Article Text

Abstract
Objective To evaluate what is currently known about the risk to surgeons and other operating theatre (OT) staff of human papillomavirus (HPV) transmission and HPV-related disease following surgical smoke exposure.
Methods A systematic literature search of Embase and Ovid-MEDLINE was undertaken for primary studies relevant to the presence of HPV in surgical smoke, contamination of OT staff with HPV after performing or attending smoke-generating surgical procedures, and the presence of HPV or HPV-related disease in OT staff following occupational surgical smoke exposure. Additional articles were identified by searching the reference lists of relevant published papers.
Results Twenty-one relevant articles were identified. These demonstrate that surgical smoke from the treatment of HPV-related lesions can contain HPV DNA, and that this can contaminate the upper airways of OT staff. Whether this corresponds to infectious virus is not known. Increased prevalence of HPV infection or HPV-related disease in OT staff following occupational exposure to surgical smoke has not been convincingly shown.
Conclusions While HPV transmission to OT staff from surgical smoke remains unproven, it would be safest to treat surgical smoke as potentially infectious. Necessary precautions should be taken when performing smoke-generating procedures, consisting of: (1) local exhaust ventilation, (2) general room ventilation and (3) full personal protective equipment including a fit tested particulate respirator of at least N95 grade. There is currently insufficient evidence to recommend HPV vaccination for OT staff or to state that the above precautions, when used properly, would not be effective at preventing HPV transmission from surgical smoke.
- health and safety
- hygiene / occupational hygiene
- occupational health practice
- viruses
- virology
Statistics from Altmetric.com
Key messages
What is already known about this subject?
Inhalation or contact with surgical smoke is potentially hazardous to surgeons and other operating theatre (OT) staff.
Smoke-generating surgical procedures are commonly used for the treatment of human papillomavirus (HPV)-related lesions.
Surgical smoke may represent a potential vehicle for the transmission of HPV to surgeons and other OT staff, leading to HPV infection and subsequent HPV-related disease.
What are the new findings?
Surgical smoke generated from the treatment of HPV-related lesions can contain HPV DNA (Royal College of General Practitioners evidence rating ***).
HPV DNA from surgical smoke can contaminate the upper airways of OT staff (**).
It remains unknown whether surgical smoke contains inactivated viral DNA or viable HPV capable of infecting those it comes into contact with.
Increased prevalence of HPV-related disease in OT staff following surgical smoke exposure has not been convincingly shown (*).
How might this impact on policy or clinical practice in the foreseeable future?
It is safest to treat surgical smoke from the treatment of HPV-related lesions as containing potentially infectious HPV particles, and to take all reasonable measures to minimise OT staff smoke exposure.
Precautions should ideally include a triple combination of: (1) local exhaust ventilation, (2) general room ventilation and (3) full personal protective equipment including a fit tested particulate respirator of at least N95 grade.
There is insufficient evidence at present to recommend HPV vaccination in OT staff, or to state that the combined safety measures recommended above, when used properly, would not be sufficient to prevent HPV transmission from surgical smoke.
Introduction
The Papillomaviridae is a family of small non-enveloped DNA viruses, which infect mucosal and cutaneous epithelia of animals and humans.1 Over 200 different human papillomaviruses (HPVs) have been identified thus far.2 Of these, a subgroup of 12 mucosal HPVs are oncogenic and are referred to as high-risk HPVs (HR-HPVs): HPV16, 18, 31, 33, 35, 39, 45, 51, 52, 56, 58 and 59.2 The HR-HPVs are the causative agents of multiple types of cancer, including cancers of the cervix, vagina, vulva, anus, penis and oropharynx.2 Of the low-risk HPVs (LR-HPVs), HPV6 and 11 are the etiological agents of benign genital warts (condylomata acuminata) and recurrent respiratory papillomatosis, while cutaneous HPV types 2, 3, 7, 10, 27, 28 and 57 are the cause of common and plantar warts (verruca vulgaris).2 The nonavalent HPV vaccine Gardasil9 provides protection against infection with HR-HPV types 16, 18, 31, 33, 45, 52 and 58, and LR-HPV types 6 and 11.3
Surgical smoke or plume is a gaseous by-product generated during a variety of surgical procedures, including diathermy, electrocautery, laser ablation/irradiation, electrosurgical excision, ultrasonic (harmonic) excision and high speed drilling, sawing or burring.4–7 It is formed and released into the operating theatre (OT) environment through thermal disintegration and vaporisation of tissue constituents during such procedures.5 Inhalation or contact with surgical smoke is potentially hazardous to surgeons and other OT staff.4–7 Smoke-generating surgical procedures are commonly used for the treatment of HPV-related lesions,8–10 and thus there is growing concern that surgical smoke represents a potential vehicle for the transmission of HPV to OT staff, leading to HPV infection and the subsequent development of HPV-related disease.10 While many reviews have been written on the general hazards of surgical smoke,11–25 there exists a paucity of comprehensive systematic review articles focusing specifically on HPV and surgical smoke. The aim of this systematic review is to address this need and evaluate what is currently known about the risk to OT staff of HPV transmission and development of HPV-related disease following surgical smoke exposure.
