterinarians as the main outcomes of the occupational contact with livestock. The pooled OR indicates a high risk and major burden of LA-MRSA colonisation and infection currently involved in livestock contact, which underscores the importance of this clone for global occupational health. Occupational exposure to pigs is the most important factor for LA-MRSA carriage, which underscores the importance of this clone for global occupational health. Future studies should focus on implementing interventions in livestock farming and operation and veterinary settings and determining the effectiveness of these interventions in reducing LA-MRSA colonisation among occupational workers and veterinarians.
Conclusion
The review shows that livestock workers, particularly swine farmers, are at significantly higher risk for LA-MRSA colonisation and subsequent infection. These results support the need for preventive practices to reduce LA-MRSA risk among those who handle and treat livestock. In addition, coordinated strategies along livestock supply chains are recommended in farms, especially from regions with high risk of LA-MRSA colonisation, to control and prevent LA-MRSA in livestock farming.
Ethics statements
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Contributors FW conceived and designed the study. CC did the literature review and data extraction. Both authors evaluated the studies. CC was involved in the data synthesis and statistical analysis. CC and FW contributed to the interpretation of the data and writing of the manuscript. Both authors agreed with its content and approved the final submitted version.
Funding This study was funded by USDA grant MICL02527 (FW).
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.