Article Text

Abstract
Background Vibration-induced white finger (VWF) is the vascular component of the hand–arm vibration syndrome (HAVS). Two tests have been standardised so as to assist the diagnosis of VWF: the measurement of finger rewarming times and the measurement of finger systolic blood pressures (FSBPs).
Objectives This study investigates whether the two tests distinguish between fingers with and without symptoms of whiteness and compares individual results between the two test methods.
Methods In 60 men reporting symptoms of the HAVS, the times for their fingers to rewarm by 4°C (after immersion in 15°C water for 5 min) and FSBPs at 30°C, 15°C and 10°C were measured on the same day.
Results There were significant increases in finger rewarming times and significant reductions in FSBPs at both 15°C and 10°C in fingers reported to suffer blanching. The FSBPs had sensitivities and specificities >90%, whereas the finger rewarming test had a sensitivity of 77% and a specificity of 79%. Fingers having longer rewarming times had lower FSBPs at both temperatures.
Conclusions The findings suggest that, when the test conditions are controlled according to the relevant standard, finger rewarming times and FSBPs can provide useful information for the diagnosis of VWF, although FSBPs are more sensitive and more specific.
- Vibration-induced white finger
- Hand-arm vibration syndrome
- Hand-transmitted vibration
- Finger skin temperature
- Finger systolic blood pressure
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
- Vibration-induced white finger
- Hand-arm vibration syndrome
- Hand-transmitted vibration
- Finger skin temperature
- Finger systolic blood pressure
What this paper adds
Previous studies have compared signs and symptoms between the hands of workers exposed to vibration and those in control groups. This study investigated the ability of two alternative objective tests to identify individual fingers with symptoms of vibration-induced white finger (VWF).
Finger rewarming times and finger systolic blood pressures (FSBPs) distinguished between fingers with and without reported whiteness. FSBPs had greater sensitivity and greater specificity than finger rewarming times.
FSBPs were lower in fingers reported to have greater areas of whiteness (ie, greater blanching scores), suggesting that FSBPs also reflect the severity of VWF.
Introduction
The term ‘hand–arm vibration syndrome’, HAVS, is used to describe vascular, neurological and other disorders associated with occupational exposures to hand-transmitted vibration. One of the vascular disorders caused by hand-transmitted vibration is vibration-induced white finger, VWF, sometimes considered a form of secondary Raynaud's phenomenon.
The diagnosis of VWF is currently heavily reliant on the reporting of relevant symptoms, such as cold-induced finger blanching, and an appropriate history of exposure to hand-transmitted vibration. The cold-induced blanching led to two alternative tests involving exposure to cold that are standardised in part 1 and part 2 of ISO 14835: the measurement of finger rewarming times after cold provocation1 and the measurement of finger systolic blood pressures (FSBPs) during cold provocation.2
The time for finger skin temperature (FST) to rewarm after the hand and fingers have been cooled is widely used as an indicator of the abnormal response to cold observed in those with symptoms of VWF. Notwithstanding many investigations of the test,3–8 it is not possible to state its diagnostic power. There have been wide variations in the nature of the cold challenge (eg, duration and temperature of the cold challenge) and the diagnostic criteria used to identify an abnormality (eg, the extent of finger blanching). Some studies have suggested that the test may be useful for discriminating, on a group basis, between those with and those without vibration-induced vascular problems, but that it lacks the sensitivity and specificity to distinguish between individuals with and without VWF.4 ,9 ,10 The diagnostic usefulness of a specific form of the rewarming test applied in the UK for medicolegal compensation claims has been questioned.11–13 This has encouraged the diagnosis of VWF from the reported symptoms, although this seems unsatisfactory when diagnoses determine whether workers lose their jobs or are awarded compensation. In air, FST depends on the environmental conditions and blood flow through the digit,5 so the reliability of the test as an indicator of VWF can be expected to depend on many factors, especially the environmental conditions before, during and after the hands are immersed in water.