Methods
Search strategy
A systematic literature search of Embase and Ovid-MEDLINE was conducted on 6 November 2019 in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses Statement guidelines.26 The search aimed to identify any primary studies relevant to the presence of HPV in surgical smoke, HPV contamination of OT staff after performing or assisting with smoke generating surgical procedures, and the occurrence of HPV-related disease in OT staff following occupational surgical smoke exposure. Alternative terms for surgical smoke and common smoke-generating surgical devices were derived from previous reviews on surgical smoke and incorporated into the search strategy.4–7 The full Embase and Ovid-MEDLINE electronic search queries and database years covered are included in the online supplementary material. A secondary search for additional relevant articles was undertaken by checking all references of potentially relevant articles identified in the primary literature search. Following this, articles referenced by papers identified in the secondary search were also checked for relevance, and so on until search saturation was reached. The strength of the evidence leading to conclusions regarding the risk to OT staff of HPV transmission and development of HPV-related disease following surgical smoke exposure was graded using the Royal College of General Practitioners (RCGP) three-star rating system: level of evidence ‘***’, generally consistent finding in a majority of multiple acceptable studies; ‘**’, either based on a single acceptable study or a weak or inconsistent finding in some of multiple acceptable studies; ‘*’, limited scientific evidence, which does not meet all the criteria of acceptable studies.
Supplemental material
Study selection
The deduplicated search results were independently screened by title and abstract by two authors (AF-L and CA) to avoid bias. Where disagreement existed regarding the relevance of an article, a third author (SR) independently screened the articles in question and made the final decision. Articles were included for review if they were primary studies published as journal articles or conference