Article Text

Abstract
Objectives The occupational exposure limit for trichloroethylene (TCE) in different countries varies from 1 to 100 ppm as an 8-hour time-weighted average (TWA). Many countries currently use 10 ppm as the regulatory standard for occupational exposures, but the biological effects in humans at this level of exposure remain unclear. The objective of our study was to evaluate alterations in immune and renal biomarkers among workers occupationally exposed to low levels of TCE below current regulatory standards.
Methods We conducted a cross-sectional molecular epidemiology study of 80 healthy workers exposed to a wide range of TCE (ie, 0.4–229 ppm) and 96 comparable unexposed controls in China, and previously reported that TCE exposure was associated with multiple candidate biological markers related to immune function and kidney toxicity. Here, we conducted further analyses of all of the 31 biomarkers that we have measured to determine the magnitude and statistical significance of changes in the subgroup of workers (n=35) exposed to <10 ppm TCE compared with controls.
Results Six immune biomarkers (ie, CD4+ effector memory T cells, sCD27, sCD30, interleukin-10, IgG and IgM) were significantly decreased (% difference ranged from −16.0% to −72.1%) and one kidney toxicity marker (kidney injury molecule-1, KIM-1) was significantly increased (% difference: +52.5%) among workers exposed to <10 ppm compared with the control group. These associations remained noteworthy after taking into account multiple comparisons using the false discovery rate (ie, <0.20).
Conclusion Our results suggest that occupational exposure to TCE below 10 ppm as an 8-hour TWA may alter levels of key markers of immune function and kidney toxicity.
- trichloroethylene
- occupational exposure
- biomarker
- immune function
- kidney toxicity
Statistics from Altmetric.com
Key messages
What is already known about this subject?
Trichloroethylene (TCE) is considered by the International Agency for Research on Cancer to be a group 1 carcinogen based in part on epidemiological studies linking it to kidney cancer, as well as limited evidence that it is also associated with non-Hodgkin’s lymphoma.
The mechanism of action for TCE has not been identified.
Although occupational exposure to TCE has been associated with changes in various immune and renal toxicity biomarkers, these have been observed at relatively high levels of exposure.
There is little evidence about its biologic effects below current occupational standards in most countries.
What are the new findings?
Seven out of 31 immune regulation and kidney function markers that we have previously reported on from a cross-sectional biomarker study of workers exposed to a wide range of TCE were significantly decreased (CD4+ effector memory T cells, sCD27, sCD30, interleukin-10, IgG and IgM) or increased (KIM-1) among workers exposed to <10 ppm TCE, which is below the current occupational standard in many countries.
How might it impact on clinical practice in the foreseeable future?
Our results suggest that occupational exposure to TCE below existing occupational standards may alter levels of key markers of immune function and kidney toxicity and raise additional questions about the safety of current standards.
Introduction
Trichloroethylene (TCE) is an industrial solvent used in degreasing, dry cleaning and for numerous other medical and industrial processes. It is a common environmental contaminant of drinking water and is present in many Environmental Protection Agency Superfund sites.1 The International Agency for Research on Cancer (IARC) recently classified TCE as a group 1 carcinogen based on its consistent association with kidney cancer and noted that there was limited evidence for an association with non-Hodgkin’s lymphoma (NHL).2 3 Currently, there are a wide range of international occupational TCE exposure standards.4 5 The current US Occupational Safety and Health Administration (OSHA) Permissible Exposure Limit is 100 ppm as an 8-hour time-weighted average (TWA). Many countries have set the standard as 10 ppm or similar levels (ie, 9 or 11 ppm), and have started considering even lower concentrations as a permissible standard.4 For example, in response to new information relating to the health and biologic effects of TCE exposure, the American Conference of Governmental Industrial Hygienists (ACGIH) reduced its threshold limit values (TLVs) (ie, TLV-TWA and TLV-short-term exposure level [STEL]) from 50 and 100 ppm to 10 and 25 ppm, respectively, in 2007. Similarly, the Scientific Committee on Occupational Exposure Limits (SCOEL) in 2009 recommended a TWA of 10 ppm and a STEL of 30 ppm. A lower value of 6 ppm is currently the occupational exposure limit for Germany and China and 1 ppm for Austria.
We previously conducted a series of analyses within a cross-sectional molecular epidemiology study to evaluate the biologic plausibility of carcinogenicity related to occupational exposure to TCE.6–10 We reported significant exposure-response relationships between TCE exposure and levels of various immune (ie, blood cell counts, cytokines and immunoglobulins) and kidney toxicity markers. Although we observed significant trends for many of these biomarkers, we did not determine if changes in biomarker levels were present below the most common regulatory standard of 10 ppm. Here, we present new analyses on all immune regulation and kidney function markers that we have measured to date to evaluate the effect of TCE exposure at levels under 10 ppm.