The measurement of FSBPs after cold provocation is less commonly used than that of finger rewarming times, possibly because more complex equipment is needed for the test. During cold provocation of the fingers, the blood vessels constrict and FSBP falls.14–17 The reduction is usually small in healthy persons but greater in fingers that are affected by the blanching associated with VWF.18–20 The cold-induced reductions in FSBPs seem to be related to reports of finger blanching and have been reported to have greater sensitivity and greater specificity than finger rewarming times.9 ,21 It has been suggested that FSBPs are more reproducible than finger rewarming times and that cold-induced reductions in FSBPs are more useful indicators of VWF than finger rewarming times.9 ,22 ,23
Studies involving objective indicators of abnormal response to cold have mostly used either finger rewarming times or FSBPs, so there are few comparisons of the two tests. Moreover, published studies in which both tests have been performed focus on the overall sensitivity and specificity of the two tests rather than differences between the two tests in individuals.9 ,24 ,25
This study investigated whether finger rewarming times1 and FSBPs2 distinguish between fingers with and without whiteness, and whether the tests distinguish between fingers with different degrees of whiteness, as indicated by blanching scores.26 The study allowed the findings of the two tests to be compared in a group of men who reported symptoms of HAVS. It was hypothesised that finger rewarming times would be increased and FSBPs would be reduced in fingers reported to suffer attacks of whiteness. It was further hypothesised that there would be a negative correlation between the results of the two tests, indicating that fingers more affected according to one test would tend to be more affected according to the other test.
Methods
The two tests were performed under the same environmental conditions by an experimenter experienced in applying the tests according to the recommended procedures.24
Apparatus
Finger rewarming times (HVLab 8-channel temperature monitor, University of Southampton).
An HVLab temperature monitor was used to measure the rewarming times following cold provocation. Calibrated thermocouples were attached to the palmar surfaces of the fingertips of the thumb, index, ring and little fingers, and the distal, middle and proximal phalanges of the middle finger of the right hand. One thermocouple was attached to the fingertip of the left middle finger as a reference.
The patients sat next to a table supporting a water bath and temperature monitor. The height of the seat was adjusted so that participants were comfortable and able to maintain a similar posture throughout the experiment. A very thin and loose waterproof glove was placed on the right hand. After a settling period of 2 min with both hands at heart level, the right hand was immersed in stirred water at 15°C for 5 min. The patient then removed the right hand from the water with the help of the experimenter, the thin glove was removed and the right hand kept at heart level to rewarm for 11 min. Throughout the test, the left hand rested on a foam support at heart level and remained motionless. There was continuous monitoring of FST during the settling period and the hand cooling and rewarming periods using a computer and HVLab diagnostic software (V.8.5, University of Southampton). The test started only if the skin temperature was stable (ie, FST varied by <1°C over 5 min). The time for FST to increase by 4°C after cold provocation was used as the indicator of dysfunction.24 If the fingers had not rewarmed by 4°C within 11 min, a rewarming time of 660 s was assumed.
Finger systolic blood pressures (HVLab multichannel plethysmograph, University of Southampton)
An HVLab plethysmograph was used to measure FSBPs following cold provocation of the digits. Water-perfusable cuffs were placed around the middle phalanx of each finger, with a separate air cuff around the thumb as a reference. Strain gauges were placed at the base of the finger nails of cuffed fingers. Patients lay supine and motionless on a couch with both hands supported at heart level so as to minimise effects of hydrostatic variations. The fingertips were squeezed to reduce blood volume and then the cuffs were inflated to 220 mm Hg (a suprasystolic pressure to prevent arterial inflow) by perfusing the cuffs with thermostatically controlled water. After 5 min of ischaemia, the cuff pressure was reduced at a rate of 2 mm Hg/s. The FSBPs were measured on the right hand after cooling by water circulating at 30°C, 15°C and 10°C. The FSBP was the cuff inflation pressure at which arterial inflow returned to the finger. The percentage changes in finger systolic blood pressures (%FSBP) were calculated according to the following equation: where FSBPt°C is the finger systolic pressure of the test finger after thermal provocation at 10°C or 15°C;
where FSBPt°C is the finger systolic pressure of the test finger after thermal provocation at 10°C or 15°C;
FSBPtest,30°C is the FSBP measured on the test finger after thermal provocation at 30°C;
FSBPref,30°C is the FSBP measured on the thumb after thermal provocation at 30°C;
FSBPref,t°C is the FSBP measured on the thumb after thermal provocation at 10°C or 15°C.