abstracts, in any language at any time, specifically looking for evidence of: (1) HPV contained within surgical smoke; (2) contamination of equipment or treatment fields with HPV from surgical smoke; (3) contamination of OT staff with HPV following surgical smoke exposure and (4) HPV-related disease in OT staff following surgical smoke exposure. Articles were excluded if they were non-primary studies (such as review articles), animal studies, case reports or were not relevant to the transmission of HPV specifically via surgical smoke (such as transmission of HPV to OT staff via other routes such as direct contact). Articles that were not excluded through title and abstract review underwent full text review by one author (AF-L) to confirm relevance with the same inclusion and exclusion criteria applied.
Results
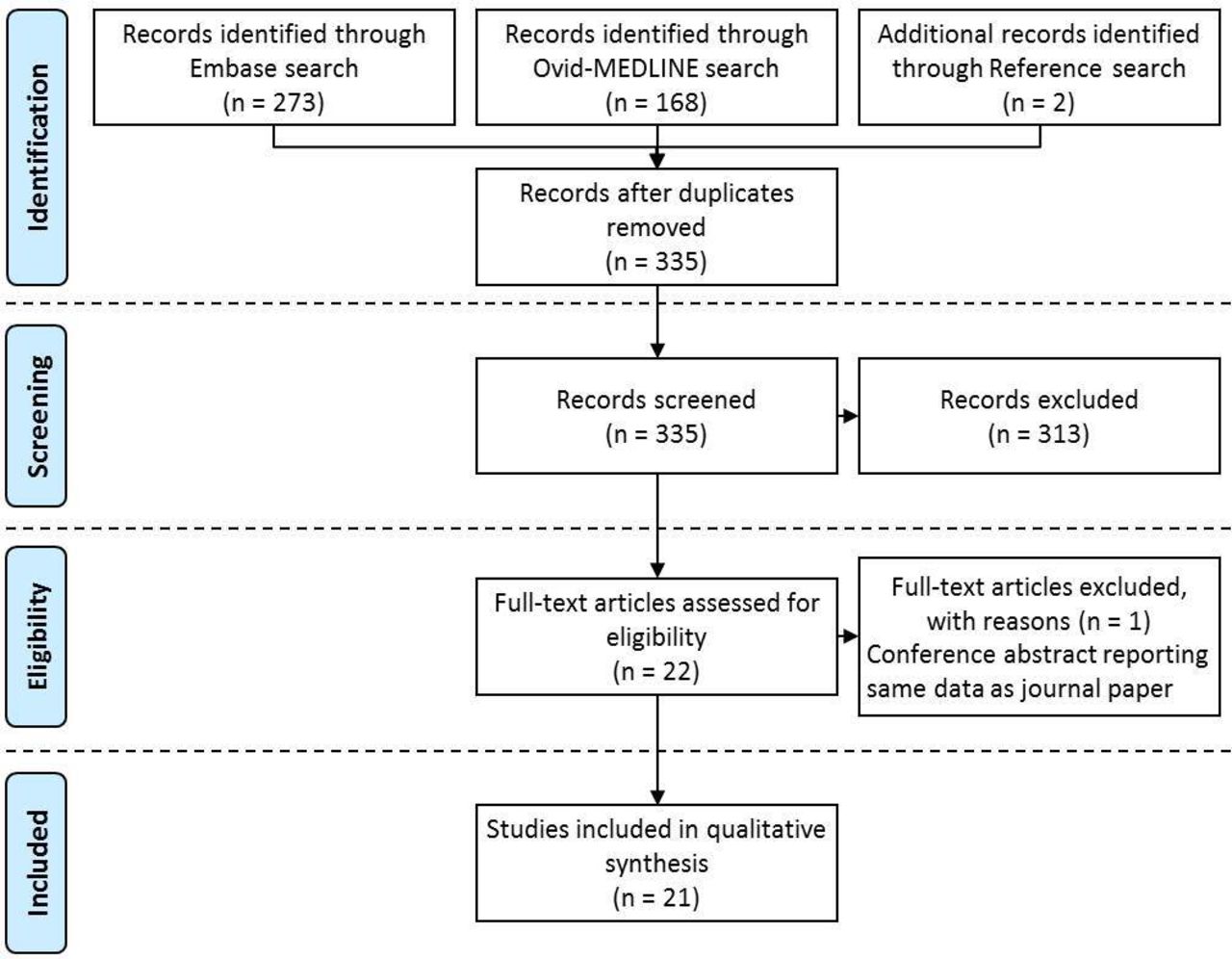
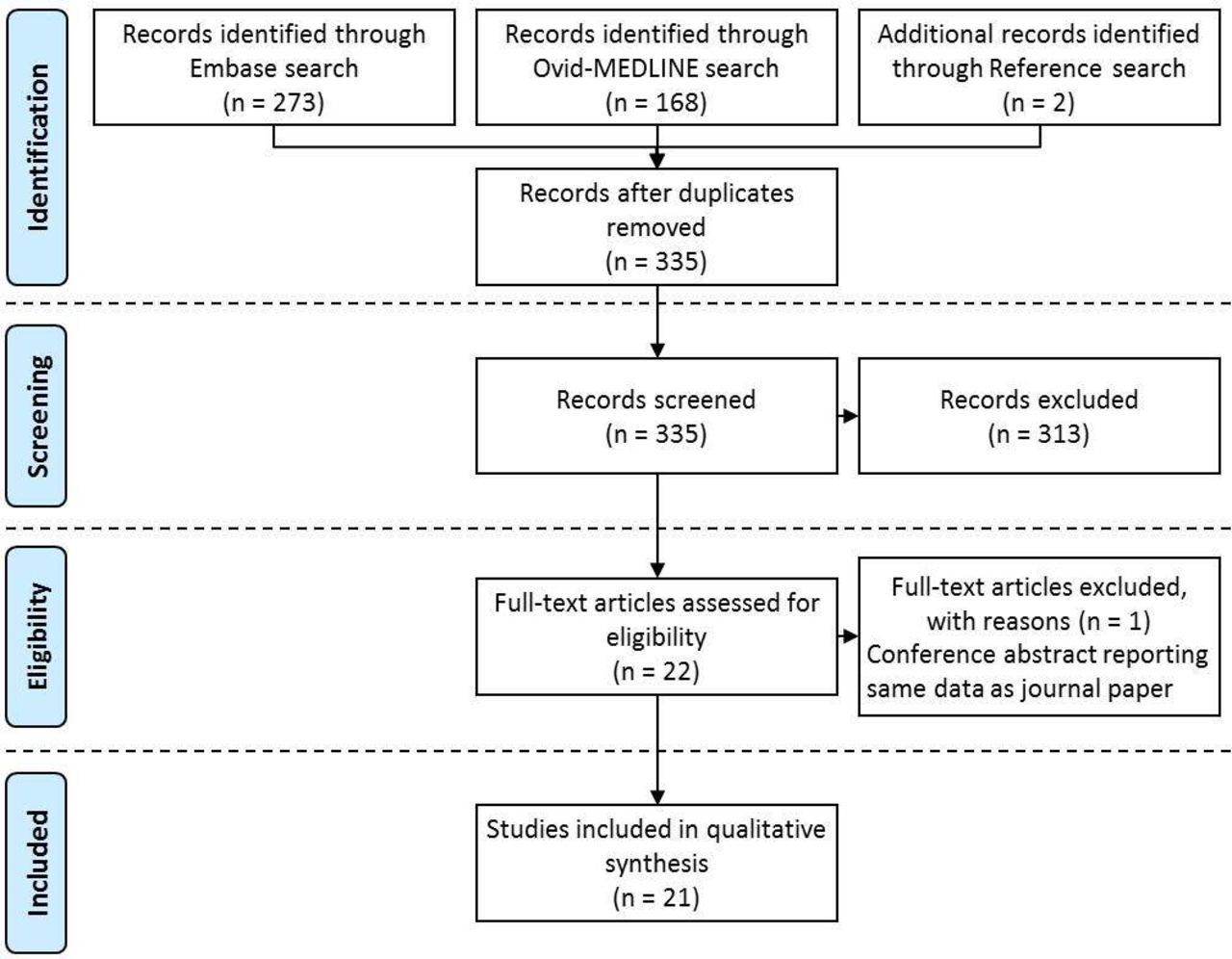
The primary systematic literature search and secondary search of references generated 335 articles after deduplication. Following exclusion of 313 non-relevant articles through title and abstract screening, 22 articles were assessed for eligibility by full text review. One article was excluded at this stage as it was deemed to be a conference abstract reporting the same results as another published study by the same authors.27 A total of 21 relevant articles were included in the final qualitative synthesis (figure 1).28–48 Articles were grouped by study type and their key findings summarised accordingly, with studies or components of studies involving human participants (eg, surgeons/operators and other OT staff) described in greater detail. Where an article included multiple study types (such as the presence of HPV in surgical smoke and HPV contamination of OT staff following surgical smoke exposure) these components were analysed separately.
{kind=link}
PRISMA diagram of article selection procedure. PRISMA, Preferred Reporting Items for Systematic Reviews and Meta-Analyses.
HPV in surgical smoke