Materials and methods
Study population and exposure assessment
The design, participants, environmental exposure assessment and biological sample collection for this study have been described.6 Briefly, this cross-sectional molecular epidemiological study included 80 workers currently exposed to TCE in six study factories with TCE cleaning operations and 96 unexposed controls from the same geographic area in Guangdong, China. Unexposed controls were frequency-matched to exposed workers by sex and age (±5 years) and were enrolled from two clothing manufacturing factories, one food production factory and a hospital that did not use TCE. Workers with a history of cancer, chemotherapy, radiotherapy or a previous occupation with notable exposure to benzene, butadiene, styrene and/or ionising radiation were excluded. A questionnaire-based interview was administered to all subjects to assess demographics, lifestyle characteristics and occupational history.
Personal air exposure measurements were conducted for all study subjects. Full-shift personal air exposure measurements were taken over a 3-week period before blood collection in the factories using 3M organic vapour monitoring (OVM) badges. All samples were analysed for TCE and a subset (48 from TCE-exposed workers) was analysed for a panel of organic hydrocarbons including benzene, methylene chloride, perchloroethylene and epichlorohydrin. OVM samples were also obtained on a subgroup of control workers. Current TCE air levels in part per million (ppm) were based on the arithmetic mean of an average of two to three measurements per subject. Ninety-six per cent of workers were exposed to TCE below the current US OSHA Permissible Exposure Limit (100 ppm 8-hour TWA) and 44% of workers were exposed to TCE below 10 ppm (online supplementary figure 1).
Supplementary file 1
Assays for molecular markers
Participants provided blood, buccal cell mouth rinse and postshift and overnight urine samples and underwent a physical examination. Blood samples were delivered to the laboratory within 6 hours of collection, where the complete blood count and differential and major lymphocyte subsets were analysed on the same day. Postshift urine samples were stored at 4°C until being processed within 10 hours of collection. Samples were centrifuged and 1.4 mL of urine supernatant was then mixed with 0.3 mL freezing buffer (NEPHKIT Urine Stabilising Buffer; Argutus Medical) to stabilise proteins for storage and freezing. Samples were subsequently stored at −80°C.
The laboratory methods for the evaluated biomarkers have been described in detail.6–10 A flow cytometer was used for blood cell counting. Plasma sCD27 and sCD30 were measured in duplicate by an ELISA (Bender Medsystems, Vienna, Austria). Serum concentrations of IgG, IgM and IgE were measured using an ELISA. Serum concentrations of interleukin (IL)-6, IL-10 and tumour necrosis factor-α were measured using a multiplex high-sensitivity human cytokine Milliplex (Billerica, Massachusetts, USA) assay for the BioPlex200 (BioRad, Hercules, California, USA) platform according to the manufacturer’s instructions. Postshift spot urine samples were analysed for creatinine, glutahione S-transferase alpha (α-GST), Pi-GST, vascular endothelial growth factor (VEGF), KIM-1 and N-acetyl-beta-D-glucosaminidase (NAG) concentrations. Creatinine was determined by automated Jaffé reaction.
Statistical analysis
Unadjusted means and SD are presented for all the immune regulation markers (n=26) and kidney function markers (n=5) that were evaluated for an association with TCE exposure previously. Linear regression models using the natural logarithm (ln) of each end point were used to test for differences between control and exposed workers and to evaluate for an exposure-response across TCE exposure categories using a three-level ordinal variable (ie, controls, low exposure group [<10 ppm] and high exposure group [≥10 ppm]). For each end point, we included the same covariates as in our previous reports6–10 into each model. The covariates included in the linear regression models were age (continuous), sex, current smoking (yes/no), current alcohol consumption (yes/no), recent infections (flu or respiratory infections in the previous month) and body mass index (BMI, kg/m2). The models for urinary biomarkers were additionally adjusted for log-transformed creatinine levels. We selected 10 ppm based on a literature review of standards for occupational exposure to TCE (online supplementary figure 2).4 5 11–15 As shown in the online supplementary figure 2, the occupational exposure limit for TCE in different countries or organisations with data available (n=47) varied from 1 to 100 ppm as TWA for 8 hours. While 20 countries or organisations still set a relatively high level as a standard (ie, ≥25 ppm), as many as 21 countries or organisations including the US ACGIH and EU SCOEL have suggested or adopted 10 ppm as a standard. The standard 9 or 11 ppm may be the same as 10 ppm considering that there may be deviance due to conversion (ie, µg/m3 to ppm). Even lower levels than 10 ppm were set as a standard by several countries including Austria (1 ppm), Latvia (2 ppm), Germany (AGS—acceptable cancer risk) (6 ppm) and China (6 ppm).