Participants
Sixty male patients referred to the Institute of Sound and Vibration Research (University of Southampton) for Tier 5 HAVS assessment were asked and all agreed to participate in the study.26 This study reports findings from all 60 successive participants (ie, there were no exclusions). The patients were medicolegal referrals and employer referrals. They had standardised rewarming tests and FSBP measurements as part of their assessment. The participants were in the clinic at a constant ambient temperature of 21±1°C, with 40–45% humidity and no noticeable air flow for more than 2 hours before the two vascular tests were started.
All patients were right handed and with a history of occupational use of hand-held vibratory tools: a mean exposure of 23 years (SD: 6.8, range: 5–45 years). They had used a wide range of vibratory tools in various jobs (eg, gardener, maintenance worker, welder, fitter, etc). The mean age of the patients was 52.9 years (SD: 12.4, range: 30–70 years), their mean stature was 176.8 cm (SD: 5.7, range: 165–190 cm), their mean weight was 83.1 kg (SD: 11.8, range: 63–126 kg) and their mean body mass index (BMI) was 26.6 kg/m2 (SD: 5.7, range: 19.6–38.8 kg/m2). All 60 patients participating in the study had a smoking history but 8 patients were not currently smoking.
The participants were requested to avoid vibration exposure on the day of the test and to avoid consuming caffeine and tobacco for 4 hours and alcohol for 12 hours prior to the testing.
Procedure
Patients attended the clinic on one occasion. Initially, they were questioned about their occupational history, social and medical history, and symptoms. The locations of any reported finger blanching, numbness or tingling were mapped using the scoring system.27 The following tests were then performed in sequence:26 Purdue pegboard, grip strength, thermotactile thresholds, vibrotactile thresholds, finger rewarming times and FSBPs. The FSBPs were not measured until at least 60 min after the completion of the finger rewarming test and not before the FST had recovered to within at least 2°C of the baseline finger temperature. The symptoms were not collected by the experimenter responsible for measuring finger rewarming times and FSBPs.
Statistical methods
Data analysis was performed using the software package SPSS (V.19.0). The data were summarised with the median as a measure of central tendency and the IQR as a measure of dispersion. Non-parametric tests were employed to analyse the data, which were not normally distributed. The Wilcoxon matched pairs signed-ranks test was used to investigate differences between the measures of %FSBP at two water temperatures (ie, 15°C and 10°C). The Friedman test was used to investigate differences between measurement locations for finger rewarming times and %FSBP. The Mann-Whitney U test was used to investigate differences between groups: fingers with and without symptoms of finger blanching and fingers with different blanching scores. The Spearman rank correlation coefficient was used to investigate associations between finger rewarming times and %FSBP. The diagnostic criteria used in the study were: (1) times to rewarm by 4°C that were longer than 300 s and (2) %FSBPs <80%. Receiver operating characteristic (ROC) analysis showed the effects of varying these criteria. The diagnostic accuracies of different measures of finger rewarming were investigated by comparing the areas under the ROC curves (AUC).
The criterion for statistical significance was p<0.05. The reported p-values have been adjusted for multiple comparisons.
Results
For each of the five fingers on the right hands of the 60 patients, symptoms of finger blanching were categorised into two groups depending on the symptom reported: Group A—finger reported to suffer attacks of whiteness, and Group B—finger reported to suffer no attacks of whiteness. Because the symptoms differed between fingers, the number of fingers in Groups A and B varied between the fingers. The symptoms were categorised only as ‘finger whiteness’ if they were reported to be provoked by cold conditions and the areas affected by whiteness were clearly demarcated from areas not affected by whiteness.