Fourteen studies were identified which set out to demonstrate, either directly or indirectly, the presence of HPV DNA in surgical smoke.28–41 The design and findings of these studies are summarised in table 1. Surgical smoke was analysed from a variety of treatment modalities, including carbon dioxide (CO2) laser ablation, erbium:yttrium-aluminum-garnet (YAG) and holmium:YAG laser ablation, and loop electrosurgical excision procedures (LEEP). CO2 laser ablation was the most studied paradigm, with nine studies examining surgical smoke produced by CO2 laser ablation of HPV-induced lesions.28–34 36 38 Of the 12 studies directly measuring HPV DNA in surgical smoke, HPV DNA was detected in 10 studies, with the HPV subtypes detected in smoke generally matching those detected in the corresponding clinical samples.29–31 33–35 38–41 Two studies attempted to demonstrate the presence of viable HPV in surgical smoke indirectly: one study collected smoke from laser ablation of genital warts and tested it for evidence of metabolic activity,28 while the other study involved inoculating human and porcine cell lines with surgical smoke from laser ablation of laryngeal papillomas and looked for signs of subsequent cellular infection.36 Neither of these studies were able to show that surgical smoke contained a metabolically active infectious agent.
Studies analysing surgical smoke for the presence of HPV DNA or viable infectious material
HPV contamination of equipment and treatment fields
Three studies were identified which attempted to detect HPV DNA in treatment fields following laser ablation of HPV-related lesions.38 42 43 Two of these studies found HPV DNA in the environment: in 7/43 (16%) treatment fields tested and in 2/15 (13%) surveillance petri dishes, respectively,42 43 with HPV DNA detected in surveillance petri dishes placed up to two metres from the operating field. In these studies, the HPV was not typed so it is uncertain if the HPV detected in the environment corresponded to that in the clinical tissue subject to the smoke-generating procedure. The third study did not demonstrate clinically relevant HPV in the 66 surveillance petri dishes analysed.38 A fourth study looked for HPV DNA on laser fibres used in ablation of laryngeal papillomas, but did not detect any.44 These studies are summarised in table 2.
