Article Text

Abstract
Objectives Asbestos is the main risk factor for peritoneal mesothelioma (PeM). However, due to its rarity, PeM has rarely been investigated in community-based studies. We examined the association between asbestos exposure and PeM risk in a general population in Lombardy, Italy.
Methods From the regional mesothelioma registry, we selected PeM cases diagnosed in 2000–2015. Population controls (matched by area, gender and age) came from two case–control studies in Lombardy on lung cancer (2002–2004) and pleural mesothelioma (2014). Assessment of exposure to asbestos was performed through a quantitative job-exposure matrix (SYN-JEM) and expert evaluation based on a standardised questionnaire. We calculated period-specific and gender-specific OR and 90% CI using conditional logistic regression adjusted for age, province of residence and education.
Results We selected 68 cases and 2116 controls (2000–2007) and 159 cases and 205 controls (2008–2015). The ORs for ever asbestos exposure (expert-based, 2008–2015 only) were 5.78 (90% CI 3.03 to 11.0) in men and 8.00 (2.56 to 25.0) in women; the ORs for definite occupational exposure were 12.3 (5.62 to 26.7) in men and 14.3 (3.16 to 65.0) in women. The ORs for ever versus never occupational asbestos exposure based on SYN-JEM (both periods) were 2.05 (90% CI 1.39 to 3.01) in men and 1.62 (0.79 to 3.27) in women. In men, clear positive associations were found for duration, cumulative exposure (OR 1.33 (1.19 to 1.48) per fibres/mL-years) and latency.
Conclusions Using two different methods of exposure assessment we provided evidence of a clear association between asbestos exposure and PeM risk in the general population.
- asbestos
- mesothelioma
- peritoneum
- population–based case–control study
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Key messages
What is already known about this subject?
Cohort studies in highly exposed workers showed that peritoneal mesothelioma (PeM) is associated with asbestos exposure.
However, this disease has rarely been investigated in community-based studies.
What are the new findings?
For the first time using a population-based case–control study, we provided further evidence of the association between PeM and asbestos exposure evaluated either with expert-based assessment or with a quantitative job-exposure matrix.
The latter also allowed quantification of the association with cumulative asbestos exposure.
How might this impact on policy or clinical practice in the foreseeable future?
These results may be of relevance for compensation of asbestos victims.
The quantitative job-exposure matrix proved to be a valuable tool to study asbestos-related diseases in a community.
Introduction
Peritoneal mesothelioma (PeM) represents a minority (<10%) of malignant mesotheliomas (MM). In the RARECARE project, based on data from 21 countries, the crude incidence rate of PeM in the period 1995–2002 was 0.12 per 100 000 person-years.1
The main risk factor for MM is asbestos (all forms).2 The epidemiology of PeM shows some differences compared with pleural mesothelioma, including a lower attributable risk of asbestos exposure,3 4 a lower male/female ratio5–8 and less definite temporal trends of PeM rates.4–6 Moreover, cohort studies showed a continuous increasing PeM risk with time since first exposure, while a plateauing was found for pleural mesothelioma.8–10 While cohort studies in high-risk industries have shown a definite excess of PeM among asbestos-exposed workers,3 11 few case–control studies on PeM have investigated this association in a general population setting.12–15
Italy was one of the main producers of chrysotile in Europe and a large consumer of all types of asbestos until the ban in 1992. In the years 1993–2004, 614 cases (362 men, 252 women) of PeM were recorded by the national MM registry (Registro Nazionale Mesoteliomi, ReNaM), and the age-standardised incidence rates in 2004 (standard: Italian population 2001) were 0.21 per 100 000 in men and 0.12 in women.16 In 2008, the rates were 0.26 and 0.12 per 100 000.6 As of 2012, the number of PeM recorded was 1392 (6.5% of all mesotheliomas, 817 in men, 575 in women).7
In Lombardy, North-Western Italy, the most populated (currently, 10 million people) and industrialised Italian region, a regional MM registry (Registro Mesoteliomi Lombardia, RML) was implemented in 2000. A high impact of asbestos exposure on MM occurrence has been shown in Lombardy.17–19 Comparing peritoneal and pleural mesothelioma characteristics, we recently found similar frequencies of asbestos exposure but higher proportions of asbestosis and exposure in the asbestos-cement industry among PeM cases.20
In this study, we examined the association between asbestos exposure and PeM in the general population using a case–control design, with cases extracted from the RML database (2000–2015) and using two sets of population controls recruited in Lombardy in earlier case–control studies,21 one on lung cancer (2002–2004) and one on pleural mesothelioma (2014).