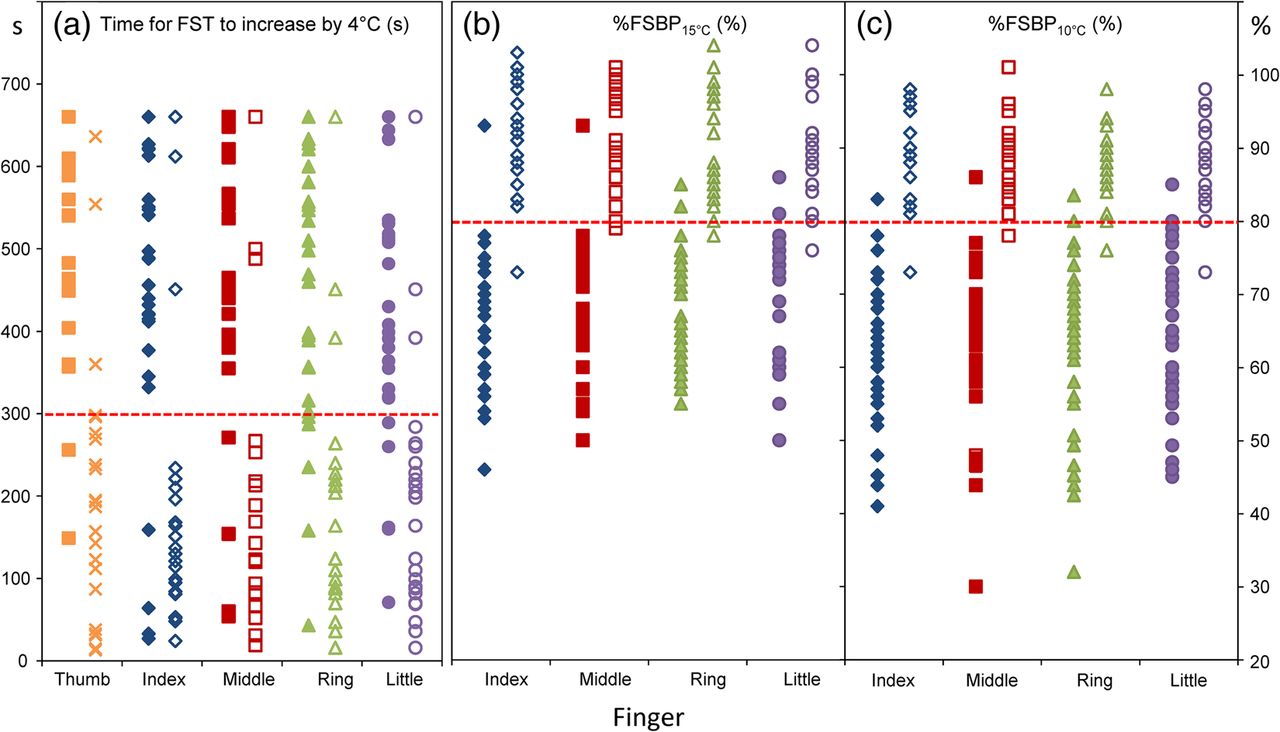
The individual times for FST to rewarm by 4°C, %FSBP15°C and %FSBP10°C on the right hand in Groups A and B are shown in figure 1.

Individual measures of times for finger skin temperature to rewarm by 4°C, %FSBP15°C and %FSBP10°C on fingers of the right hand in Group A (solid points) and Group B (hollow points). Broken horizontal lines indicate the criteria for dysfunction (ie, >300 s for rewarming times; <80% for finger systolic blood pressures).
The median, IQR, minimum and maximum of finger rewarming times, %FSBP15°C and %FSBP10°C on the index, middle, ring and little fingers with different blanching scores (score 0, 1, 3 and 6) are shown in figure 2.

Median, IQR, minimum and maximum of finger rewarming times, %FSBP15°C and %FSBP10°C on the index, middle, ring and little fingers with different blanching scores.
The ROCs for finger rewarming times and %FSBPs at 15°C and 10°C are shown in figure 3.

The receiver operating characteristics (ROC) curve for finger rewarming times (time for FST to rewarm by 4°C), and %FSBPs at 15°C and 10°C.
Finger rewarming
During the 2 min baseline period, the temperatures on the fingertips of the ring and little fingers were lower than those on the fingertips of the thumb, index and middle fingers in Group A (p<0.05), but not in Group B (p=0.12–0.32). The FSTs on the ring and little fingers were lower in Group A than in Group B (p<0.01), but there were no significant differences on the other three fingers (p=0.11–0.42).
During the 5 min immersion period, there was a trend for slightly lower FST at the 5th minute of cold provocation in Group A than in Group B, although statistically significant only for the ring and little fingers (p<0.05).
After adjustment for multiple comparisons, the finger rewarming times for all locations on the right hand were greater in Group A than in Group B (p<0.001).
On the left middle finger (ie, reference finger not immersed in cold water), there was no significant change in FST across the 2 min baseline period, the immersion period and the recovery period in either Group A or Group B (p=0.38–0.53).