Studies analysing equipment and treatment fields for the presence of HPV DNA
HPV contamination of medical personnel exposed to surgical smoke
Five studies were identified which sought to determine if contamination of medical personnel with HPV occurred following direct exposure to surgical smoke.33 38 41 43 45 These studies involved sampling various smoke exposed sites on the operator after they had performed smoke generating procedures on HPV-related lesions, and then analysing the samples for the presence of HPV DNA. Two of these studies failed to detect any HPV DNA in the operator samples.33 38 One study found HPV DNA on postoperative samples from operator gloves but not their oral mucosa,45 and two studies detected HPV DNA in operator nasal samples postoperatively.41 43 These studies are summarised in table 3.
Studies looking at HPV contamination of medical personnel following exposure to surgical smoke
The first of these studies, undertaken in 1990 by Ferenczy et al, involved sampling the nasopharynx, eyelids and ears of a single laser surgeon before and after they performed CO2 laser surgery on patients with anogenital and cervical condylomata.33 Samples were collected before and after nine laser treatment sessions (11–13 patients per session, with 110 patients treated in total) and analysed for the presence of HPV DNA using a filter hybridisation technique. It was noted that during laser treatment sessions, both general room ventilation and local smoke extraction were used in the OT, and a standard surgical mask and plastic goggles were worn by the laser surgeon. In this study, HPV DNA was detected in 65/110 (59%) clinical samples, but was not detected in any of the pre-treatment or post-treatment session samples from the operating laser surgeon.
The second such study, by Bergbrant et al in 1994, involved sampling the nostrils, nasolabial folds and conjunctiva of operators before and after they performed CO2 laser ablation or electrocoagulation (diathermic) treatment of genital warts.43 This study used PCR to detect HPV DNA, which was deemed to be more sensitive than the filter hybridisation technique used in the prior study by Ferenczy et al.33 As with the previous study, standard surgical masks and plastic goggles were worn by the operators, though masks were noted to be worn inconsistently during electrocoagulation sessions. The use of general room ventilation or local smoke extraction was not mentioned. In operators performing electrocoagulation, 2/51 (4%) pre-treatment operator samples tested positive for HPV DNA compared with 9/51 (18%) post-treatment samples, though results were not further stratified based on mask use. In operators performing CO2 laser ablation, 5/28 (18%) pre-treatment and 6/28 (21%) post-treatment samples were positive for HPV DNA. In this study, no attempt was made to correlate the HPV types detected in the operator samples with those present in the clinical lesions being operated on, and it is unclear whether the increased rate of operator contamination seen following electrocoagulation was due to the procedure itself or the variable adherence to mask use.
Weyandt et al performed another similar study in 2011, with the glasses and nasolabial folds of operators being sampled before and after ten treatments of genital warts with multilayer argon plasma coagulation.38 The presence of HPV DNA in samples was determined using PCR. The nature of the personal protective equipment (PPE) used and OT smoke extraction measures were not described. In this study, tissue samples from the lesions being treated were also analysed for the presence of HPV DNA to allow for correlation with positive operator samples. Of the 20 operator samples, two (10%) tested positive for HPV DNA, but the HPV subtypes identified in the operator samples did not match those in the corresponding clinical samples.
In 2012, Ilmarinen et al sampled the surgical masks, gloves and oral mucosa of operating surgeons and other attending OT staff before and after CO2 laser ablation treatments of laryngeal papillomas and genital warts.45 Samples were tested for the presence of HPV DNA by PCR. Protective goggles, surgical gloves and standard surgical masks were used during each operation, but smoke extraction measures were not described. All oral mucosa and surgical mask samples from medical personnel tested negative for HPV DNA, whereas 14/20 (70%) of the post-treatment surgical glove samples tested positive for HPV DNA, with the HPV subtypes detected matching those in the corresponding clinical samples.