Methods
The Lombardy Mesothelioma Registry (RML)
The Lombardy Mesothelioma Registry (RML) collects clinical information on newly diagnosed MM cases among Lombardy residents from regional and extra-regional hospitals. Diagnosis is evaluated on individual basis after revision of clinical records by two experts working in the registry since its implementation (CM and LR). Following ReNaM guidelines, confirmed cases are classified as ‘definite’ (histological diagnosis, possibly with immunohistochemical confirmation), ‘probable’ (usually, cytology plus imaging) or ‘possible’ (positive imaging).22 Completeness of reporting (compulsory by law) is periodically verified using various sources, including hospital admission databases.
Cases with confirmed MM or their next-of-kin are interviewed by trained personnel using a standardised ReNaM questionnaire covering life-time job-history (including industry, occupation and details about tasks or indirect exposure within each jobs) and also various sources of extra-occupational asbestos exposure, including familial or para-occupational (from a cohabitant’s contaminated clothes); domestic or home-related (eg, ironing on asbestos boards; installation, repair or removal of asbestos containing materials); environmental (mostly residence near an asbestos-cement factory).18 19 22 Then, following ReNaM guidelines, lifetime asbestos exposure is evaluated by experts (CM and LR) and finally classified as ‘occupational’ (definite, probable, possible) or (only for non-occupationally exposed cases) ‘extra-occupational’.22
Cases
From the RML database, we extracted all incident PeM cases in the period 2000–2015. To approximately match the study base, represented by the two series of controls,23 we created two sets of cases, the first (2000–2007) including cases residing in five provinces (Milan, Monza, Brescia, Pavia and Varese) aged 35–79 years, and the second (2008–2015) comprising cases aged 20–89 years living in any province.