To account for multiple comparisons, the false discovery rate (FDR) was calculated for the set of p values from the comparisons between control and the low exposed group (<10 ppm). FDR results <0.20 were considered noteworthy. For these significant markers, further analyses including workers with even lower exposure levels (ie, <6, <5, <4, <3, <2 and <1 ppm) and unexposed controls were also conducted. All analyses were carried out using SAS V.9.4 software (SAS Institute, Cary, North Carolina, USA).
Results
Demographic characteristics including age, sex, BMI, current smoking, alcohol status and recent infection were comparable between the unexposed control and exposed subjects (table 1). The mean TCE exposure among the exposed workers was 22.2 ppm (SD: 35.9; range: 0.4–229) and median was 12 ppm, while TCE exposure was negligible in the control factories. On average, the exposed subjects worked for 2 years in the TCE facilities while unexposed subjects worked for 2.3 years in the control factories (data not shown). Six immune biomarkers (CD4+ effector memory T cells, sCD27, sCD30, IL-10, IgG and IgM) were significantly decreased (p<0.05 and FDR<0.20) and levels of one urinary kidney function (KIM-1) marker were significantly increased among workers exposed to <10 ppm compared with the unexposed controls (p<0.05 and FDR<0.20) (table 2). The % differences in biomarker levels among the low exposed group (<10 ppm) relative to unexposed controls were −19.2% for CD4+ effector memory T cells, −62.7% for sCD27, −34.9% for sCD30, −72.1% for IL-10, –16.0% for IgG, −35.2% for IgM and +52.5% for KIM-1. In addition, all of these biomarkers showed a statistically significant exposure-response gradient across controls, <10 and ≥10 ppm TCE exposure (table 2). An additional 12 biomarkers showed a significant exposure-response association, but levels were not significantly different among workers exposed to <10 ppm compared with unexposed controls. Also, the magnitude of the changes for these biomarkers were from −22.2% to +24.8% among workers exposed to <10 ppm compared with the unexposed controls.
Demographic characteristics of the subjects
Levels of biological markers by TCE exposure level
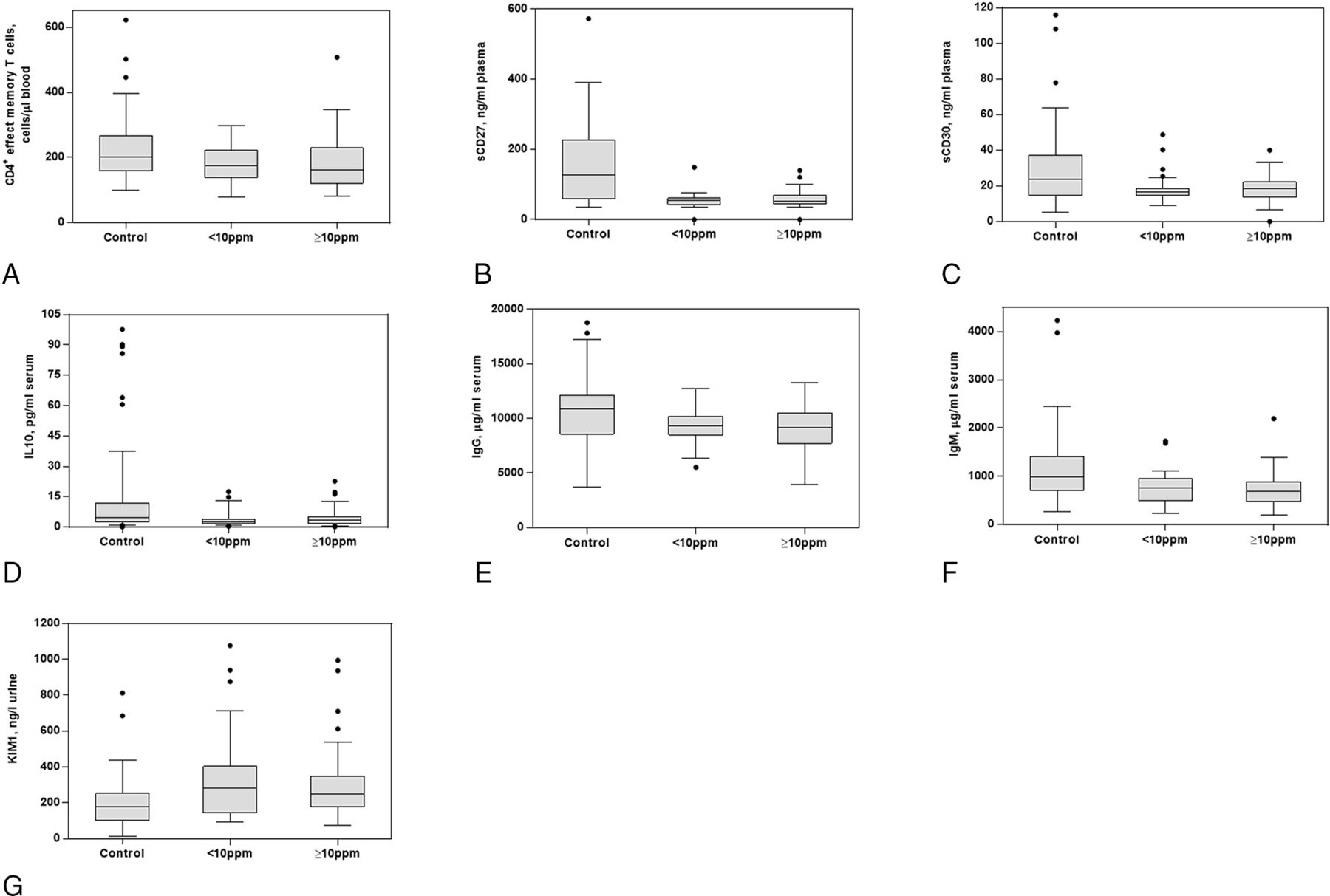