Inter-individual variability in finger rewarming times is indicated by the ratio of the IQR to the median and showed similar variability in Group A (57–73%) and in Group B (67–74%). For the fingers in Group A, the upper quartile value was 660 s, the cut-off time for the recovery period. A greater IQR would have been obtained in these fingers if the recovery had been monitored beyond 11 min.
On fingers with whiteness, there was no significant difference in rewarming times between different whiteness scores (p=0.07–0.47). There was no difference between smoking and non-smoking groups on baseline FST and finger rewarming times (p=0.12–0.84).
Of the 300 fingers participating in the finger rewarming test, 143 fingers would be identified as having dysfunction when using the criterion of rewarming by 4°C within 300 s. The sensitivity and specificity of the finger rewarming test were 77% and 79%, respectively, with an AUC of 0.80 (CI of 0.74 to 0.85) (figure 3(a)).
The baseline FSTs were not correlated with rewarming times in Group A (p=0.12), but there was a negative correlation for fingers without whiteness in Group B (p=0. 02). The FST measured at the 5th minute of the immersion period was not correlated with the time for FST to rewarm by 4°C in either Group A or Group B (p=0. 22–0.46).
Comparisons between different measures of the FST after cold provocation
Eight measures of rewarming were calculated from the rewarming profile to represent alternative measures employed in previous studies. The measures have been grouped as: (1) times to rise by 3°C, 4°C or 6°C, (2) absolute temperature after 5 or 10 min of recovery, (3) rates of change of temperature to 5 or 10 min of recovery and (4) the area above the rewarming curve (ie, area between the FST during the recovery period and the FST measured during the baseline period10). The medians (and IQRs) of these measures for fingers with and without whiteness are shown in table 1. The sensitivity, the specificity and the AUC for the detection of whiteness on individual fingers are also shown in table 1.
Medians (and IQR) for eight measures describing components of the finger skin temperature response to cold, and corresponding sensitivities, specificities and AUC (and 95% CI)
Finger systolic blood pressures
The FSBP at 30°C was not significantly different between Group A and Group B for fingers on the right hand (p=0.22–0.62). The FSBP at 30°C did not differ across the right index, middle, ring and little fingers in either Group A (p=0.31) or Group B (p=0.46).
The FSBP measured in air on the reference right thumb did not differ when the temperature of the other fingers varied between 30°C, 15°C and 10°C in either Group A or Group B (p=0.56).
After adjustment for eight multiple comparisons, the %FSBPs on the right index, middle, ring and little fingers were lower in Group A than in Group B (p<0.01).
In fingers with whiteness, the %FSBPs on the index, middle, ring and little fingers were lower at 10°C than at 15°C (Group A, p<0.01), but in fingers without whiteness, there was no significant difference (Group B, p=0.23). There was a positive correlation between %FSBPs at 15°C and 10°C in both Group A and Group B (p<0.01), showing that fingers with the lower %FSBP at 15°C tend to also have a lower %FSBP at 10°C.
The ratio of the IQR to the median %FSBP15°C showed greater variability in Group A (11–15%) than in Group B (7–12%). The ratios for the %FSBPs at 10°C were 14–16% in Group A and 7–11% in Group B.
On fingers with whiteness (ie, Group A), the %FSBPs (at both 15°C and 10°C) were lower on fingers with a blanching score of 6 than on fingers with a blanching score of 1 or 3 (p<0.01). There were no significant differences in %FSBP at either 15°C or 10°C between blanching scores of 1 and 3 (p=0.07–0.29).
There was no difference between smoking and non-smoking groups in the FSBP at 30°C or the %FSBPs at 15°C or 10°C (p=0.17–0.31).
Of the 240 fingers (thumbs not tested) participating in the FSBP test, 136 and 141 fingers would be identified as having dysfunction when using the criterion of the %FSBP being <80% with water temperatures of 15°C and 10°C, respectively. The sensitivities and specificities of the FSBP test were, respectively, 93% and 95% for %FSBP15°C and 97% and 95% for %FSBP10°C. The AUC was 0.93 (CI of 0.89 to 0.96) for %FSBP15°C and 0.95 (CI of 0.91 to 0.98) for %FSBP10°C (figure 3(b) (c)).