Controls
The first set of controls (figure 1) came from the Environment And Genetics in Lung cancer Etiology (EAGLE) population-based case–control study on lung cancer.24 Controls (frequency matched to cases by area of residence, gender and age) had been randomly sampled in 2002–2004 among 1 642 074 residents aged 35–79 years in 216 municipalities out of 725 (3 462 808 residents) in five Lombardy provinces (Milan, Monza, Brescia, Pavia and Varese). The participation rate (participants/eligible) was 72.4%. Subjects underwent a computer assisted personal interview (https://eagle.cancer.gov/questionnaires.html), which investigated lifetime occupational history (years of start/stop, industries, occupations) for jobs held for 6+ months.25 26
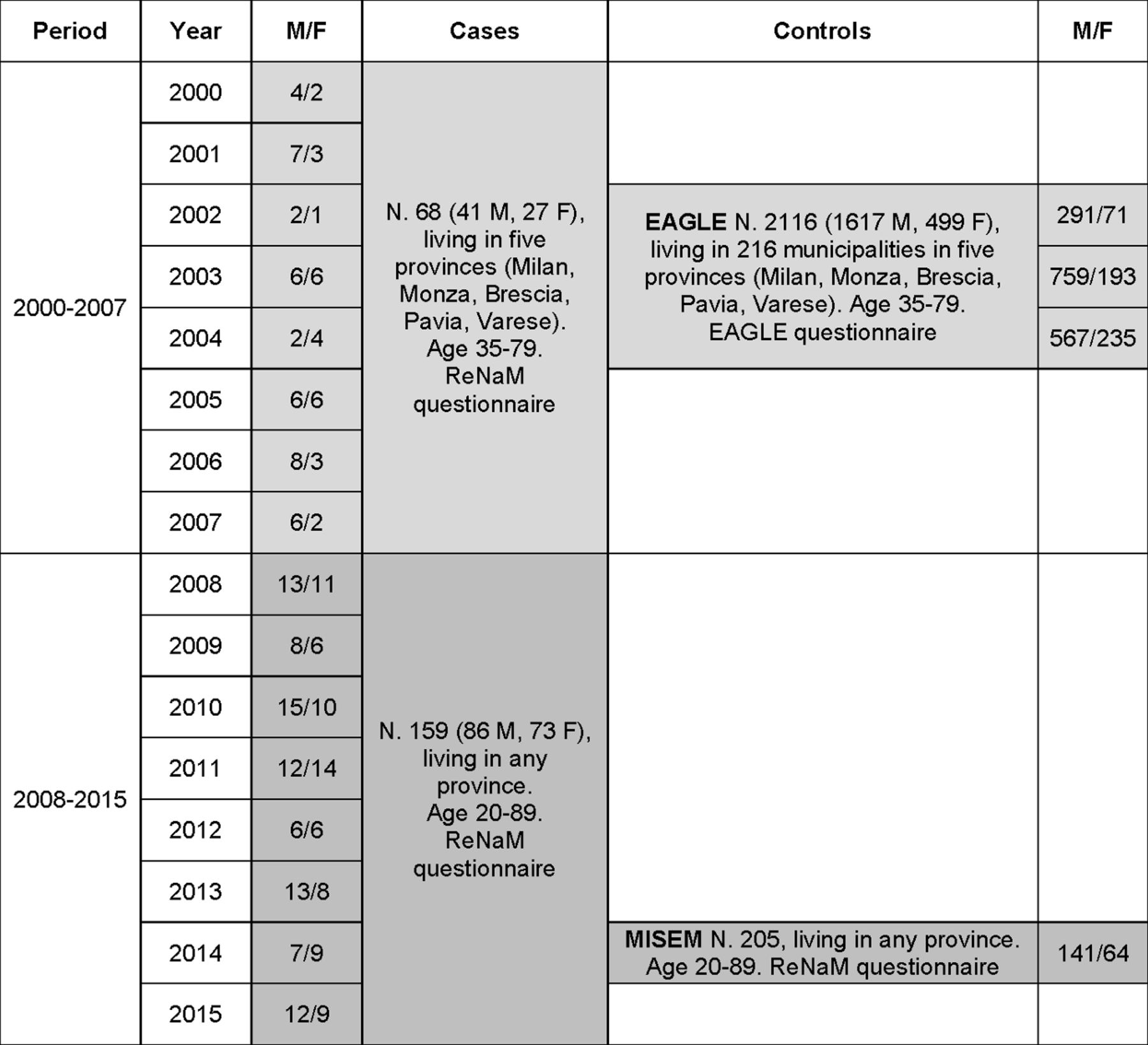
Diagram showing numbers of male (M) and female (F) peritoneal mesothelioma cases and controls across the years and their main characteristics, Lombardy, Italy, 2000–2015. ReNaM, Registro Nazionale Mesoteliomi.
The second set of Lombardy controls (figure 1) was taken from a multicentre population-based case–control study on pleural mesothelioma (MISEM, unpublished), performed in five regions including Lombardy, where controls (frequency matched to cases by province of residence, gender and age) had been randomly sampled from residents in any province aged 20–89 years in 2014 and interviewed in 2015 using the same ReNaM questionnaire of cases. Participation rate was 48.1%.
Assessment of occupational exposure to asbestos
We used two methods of exposure assessment, one based on expert evaluation of the ReNaM questionnaire, the other on a job-exposure matrix (JEM).