Figure 1 shows box plots for the seven markers that showed significant differences among the group exposed to <10 ppm compared with controls. Most of the seven markers except for CD4+ effector memory T cells showed non-monotonic exposure-response relationships with the level of TCE. Specifically, the magnitude of differences in levels of these biological markers were comparable in low and high exposed groups relative to the unexposed control workers. In addition, among these seven markers, four (sCD27, IgG, IgM and KIM-1) remained statistically significant when comparing levels in workers exposed to <6 ppm of TCE to unexposed controls (online supplementary table 1). Significantly decreased levels of IgM and sCD27 were also observed among the group exposed to <2 and <1 ppm of TCE compared with unexposed controls, respectively (online supplementary table 1). In general, these seven markers were weakly correlated with each other among both exposed and control workers, except for a higher correlation between sCD27 and sCD30 among controls (rsp=0.72; online supplementary table 2).
{kind=link}
Box plots for selected biomarkers that showed significant differences between controls and those exposed to <10 ppm of trichloroethylene (TCE). (A) CD4+ effect memory T cells, (B) sCD27, (C) sCD30, (D) interleukin (IL)-10, (E) IgG, (F) IgM and (G) KIM-1. Most of the box plots of the nine markers show non-monotonic dose-response relationships with the level of TCE. Thus, exposure to a much lower level of TCE than 10 ppm may cause significant effects on the level of these biomarker.
Discussion
Six immune regulation markers (ie, CD4+ effect memory T cells, sCD27, sCD30, IL-10, IgG and IgM), and one kidney function marker (KIM-1) were significantly different among those exposed <10 ppm compared with unexposed controls. Among these markers, sCD27, IgG, IgM and KIM-1 remained significant at exposure levels even lower at <6 ppm and sCD27 and IgM were significant at levels below 2 ppm. These results suggest that biological markers related to immune function and kidney toxicity are altered by low levels of occupational exposure to TCE (ie, <10 ppm or even lower than 6 ppm), below most current national occupational exposure standards.