Associations between finger rewarming times and percentage changes in FSBPs
The times for each of the four fingers to rewarm by 4°C tended to increase as the %FSBP at either 15 or 10°C reduced (figure 4). After adjustment for multiple comparisons, the finger rewarming times on the fingers with whiteness were negatively correlated with the %FSBP15°C on the index, ring and little fingers (p<0.05), but not on the middle finger (p=0.06). With reduced water temperature when measuring FSBPs, there was a negative correlation between finger rewarming times and %FSBP15°C on all four fingers of the right hand (p<0.01). A similar trend was found within Group B: negative correlations between finger rewarming times and FSBPs at both 15°C and 10°C (p<0.05).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Relationship between individual times for FST to rewarm by 4°C and %FSBP at 15°C on the index, middle, ring and little fingers of the right hand.
Discussion
Finger rewarming
The diagnostic indicator for finger rewarming used in this study was the time for the FST to rewarm by 4°C. This provided a useful indication of fingers with and without symptoms of VWF, with 77% sensitivity and 79% specificity. This is consistent with some previous studies that have concluded finger rewarming can distinguish between groups with and without VWF.3 ,5 ,8 ,10 ,23 ,28
The methods of measuring rewarming have differed widely, but even when the same method has been used, different sensitivities and specificities of the test for detecting VWF have been reported. For example, whole-hand immersion in water at 10°C for 10 min has yielded sensitivities between 20% and 91% and specificities between 37% and 100%.6 ,29–32
Many factors may be expected to influence the sensitivity and specificity of a rewarming test, including differences between test conditions and assessment protocols. Patients in the current study were not tested in the summer season. They stayed in the clinic with a constant ambient temperature, with no noticeable air flow, and with humidity around 40–45%. Some investigators have considered the sensitivity of the test applied to one finger as an indicator of the presence of VWF on any finger of the hand, or the staging of VWF on the whole hand. Since symptoms of the vascular disorder known as VWF vary between fingers, and between phalanges, an assessment of the sensitivity and specificity of a measure of finger rewarming should be specific to a finger and not averaged over a whole hand. On this basis, it is more appropriate to assess the value of the test using finger blanching scores than the Stockholm staging of the vascular component of the HAVS.
A large inter-individual variability in rewarming times may be explained by the finger rewarming times after a cold challenge being dependent on changes in finger blood flow mediated by several different mechanisms.5 The vasodilation process during recovery could be due to a gradual release of arterial vasospasm3 or a combination of different mechanisms.6 A previous study suggested that the results of the test should be interpreted with respect to the state of the initial blood flow.10 A low blood flow during the settling period may be indicative of poor capillary blood flow or obstructive disorders of the peripheral circulation.
In fingers without whiteness, rewarming tended to be quicker when the baseline FST was higher. However, in fingers with whiteness, there was no correlation between baseline FST and rewarming times. Furthermore, the baseline FST was not significantly different between fingers with and without whiteness. These findings suggest that in the conditions of this study, the baseline FST is not a useful measure for the diagnosis of VWF, although it does indicate differences in peripheral circulation among healthy participants.
Limitations of the finger rewarming test have been reported by previous researchers who have concluded that the sensitivity and specificity of the test can be low and that the value of the test is highly influenced by the test conditions and assessment protocols.5 ,10 In the ROC curves, the further the central portion of the curve moves upwards and to the left, the better the measure is at distinguishing between fingers with and without whiteness. In the ROC curve analysis, AUCs of 0.8, 0.65 and 0.5 are described as having, respectively, ‘good’, ‘fair’ and ‘poor’ discriminative ability.33 For the time it took the FST to rise by 4°C, the AUC was 0.80 in the current study, indicating that the finger rewarming test can provide a ‘good’ indication of whether a finger has whiteness when the test conditions and assessment protocols are as described here.
Comparison of alternative measures of finger rewarming
All eight measures used in this study distinguished between fingers with and without whiteness: in fingers with whiteness, there was significantly reduced FST during recovery, reduced rate of recovery, increased times for the FST to rise to specific temperatures and a greater area above the rewarming curve. The sensitivity and specificity of these measures suggest that the time for FST to rise by 4°C, the temperature at the 5th minute of recovery and the area above the rewarming curve have the greatest power for detecting the abnormal response to cold provocation associated with VWF.