For cases and MISEM controls (2008–2015), we classified asbestos exposure according to non-blind expert evaluation based on the ReNaM questionnaire. We used four categories: never-exposed, extra-occupational, occupational probable/possible and definite occupational exposure.
For all subjects (cases, EAGLE and MISEM controls, 2000–2015), industries and job titles were coded following the International Standard Industrial Classification of All Economic Activities (ISIC, 1971) and the International Standard Classification of Occupations (ISCO, 1968).25 26 Within EAGLE, coding was supervised by two of us (DC, SDM). For cases and MISEM controls, coding was performed/checked by three of us (CM, DM, DC). Coding was blind for disease status in EAGLE and MISEM, while it was non-blind for PeM cases. ISCO-68 codes were linked to a quantitative JEM (SYN-JEM), developed and used within the SYNERGY project on lung cancer,27–29 to get yearly intensities of exposure in fibres (ff) per mL in each job, from which we calculated individual lifetime cumulative exposure to asbestos (ff/mL-years).
Statistical analysis
We performed analyses for asbestos exposure, as defined according to (1) an expert-based evaluation based on information provided by the ReNaM questionnaire (only available for MISEM controls, 2008–2015); and (2) SYN-JEM, available for both periods (2000–2007 and 2008–2015), and both sets of controls. To avoid sparse data problems, we fitted period-specific and gender-specific conditional (instead of unconditional) regression models using age categories (<50, 50–59, 60–64, 65–69, 70–74 and 75+ years) as the adjustment set to calculate OR and CI.30 To address potential residual confounding by age, we included among covariates the age deviations from midpoint age categories.31 We calculated 90% CIs in order to avoid a reductive interpretation of CIs as significance tests.32–34
All models were additionally adjusted for province of residence (five provinces for cases and EAGLE controls in 2000–2007, 12 provinces for cases and MISEM controls in 2008–2015). Since education (a proxy for socioeconomic status) may be related to control participation, we always included education among the covariates.35 Because there were missing education data for cases and MISEM controls, using a multinomial model we generated 50 samples by imputing values based on case status, gender, age (continuous) and blue collar job (ever/never).
Cumulative exposure (from SYN-JEM) was either categorised in four categories (non-exposed and three categories based on tertiles calculated among exposed cases) or analysed as a continuous variable and its natural logarithm.
For ever-exposure to asbestos, we calculated the population attributable fraction (PAF=PEC(OR–1)/OR, where OR is adjusted and PEC is the proportion of exposed cases).23
We performed sensitivity analyses by including only cases with definite diagnosis or with direct interview (ie, exclusion of next-of-kin interviews) and excluding job periods after 1992 (year of asbestos ban in Italy). Given the incomplete spatiotemporal overlap between cases and controls, we performed further analyses by applying the following restrictions to cases: diagnosed in 2000–2007 living in the same 216 municipalities as EAGLE controls (SYN-JEM, spatial restriction); diagnosed in 2000–2004 or in 2010–2014 (expert-based assessment and SYN-JEM, temporal restriction); diagnosed in 2000–2004 living in the same 216 municipalities as EAGLE controls or in 2010–2014 (SYN-JEM, spatiotemporal restriction). Statistical analyses were performed with Stata V.15.36
Results
In the years 2000–2015, the RML recorded 325 subjects with PeM (170 men, 155 women). The corresponding crude incidence rates were 0.23 and 0.20 per 100 000 person-years.
In the period 2000–2007, there were 77 male and 70 female cases. After selection of residents in the five provinces aged 35–79 years, cases decreased to 42 and 31, respectively. We further excluded one man and four women without interview, leaving 68 cases (41 men, 27 women) for the analyses (figure 1 and table 1, upper half). From 2120 EAGLE controls (1620 men, 500 women), we included 2116 with interview (1617 men, 499 women). Mean ages ranged from 64.1 to 66.2 years and there was good overlap for age adjustment. The proportion of PeM cases directly interviewed was <50%. Education level was higher in EAGLE controls. Most PeM cases in both genders (>80%) had ever been employed in blue collar jobs. The majority of cases had a definite mesothelioma diagnosis. The most frequent histological type was epithelioid.