The most recent, and also the most comprehensive study looking at HPV contamination of medical personnel following surgical smoke exposure was conducted by Zhou et al.41 In this study, the nasal epithelia of 31 operators were sampled before and after performing 134 LEEP on HPV-associated cervical intraepithelial neoplasia lesions. Exfoliated cervical cells from patients were also collected to allow for HPV subtype correlation between operator and patient clinical samples. A total of 268 operator nasopharyngeal swabs and 134 patient cervical samples were collected and tested from the presence of HPV DNA using PCR, with any HPV detected then undergoing further subtyping. Local smoke evacuation was noted to have been used during all procedures, though general room ventilation was not mentioned. This was the only study identified in which N95 particulate respirators were used, with standard surgical masks being worn during 94/134 (70%) procedures, and N95 particulate respirators being worn during 40/134 (30%) procedures. None of the 134 operator pre-treatment samples tested positive for HPV DNA. Postoperatively, HPV DNA was detected in 2/134 (1.5%) operator samples, with the HPV subtypes detected matching those in the corresponding clinical samples. The two instances of post-treatment HPV-positive samples occurred in operators who had worn standard surgical masks, though standard surgical masks had been worn for the majority of procedures. This study also set out to determine whether HPV DNA persisted in the nasopharynx of the operators. The two operators in whom HPV DNA was detected immediately post-treatment underwent follow-up sampling at 3, 6, 12, 18 and 24 months, and clinical surveillance for HPV-related disease in the nasopharynx for approximately 3–3.5 years. One operator tested negative for the HPV subtype previously detected on initial follow-up at 3 months and thereafter, and the second operator tested negative for the HPV subtype previously detected at 6 months and thereafter. It is not stated whether the second operator had detectable HPV at 3 months. Neither operator developed clinically overt HPV-related disease during the subsequent clinical surveillance period.
Prevalence of HPV or HPV-related disease in medical personnel exposed to surgical smoke
Three studies attempted to establish the prevalence of HPV-related disease in operators exposed to surgical smoke, primarily CO2 laser users.46–48 These studies are summarised in table 4.
Studies comparing the prevalence of HPV infection or HPV-related disease between medical personnel exposed to surgical smoke and non-exposed controls
Lobraico et al conducted a questionnaire-based study asking laser users to detail the type of laser they used, the number of years performing laser procedures, the presence or absence of HPV-related lesions, and the anatomical location of any lesions.46 Of the 824/4500 (18%) questionnaire responses obtained, lesions were reported by 26/824 (3.2%) respondents, though only 4/26 (15%) lesions were histologically confirmed as compatible with HPV, and detection of HPV DNA within lesions was not enquired about. The main procedure performed by respondents was CO2 laser ablation of verrucae. When related to the duration of surgical smoke exposure, 6/26 (23%) lesions were reported by those with ≤5 years of laser practice and 20/26 (77%) of lesions were reported by those with >5 years of laser practice. Of 24, 17 (71%) of reported lesions were on the hands, with no reported lesions in the mouth or upper airways. Protective measures used by respondents reporting lesions was purportedly enquired about, though these findings are not mentioned in the results of this study.
A second questionnaire-based study was conducted by Gloster and Roenigk with similar questions.47 In this study, a comparison was made between the prevalence of warts in laser users and the general regional population, and also between the anatomical location of warts in laser users and in a patient clinic population being treated for warts. Of the 570/4200 (14%) questionnaire responses obtained, 31/570 (5.4%) respondents reported warts that they believed were due to surgical smoke exposure. No significance difference was found between overall prevalence of warts reported by laser users (5.4%) and overall prevalence of warts in the general regional population (4.9%). However, when a comparison was made between the anatomical sites of the warts reported by laser users and those in a patient clinic population being treated for warts, it was found that laser users had a significantly higher prevalence of nasopharyngeal warts (4/31, 13%) compared with the clinic population (37/6124, 0.6%). This was in contrast to plantar and genital/perianal warts, which had a significantly higher prevalence in the patient clinic population. This study also attempted to correlate the presence of warts reported by laser users with PPE and smoke removal measures reportedly used, but no difference was found between laser users with warts and those without warts on the basis of failure to use PPE or smoke evacuators. Use of N95 particulate respirators was not specifically assessed. Additionally, the prevalence of warts in laser users was not found to increase significantly with the number of years the operator had been performing laser procedures (ie, the duration of surgical smoke exposure).
The most recent study, by Kofoed et al, assessed HPV prevalence more objectively by testing oral rinse and nasal samples for the presence of HPV DNA using PCR.48 A comparison was made between medical personnel performing smoke-generating procedures and medical personnel not performing such procedures. Of the 287 medical personnel participating in the study, no significant difference was found between HPV positivity rates in participants who had performed CO2 laser treatment and electrosurgical treatment of genital warts, or LEEP of cervical dysplasia, and those who had no such experience of these procedures. However, it was found that CO2 laser users who had been performing laser ablations of genital warts for ≥5 years had a significantly higher rate of HPV positivity than those who had <5 years or no laser experience. Overall use of local smoke evacuation and laser masks was reported for CO2 laser users (88% and 79%, respectively), though no attempt was not made to correlate HPV positivity rates with PPE or smoke extraction measures used.