The alternative measures of finger rewarming may reflect the activity of different physiological mechanisms involved in the response of the body to cold provocation. Of the three measures that performed well here, neither the time to rise by 4°C nor the temperature at 5th minute of recovery reflects the shape of the response profile. Although the single value given by the area above the rewarming curve does not distinguish between different ‘patterns’ of response to cold, it requires the recording of the full rewarming curve that may contain information on the response of several physiological mechanisms and may become more useful in the future.
Finger systolic blood pressures
The measures of FSBP used in this study were the %FSBP after cold provocation at 15°C and 10°C. Significantly lower %FSBPs were observed on fingers with symptoms of whiteness than in fingers without symptoms of whiteness. This is consistent with previous conclusions that FSBPs during local cooling are useful for detecting an abnormal cold response in the digital blood vessels of workers exposed to hand-transmitted vibration.17 ,34–40 Using the same test conditions and criteria, previous studies have reported a sensitivity of 84–99% and specificity 94–100%.34 ,38–40 The present findings suggest that the test has the ability to not just distinguish between control participants without symptoms and workers exposed to hand-transmitted vibration with symptoms but also discriminate between fingers with and without whiteness, which allows confirmation of the pattern of symptoms reported by a VWF patient.
The results suggest that %FSBPs are powerful indicators of VWF. They have sensitivity and specificity >90% and an AUC >0.9. The reduced %FSBPs on fingers with greater whiteness scores suggest that the test may also be used to indicate the severity of symptoms, which can influence medical decisions on the removal of symptomatic workers from exposure to vibration.
The positive correlation between %FSBP15 and %FSBP10 implies that the FSBP could be measured after cooling to only one of these two temperatures. The slightly lower %FSBP10 in fingers with whiteness, and the greater sensitivity and specificity with %FSBP10, suggests that FSBPs could be measured solely at 10°C. Although the test can be a little painful at 10°C, there is less pain (and a saving of time) in conducting the test only at 10°C than conducting it at both 15°C and 10°C.
Association between finger rewarming times and %FSBP
The times for fingers to rewarm by 4°C were negatively correlated with %FSBPs at both 15°C and 10°C. This indicates that the response of the fingers is similar in both tests: fingers with longer times to recover after cold provocation generally have lower FSBPs during local cooling. Using the normal criteria for dysfunction, of the 140 fingers reported to suffer from whiteness, 77% had dysfunction according to the finger rewarming test and 97% had dysfunction according to the FSBP test. The false-positive rates of the rewarming test and the FSBP test were 21% and 5%, respectively. Although there is no known previous study comparing the two standardised tests in individuals, a review of objective tests for the diagnosis of VWF has concluded that both tests can provide useful indications of dysfunction and assist the diagnosis of VWF.25
Finding an abnormally long rewarming time or abnormally low %FSBP is not sufficient to diagnose VWF. The findings should be related to symptoms on the same finger (eg, a reliable history of attacks of finger blanching), a work history of exposure to hand-transmitted vibration that may be associated with a risk of injury and the absence of alternative explanations of the signs and symptoms, including primary Raynaud's phenomenon.
Although self-reported areas of whiteness can be overestimated or underestimated, this would not have affected the relative performance of the two alternative tests for dysfunction. Although the results indicate this type of error could not have been common in this study, it is because the symptoms cannot always be trusted that a reliable test is required. Other factors, such as the duration and frequency of symptoms, the rate of progression of symptoms, the age of the patient, etc, may also have an influence on the sensitivity and specificity of the tests.
Conclusions
Using the test conditions and assessment protocols applied in this study, the finger rewarming times1 and FSBPs2 showed differences between fingers with and without symptoms of VWF.
FSBPs after cooling were more sensitive and more specific than finger rewarming times. Moreover, the FSBPs were lower in fingers reported to have greater areas of whiteness (ie, greater blanching scores), suggesting the %FSBP also reflects the severity of VWF.
References
Footnotes
Contributors YY and MJG involved in conception and design of research; interpreted results of experiments; prepared figures; and drafted, revised and approved the final version of manuscript. YY performed experiments and analysed data.
Competing interests None declared.
Patient consent Obtained.
Ethics approval The study was approved by the Ethics Committee of the Faculty of Engineering and the Environment at the University of Southampton (10704).
Provenance and peer review Not commissioned; externally peer reviewed.