Characteristics of peritoneal mesothelioma cases and controls, Lombardy, Italy, 2000–2015
In the period 2008–2015, there were 178 cases (93 men, 85 women). We excluded 3 women aged 90+ years and 7 men and 9 women without interview, leaving 159 cases (86 men, 73 women) for the analyses (figure 1 and table 1, lower half). MISEM controls were 205 (141 men, 64 women), all interviewed. Mean ages ranged from 68.0 to 69.9 years, again with good overlap. The proportion of patients interviewed was 61.6% in men and 51.3% in women. Education was higher among MISEM controls. In PeM cases, blue collar jobs were reported by 83.7% of men and 52.1% of women. The proportion of definite diagnoses was almost 90% in both genders. Epithelioid mesothelioma was the most frequent histological type.
In the period 2008–2015, using MISEM controls and according to exposure evaluation by experts based on the ReNaM questionnaire (table 2), in men we found an OR of 5.78, based on 64 ever exposed cases (74.4%), corresponding to a PAF of 0.62. The OR was 12.3 for definite occupational exposure and there were clear increasing trends with duration of exposure and time since first exposure. In women, there was an OR of 8.00 based on 26 (36.6%) ever exposed cases (PAF 0.32), and an OR of 14.3 for definite occupational exposure. There were positive, although irregular, trends of risk for duration and time since first exposure. In both genders, a twofold elevated OR was calculated for probable/possible occupational exposure while in men ORs were elevated also for extra-occupational exposures to asbestos (based on few exposed cases).
Peritoneal mesothelioma OR and 90% CI for expert-based assessment of asbestos exposure based on the national mesothelioma registry (ReNaM) questionnaire, calculated with conditional logistic regression models (set: age category), adjusted for province of residence, education and residual age within age category, Lombardy, Italy, 2008–2015
Proportions of ever exposed male controls according to the SYN-JEM were remarkably similar in the two periods, 503/1617=31.1% in EAGLE and 47/141=33.3% in MISEM (online supplementary tables 1-2). Moreover, among EAGLE controls the proportions of ever exposed men was constant over the years: 101/291=34.7% (2002), 230/759=30.3% (2003) and 172/567=30.3% (2004) (p value: 0.34). In women, proportions of exposed controls were 50/499=10.0% in EAGLE and 3/64=4.7% among MISEM controls (online supplementary tables 1-2). Among women, EAGLE controls proportions of ever exposed were 4/71=5.6% (2002), 24/193=12.4% (2003) and 22/235=9.4% (2004) (p value: 0.24).
Supplementary file 1
In analysing occupational asbestos exposure estimates from SYN-JEM, patterns of ORs were similar either using EAGLE or MISEM controls (online supplementary tables 1-2) and there was no suggestion of period-exposure interactions. Therefore, we combined the two periods (table 3). In men, we found an OR of 2.05 based on 72 ever exposed cases (56.7%), corresponding to a PAF of 0.29, and positive trends by duration and cumulative exposure, for which we estimated ORs of 1.33 per ff/mL-years and 2.15 per ln(ff/mL-years) (figure 2). The OR continued to increase with increasing time since first exposure. In women, the number of ever exposed cases was 17 (17.0%), with an OR of 1.62 (PAF 0.07) and no clear patterns by duration, cumulative exposure and latency.

{kind=link}
{kind=link}
Association between peritoneal mesothelioma risk and cumulative asbestos exposure (ff/mL-years) in men using restricted cubic splines (knots at 10th, 25th, 50th, 75th and 90th percentiles of cumulative exposure among exposed, log-transformed), Lombardy, Italy, 2000–2015.The dashed line shows the log-linear relationship OR=2.15 per ln(ff/mL-years) (see table 3); vertical bars close to the horizontal axis indicate cases (upper bars) and controls (lower bars).