Discussion
Surgical smoke is generated by a large number of surgical procedures,5 41 and poses a risk to OT staff for a variety of reasons.6 The American Occupational Safety and Health Administration has estimated that each year half a million workers are exposed to surgical smoke.6 7 These numbers indicate that surgical smoke represents a significant occupational health issue on a global scale, and should be addressed seriously at departmental, institutional and national levels. As the number of surgical smoke-generating procedures for the treatment of HPV-related disease increases, so too does the theoretical risk of HPV transmission to OT staff through surgical smoke exposure.
The presence of HPV DNA in surgical smoke was a generally consistent finding in a majority of multiple acceptable studies (RCGP evidence rating ***), with several studies detecting HPV DNA in surgical smoke generated from treatment of HPV-related lesions, and the HPV subtypes present in smoke generally matching those in the corresponding clinical samples. However, there was limited scientific evidence that HPV DNA is dispersed onto treatment fields and the wider OT environment (evidence rating *).
HPV contamination of medical personnel exposed to surgical smoke was an inconsistent finding in some of multiple acceptable studies (evidence rating **). Study methodology was heterogeneous, with a variety of operator sites sampled and two different smoke-generating procedures studied (LEEP and CO2 laser ablation). Findings from one type of procedure are not necessarily generalisable to other procedures, and only upper airway samples would have utility in establishing the risk of HPV transmission via an inhalational/respiratory route. Two of the five studies looking at operator contamination demonstrated HPV DNA in operators’ upper airways following exposure to surgical smoke.41 43 In neither of these studies was a combination of general room ventilation and local exhaust ventilation (smoke extraction) used as recommended by the US National Institute for Occupational Safety and Health (NIOSH).49 Indeed, use of general room ventilation, local smoke extraction, and PPE was variably described, with only one study utilising N95 particulate respirators.28 In this study, the two surgeons with postoperative HPV-positive nasal samples wore standard surgical masks rather than N95 particulate respirators, though the significance of this finding is unclear given that standard surgical masks had been worn for the majority of procedures in the study (70%). In these two surgeons, HPV was not detected at 3–6 month follow-up.
There was limited scientific evidence for increased prevalence of HPV or HPV-related disease in OT staff following exposure to surgical smoke (evidence rating *). Two of the three included studies were retrospective and questionnaire based, and did not use any confirmatory testing to verify reported lesions as being HPV related.46 47 Only one of these studies, undertaken over 20 years ago, found a significantly higher prevalence of nasopharyngeal warts in laser surgeons compared with a clinic population being treated for warts.47 However, comparing the anatomical distribution of warts between these groups may be misleading, since patients with nasopharyngeal warts may be managed in more specialist clinics, such as otorhinolaryngology (ear, nose and throat) clinics, rather than in general wart clinics. Additionally, smoke extraction measures and PPE used by the 31 laser surgeons reporting warts in this study were not described. The most recent study, from 2015, found no significant difference in HPV-positivity in oral and nasal samples between medical personnel performing smoke-generating procedures and those not performing such procedures.48 This study did find that CO2 laser users with ≥5 years experience had higher HPV positivity rates than those with <5 years or no experience, though greater years performing smoke generating procedures does not equate to greater number of procedures actually performed, and this finding could have been influenced by age or use of PPE and smoke extraction measures.
To date, there have only been four reported cases of surgeons or other OT staff developing HPV-associated upper airway pathology following surgical smoke exposure (two cases of laryngeal papillomatosis and two cases of oropharyngeal squamous cell carcinoma).50–52 These cases occurred after working in poorly ventilated operating environments for prolonged periods, in the absence of any safety measures. They point towards an association between surgical smoke exposure and the development of HPV-related disease but are not evidence of causality as other risk factors cannot be excluded.