A decrease in CD4+ effector memory T cells may lead to a decreased capacity of the body to respond to antigenic-related inflammation.16 A recent study has reported that TCE altered the expression of ∼560 genes in the same effector/memory CD4+ T cells.17 Both sCD27 and sCD30 are shed by B and T cells at activation and are important co-stimulator molecules in the regulation of the balance between Th1 and Th2 responses.18 19 IL-10 has been demonstrated to suppress chronic inflammation through apoptotic effects on developing macrophages and mast cells.20 22 A recent study has reported that the elevation of IL-10 level may be a kind of pathogenesis indicator in occupational medicamentosa-like dermatitis due to TCE.21 Both IgG and IgM are involved in a variety of host immunological functions, as increased levels of IgM are produced by B cells following antigen stimulation and function in the primary immune response during an acute infection, after which IgG antibodies are produced to mediate the secondary immune response.22 KIM-1 is known to be strongly upregulated in injured cells throughout the kidneys.23 Given that altered immunity, including immunosuppression, is an established risk factor for NHL,24 TCE exposure as low as <10 ppm may be mechanistically associated with NHL through the reduced capacity to respond to antigenic-related inflammation. Additionally, kidney toxicity caused by the exposure to low TCE levels may add to plausibility of the epidemiological findings linking TCE and kidney cancer.25
Evidence from experimental and epidemiological studies contributed to lowering the standards for occupational exposure to TCE from 100 to 50 ppm, 25 and 10 ppm (online supplementary figure 2).4 5 Although the US OSHA still maintains 100 ppm for regulatory purposes, OHSA in California set a standard of 25 ppm, NIOSH has recommended a standard of 25 ppm and ACGIH has suggested 10 ppm as the standard. It should be noted that most standards went into place before IARC designated TCE as a group 1 carcinogen. Given that current occupational standards for TCE in different countries vary considerably from 1 to 100 ppm (ie, the UK: 100 ppm, Mexico: 100 ppm, Japan-JSOH: 25 ppm and Russia: 10 ppm), studies to evaluate associations between lower levels of TCE exposure and biological changes are warranted. In this context, we focused on evaluating whether there are significant differences in the levels of molecular biomarkers among the group exposed to <10 ppm of TCE compared with unexposed controls.
Our findings suggest non-monotonic exposure-response relationships for most of the markers that showed significant differences between those exposed to <10 ppm of TCE and controls. The levels of several markers with non-monotonic exposure-response relationships were also altered significantly at even lower levels of TCE (ie, <2 ppm), and then tended to plateau as the level of TCE exposure increased. Out of the seven markers, four markers (ie, sCD27, IgG, IgM and KIM-1) remained statistically significant when the cut point was reduced at 6 ppm and two markers remained significant when the cut point was even below 2 ppm, which suggests the potential for a very low exposure threshold for alterations in these specific markers. On the other hand, for the markers with linear exposure-response relationships with TCE exposure level, whether we could detect significant alterations or not may depend on several factors including how steep the slope is (ie, effect size), population variation in levels of each marker and sample size.
Our study may have a limitation in that we could not disentangle the effect of long term exposure and short term exposure due to cross-sectional design. However, when we checked the correlations between work duration and each of the biomarkers, we only found marginally significant negative correlation with VEGF among the exposed subjects. We did further analysis stratified by work duration >2 years and <2 years. As shown in online supplementary table 2, a consistent trend for the end points between the two strata was observed. As another sensitivity analysis, we conducted Spearman’s correlation analyses between the covariates and each of the biomarkers. As shown in the online supplementary table 2, we only found only two noteworthy results: age was moderately correlated with decreased CD4+ naïve and CD8+ naïve cells, which is consistent with the function of naïve T cells taking centre stage on immune ageing26), and there was a moderate positive correlation between VEGF and gender, which supports the findings of a previous study27 that VEGF production according to VEGF 936C>T genotype might differ between men and women. However, the main results may have remained unchanged considering that covariates were already adjusted in the statistical model in our study.
In conclusion, our study suggests that even at levels of exposure below typical regulatory limits (ie, 10 ppm), certain biomarkers related to immune function and kidney toxicity may be altered by occupational exposure to TCE. Our results contribute to the scientific evidence of biologic changes experienced by workers who are exposed to relatively low level of TCE and raises a question about whether any occupational exposure to TCE can be considered ‘safe’. Continued efforts are warranted to investigate the biologic effects and health outcomes at low levels of exposure to TCE.
References
Footnotes
Contributors QL, MTS, NR, and LZ designed this study, managed data collection and participated in data processing. K-ML conducted the analyses and was primarily responsible for writing the paper under the supervision of QL. WH conducted the statistical analyses. All authors contributed to draft manuscripts and the final version. QL and NR are the guarantors.
Funding Intramural funds from National Institutes of Health and National Cancer Institute; National Institute of Environmental Health Sciences (P42ES04705 and P30ES01896 to MTS); Northern California Center for Occupational and Environmental Health and Department of Science and Technology of Guangdong Province, China (2007A050100004); International Research Fund (2018) from Korea National Open University
Competing interests None declared.
Ethics approval The study was approved by institutional review boards at the US National Cancer Institute and the Guangdong National Poison Control Center, China.
Provenance and peer review Not commissioned; externally peer reviewed.
Patient consent for publication Not required.