Peritoneal mesothelioma OR and 90% CI for occupational asbestos exposure from the job-exposure matrix (SYN-JEM), calculated with conditional logistic regression models (set: age category), adjusted for period (2000–2007 and 2008–2015), province of residence, education and residual age within age category, Lombardy, Italy, 2000–2015
Either for expert-based or SYN-JEM exposure assessment, results were similar when analyses were restricted to definite cases (results not shown), directly interviewed subjects (online supplementary tables 3-4), and when jobs periods after 1992 were excluded (results not shown).
The OR patterns according to SYN-JEM exposure assessment were confirmed when in the period 2000–2007 we included only cases living in the same 216 municipalities of EAGLE controls (spatial restriction, online supplementary table 5 and figure 1). Results were basically unchanged also in the other sensitivity analyses in which temporal (online supplementary tables 6-7 and figure 2) or spatiotemporal (online supplementary table 8 and figure 3) restrictions were applied to cases.
Discussion
Our study showed positive associations between PeM in men and asbestos exposure evaluated either with expert-based assessment based on an asbestos-specific standardised questionnaire used by the Italian mesothelioma registry (ReNaM) or with a quantitative JEM. In particular, PeM risk increased with increasing cumulative exposure (calculated with the SYN-JEM) and ORs were strongly elevated in the period 2008–2015 (MISEM controls), when asbestos exposure was assigned by experts. Among women, there were suggestive positive associations when using the JEM, but few subjects were classified as exposed, while clear excess risks were found with the expert-based assessment.
Comparison with published research
We found four case–control studies on PeM and asbestos exposure. The first one, hospital-based, was performed in the London area including 56 pleural and 27 peritoneal MM, but results were only presented for both sites combined.14
A second study using dead controls was performed in the USA (Los Angeles County, with a large shipyard industry, New York State, and 39 large Veterans Administrations hospitals, 1975–1980).13 Next-of-kin were interviewed by telephone and exposure was evaluated with different methods, including a direct question about ever asbestos exposure, having worked in nine prespecified high-risk occupations, and a JEM which classified likelihood of exposure (none, 10%–19%, 20%–49% or 50%+) in each job. Similar to us, they observed that ORs differed by exposure assessment method. Based on 20 PeM cases in men (17 exposed) and an overall OR of 3.1 (all exposures combined), the attributable risk (PAF) was 58.1%. The ORs were 10.6 for the direct question on ever asbestos exposure (PAF 63.5%), 3.0 for high-risk occupations (PAF 43.9%), and, using the JEM, 4.0 for <20% likelihood of exposure (PAF 26.1%) and 4.2 for 20+ likelihood (PAF 14.7%).
The third study applied an asbestos JEM (in which combined scores of probability/intensity of exposure were categorised as none, low, medium and high) to 657 deaths from PeM and 6570 controls who died from non-malignant diseases in 24 US states (1984–1992).12 Positive associations between PeM and selected occupations were found for both genders. Among men, elevated ORs were found for high probability (OR 61.6, 17 cases exposed) and high intensity of exposure (OR 4.8, 22 cases exposed). The highest ORs were found for high-exposure groups, including insulators (OR 180, 17 cases exposed) and asbestos-cement workers (OR 7.6, 5 cases exposed). Less clear patterns were observed in women.
The fourth was a hospital-based study including 24 male PeM cases and 24 controls with appendiceal cancer (Washington Cancer Institute, 1989–2001).15 Subjects underwent a telephone interview using the same questionnaire of the second study quoted above.13 The OR for any asbestos exposure was 6.6 (22 cases exposed). The ORs were 2.0 for the direct question on ever asbestos exposure, 5.0 for nine high-risk occupations, and 11.7 according to expert evaluation (ORs recalculated by us from table 1 of the paper because of inconsistencies between tables and text). Those results (higher ORs with expert-based assessment) are consistent with ours.