Whether HPV DNA in surgical smoke corresponds to the presence of infectious virus, and whether transmission of HPV can occur following inhalation of surgical smoke remains unproven. Transmission of viable papillomaviruses from surgical smoke has been demonstrated in vivo using animal papillomavirus models.53 54 These studies used a subcutaneous/intradermal route to transmit animal papillomaviruses from surgical smoke, and thus do not indicate whether viable HPVs can be transmitted through an inhalational/respiratory route. Given this uncertainty, and the presence of HPV DNA in surgical smoke, it would be prudent to assume that surgical smoke from the treatment of HPV-related lesions is potentially infectious. Accordingly, all reasonable measures should be taken to minimise OT staff exposure to surgical smoke from such procedures. These precautions should ideally include a triple combination of: (1) local exhaust ventilation (smoke extraction) to extract the majority of surgical smoke as efficiently as possible; (2) general room ventilation to remove any residual smoke in the OT atmosphere not captured by the local smoke evacuator and (3) full PPE including a fit tested particulate respirator of at least N95 grade. Points (1) and (2) are recommended by the NIOSH guidelines,49 which specify that local exhaust ventilation should ideally comprise a high efficiency particulate air-filtered smoke evacuator with sufficient capture velocity sited in close proximity to the smoke source (2–5 cm/2 inches), and that smoke evacuators should be well maintained, active at all times during smoke-generating procedures, and parts replaced following each procedure and disposed of as infectious waste.49 Full PPE should prevent surgical smoke from coming into contact with the clothes, skin, eyes and mucous membranes of the wearer. In addition to an N95 particulate respirator, full PPE should include gloves, gowns and eye protection.6 With a diameter of 55 nm,55 HPV virions correspond to the most penetrating particle size (MPPS) for N95 particulate respirators, which is approximately 30–60 nm.56 57 This means that a properly fitted N95 particulate respirator should filter at least 95% of HPV virions contained within surgical smoke. Particles which are smaller than the MPPS (such as fragments of HPV DNA) or larger than the MPPS (such as HPV virions associated with larger particles present in smoke) will be filtered with greater efficiency.58 For these reasons, when used properly, N95 particulate respirators are likely to significantly decrease human exposure to HPV in surgical smoke.59
This review has several limitations. The search strategy used was informed by previous reviews regarding terminology for surgical smoke and common surgical smoke generating procedures/devices, and this list may not be exhaustive. As with any systematic review, publication bias will affect the conclusions drawn, and this will be more pronounced when there are fewer published relevant studies, as in the present review. A major limitation lies in the methodologies of the included studies which aimed to detect HPV in a variety of settings. Included studies detected different selections of HPV subtypes, did not mention the limit of detection of the assays used, and the majority were undertaken over 20 years ago. As such, the methodology employed may not be considered acceptable by contemporary laboratory standards, and it is thus unclear whether the proportion of samples in which HPV DNA was detected accurately reflects the presence of HPV DNA in surgical smoke: contamination or assay insensitivity may lead to overdetection and underdetection, respectively. Finally the strength of evidence and conclusions drawn from studies with human participants was moderate to low. However limited evidence is not the same as no evidence, and we feel that this review accurately reports what is currently known regarding the risk to OT staff of HPV transmission and HPV-related disease following surgical smoke exposure.
Conclusions
It is now known that surgical smoke generated from the treatment of HPV-related lesions can contain HPV DNA, and that this DNA can contaminate the upper airways of OT staff. It is not known whether such smoke contains inactivated viral DNA or viable HPV capable of infecting those it comes into contact with. It would be safest to assume the latter was the case, and take necessary precautions when performing smoke-generating procedures consisting of: (1) local exhaust ventilation; (2) general room ventilation and (3) full PPE including a fit tested particulate respirator of at least N95 grade.
Increased prevalence of HPV or HPV-related disease in medical personnel exposed to surgical smoke has not been convincingly shown, and thus there is insufficient evidence at present to recommend HPV vaccination in OT staff, or to state that the combined safety measures recommended above, when used properly, would not be sufficient to prevent HPV transmission from surgical smoke.
As the utility of smoke-generating surgical procedures increases, so too does the field of surgical smoke science. More research, particularly in the form of prospective studies, is needed to clarify the risk of HPV-transmission to OT staff following exposure to surgical smoke, to quantify how this risk varies between the various smoke-generating procedures used, and to establish if any risk remains when recommended safety precautions are adhered to.
Acknowledgments
The authors are very grateful to Anne Wilson and Selina Foote at Auckland University Library Services for their assistance in systematic literature searching and location of full-text articles, respectively, and to Meik Dilcher at Canterbury Health Laboratories for his assistance in article translation.
References
Footnotes
Contributors AF-L conceived the work and conducted the literature search. AF-L and CA screened search results for inclusion, and SR resolved any disagreement. All authors contributed to the qualitative results synthesis, prepared the first draft of the manuscript and approved the final manuscript.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent for publication Not required.
Provenance and peer review Not commissioned; externally peer reviewed.