In cohort studies, a strong correlation has been reported between proportions of PeM and pleural mesothelioma deaths, with PeM proportions particularly high among highly exposed subjects (insulators, asbestos-cement workers and asbestosis patients).3 Recent cohort studies showed continuously increasing relative risks by latency for PeM, while an attenuation of the increase was found for pleural mesothelioma.8–10 Our findings are consistent with those results.
Strength and limitations
The present study has several strengths. First, it is, to our knowledge, the first case–control study on PeM with controls sampled from the general population. Second, it was based on a virtually complete series of cases with good quality diagnosis. In fact, Lombardy has a network of high-quality hospitals, so the majority of PeM cases were confirmed by immunochemistry, histology or cytology. All relevant clinical information was reviewed before inclusion of cases into the registry. RML completeness and quality have been confirmed by comparison with cancer registries.37 In any case, key findings were confirmed after restricting analyses to definite cases. Third, interview rate of cases was very high (>90%), although, given the low survival of the disease, the ReNaM questionnaire could be administered to patients in only about half of cases (for very ill and deceased subjects the next-of-kin is interviewed). Moreover, results were confirmed among directly interviewed subjects. Fourth, the case–control design allowed us to evaluate PeM risk associated with asbestos exposure in all industries and occupations, not only in specific high-risk groups as in cohort studies.
The main potential limitations of this study are that populations samples (controls) had been recruited during limited time periods, 2002–2004 (EAGLE) and 2014 (MISEM), and that EAGLE controls did not cover the whole population in the five provinces. As to incomplete time coverage, we have to consider that our focus was on lifetime asbestos exposure, which we expect to have remained constant in the source population over the study period. The fact that asbestos exposure (evaluated with SYN-JEM, which depends only on occupations) was around 30% in both male control series and constant in the period 2002–2004 among EAGLE controls further supports the assumption that controls had been sampled from similar populations without evident secular exposure trends.21 Moreover, sensitivity analyses in which we applied temporal restriction to cases yielded results comparable to the main analyses. As to incomplete geographical coverage in 2000–2007, we did not expect major variations in asbestos exposure between the 216 selected and the unselected municipalities (geographically quite close); the main results were confirmed in sensitivity analysis performed after spatial restriction.
Another possible limitation is that EAGLE controls had been interviewed using a different questionnaire from that used for cases and MISEM controls. However, since the JEM-based exposure assessment depended exclusively on completeness of individual work histories and quality of job coding, the only relevant comparison between the EAGLE and ReNaM questionnaires is that involving the respective occupational history sections. The occupational sections of both questionnaires recollected full, lifetime occupational histories and had very similar structures, registering for each employment period: year of start and end, industrial activity, occupation and a short free-text job description. Coding of industry and occupation was therefore based on the same quality of information, irrespective of whether provided by the EAGLE or the ReNaM questionnaire.
One further limit was the low participation of MISEM controls (48.1%), which could have resulted in a lower representation of blue collar workers. To address the potential selection bias resulting from differential participation, regression models were adjusted for education, a proxy for socioeconomic status.35
In most if not all applications in Italy both chrysotile and amphiboles have been used at the same time. Therefore, it was not possible to discriminate between exposure to either type of asbestos.
Comparison of results obtained with JEM and expert-based assessment
SYN-JEM exposure assessment, being based on job titles, is expected to have lower sensitivity and specificity than the ReNaM questionnaire, which investigates each job in detail and can take into account specific tasks and working conditions. Considering subjects evaluated with both tools (cases and MISEM controls, 2008–2015), and taking ReNaM as reference, overall sensitivity of SYN-JEM was 0.61 (90% CI 0.54 to 0.67) and specificity 0.88 (90% CI 0.84 to 0.91). Indeed, SYN-JEM has been created privileging specificity.27 Sensitivity was higher in men, specificity in women. The overall Cohen’s kappa was 0.51 (90% CI 0.43 to 0.58), with agreement higher among men (online supplementary table 9).
Although expert assessment can a priori be considered more accurate, we have to consider the possibility of recall, interviewer and assessor biases (because assessment for cases was non-blinded), which could result in an OR biased away from the null. The SYN-JEM has three main advantages over expert assessment. First, being based only on job titles, it is not affected by recall and interviewer biases.38–40 Second, it is much less time-consuming. Third, it allows quantitative analyses. On the other hand, there may be OR underestimation due to non-differential exposure misclassification (because of lower accuracy and possible errors in coding occupations).
Asbestos exposure in this study was much more frequent among men than among women using both exposure assessment methods. This finding is not restricted to PeM, being shared by pleural mesothelioma, either in Lombardy or in Italy.7 20
Conclusions
In this first population-based case–control study on PeM, we found clear associations between PeM risk and several indices of asbestos exposure (probability, duration and cumulative exposure) among men. Notably, findings were consistent using two different methods to assess lifetime asbestos exposure. In agreement with cohort studies, relative risks in men showed a continuous increase with time since first exposure. In women, clearly increased risks were found only when exposure assessment was based on the standardised questionnaire used by the Italian mesothelioma registry, most likely due to their low prevalence of asbestos exposure.
Acknowledgments
The authors wish to thank the personnel of the regional hospital Occupational Health Departments (UOOML) and of the Occupational Prevention and Safety Departments of the Local Health Units (SPSAL) for their collaboration in notifying and interviewing subjects affected by mesothelioma; the personnel of the Medical, Surgical and Pathology Departments of regional hospitals for their collaboration in providing clinical documentation; Luana Garlati, Lombardy Mesothelioma Registry, for her valuable secretarial assistance; the subjects affected by mesothelioma and their family members for granting interviews; the personnel of SELEXI for performing MISEM interviews. Lützen Portengen (
Institute for Risk Assessment Sciences, Utrecht University
) linked the SYN-JEM to the job histories of cases and controls.
Cristina Calvi contributed to this work while attending the
Master in Epidemiology, Università degli Studi di Torino, Turin, Italy.
References
Footnotes
Contributors DC: study design, statistical analysis, supervision of data collection and manuscript drafting; CC: manuscript drafting. SDM: statistical analysis (EAGLE study). DM: scientific coordinator, study design and supervision of data collection (MISEM study). MTL and NEC: principal investigators and study design (EAGLE study). SP, RV and HK: job-exposure matrix creation and creation. BD and LR: data collection (cases). ACP: study design and supervision of data collection (EAGLE study). CM: study design, data collection (cases) and supervision of data collection (MISEM controls). All authors contributed to interpretation of findings and discussion. All authors revised and approved the manuscript for intellectual content.
Funding This work was partially supported by: the Intramural Research Program of the National Institutes of Health, the National Cancer Institute, Division of Cancer Epidemiology and Genetics, Bethesda, Maryland, USA (EAGLE); Ministry of Health, CCM (Centro Nazionale per la Prevenzione e il Controllo delle Malattie), Rome, Italy (MISEM); Istituto Nazionale per l’Assicurazione contro gli Infortuni sul Lavoro (INAIL), Rome, Italy: BRiC P55 and P59; Associazione Italiana per la Ricerca sul Cancro (AIRC), Milan, Italy: IG 2015/17692.
Competing interests DC and CM served as consultants for the court in litigations concerning asbestos-related diseases. DM served as consultant for the public prosecutor in litigations concerning asbestos-related diseases.
Ethics approval As reporting of malignant mesothelioma to the National Mesothelioma Registry (ReNaM) is compulsory by law, ethics approval is not required for cases. The EAGLE and MISEM study were approved by the following institutional review boards (IRBs): National Cancer Institute Special Studies IRB: 01-C-N211, National Cancer Institute, Bethesda, Maryland, USA (EAGLE); Comitato Etico Interaziendale, AOU San Giovanni Battista di Torino and AO CTO/Maria Adelaide di Torino, Turin, Italy: CEI-589 (MISEM).
Provenance and peer review Not commissioned; externally peer reviewed.
Patient consent for publication Not required.