Article Text

Abstract
Objectives Surgeons become uncomfortable while performing surgery because heat transfer and evaporative cooling are restricted by insulating surgical gowns. Consequently, perceptions of thermal discomfort during surgery may impair cognitive performance. We, therefore, aimed to evaluate surgeons’ thermal comfort, cognitive performance, core and mean skin temperatures, perceptions of sweat-soaked clothing, fatigue and exertion with and without a CoolSource cooling vest (Cardinal Health, Dublin, Ohio, USA).
Methods Thirty orthopaedic surgeons participated in a randomised cross-over trial, each performing four total-joint arthroplasties with randomisation to one of four treatment sequences. The effects of cooling versus no cooling were measured using a repeated-measures linear model accounting for within-subject correlations.
Results The cooling vest improved thermal comfort by a mean (95% CI) of −2.1 (–2.7 to –1.6) points on a 0–10 scale, p<0.001, with no evidence of treatment-by-period interaction (p=0.94). In contrast, cooling had no perceptible effect on cognition, with an estimated mean difference (95% CI) in Cleveland Clinic Cognitive Battery (C3B) Processing Speed Test score of 0.03 (95% CI –2.44 to 2.51), p=0.98, or in C3B Visual Memory Test score with difference of 0.88 (95% CI –2.25 to 4.01), p=0.57. Core temperature was not lower with the cooling vest, with mean difference (95% CI) of −0.13 (–0.33°C to 0.07°C), p=0.19, while mean skin temperature was lower, with mean difference of −0.23 (95% CI –0.40°C to –0.06°C) lower, p=0.011. The cooling vest significantly reduced surgeons’ perceptions of sweat-soaked clothing, fatigue and exertion.
Conclusions A cooling vest worn during surgery lowered core and skin temperatures, improved thermal comfort, and decreased perceptions of sweating and fatigue, but did not improve cognition. Thermal discomfort during major orthopaedic surgery is thus largely preventable, but cooling does not affect cognition.
Trial registration number NCT04511208.
- Health Personnel
- Physical Exertion
- Differential Thermal Analysis
- Personal Protective Equipment
- Occupational Stress
Data availability statement
Data are available on reasonable request. The data that support the findings of this study are available from the authors, on reasonable request. It can be addressed to FAR-P (RODRIGF3@ccf.org), the project leader.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
- Health Personnel
- Physical Exertion
- Differential Thermal Analysis
- Personal Protective Equipment
- Occupational Stress
WHAT IS ALREADY KNOWN ON THIS TOPIC
Layers of personal protective equipment (PPE) worn during surgery makes surgeons uncomfortably warm. How best to prevent the sensation of overheating and whether surgeons’ thermal discomfort impairs cognitive performance remains unknown.
WHAT THIS STUDY ADDS
A conductive cooling vest worn by surgeons under PPE reduced thermal discomfort, fatigue and exertion and lowered skin and core body temperatures. However, cooling did not affect cognitive performance.
HOW THIS STUDY MIGHT AFFECT RESEARCH, PRACTICE OR POLICY
Our results support using cooling systems to improve thermal comfort of surgical personnel in operating rooms, and other excessively warm occupational settings.
Introduction
Surgeons do physically demanding work while wearing impervious protective garments that impede heat transfer and evaporation. The result is a microclimate under the personal protective equipment (PPE) that is often excessively warm. Thermal discomfort is thus common and may impair cognitive function, even in relatively cool operating rooms. For example, the added burden of PPE increases skin temperature resulting in sensory displeasure that can alter an individual’s subjective state and impair effective decision-making.1
A conductive cooling vest worn during surgery can mitigate thermal discomfort experienced by surgeons. For example, de Korte et al determined that cooling vests worn under PPE by COVID-19 nurses significantly alleviated the heat strain they experienced.2 In addition, cooling garments evaluated in warm occupational environments identified they improve performance, decrease heat strain, lower body temperature and minimise sweating.3
A disposable non-tethered, light weight (CoolSource) cooling vest was developed a decade ago for surgical personnel to reduce thermal strain. Ice packs inserted into the vest are distributed over to the shoulders, back and flank areas of the torso and cool for approximately 2.5 hours. However, the extent to which the cooling system mitigates thermal discomfort and affects physiological and perceptual responses of surgical personnel during real-time surgery remains unknown. In a randomised cross-over trial, we aim to evaluate the physiological and perceived responses of orthopaedic surgeons performing major joint arthroplasties with and without a cooling vest. We tested the hypothesis that conductive cooling vests worn by surgeons improves their perception of thermal comfort. Secondly, we tested the hypothesis that wearing a cooling vest preserves cognitive performance, reduces mean skin and core temperatures, decreases the perception of sweat-soaked scrub clothing, and reduces perceptions of fatigue and exertion.
Methods
We enrolled 30 orthopaedic surgeons aged 28–62 years between June 2020 and December 2020.
Protocol
Each surgeon participated during four separate working days at least 1 day apart while performing total-joint arthroplasties expected to last 90–150 min. Surgical cases were excluded on any given day if the surgeon had a fever (oral temperature exceeding 38°C) within 24 hours. The protocol excluded cases when the surgeon sat during the procedure, or needed to wear a lead X-ray apron. Prior to participation, each surgeon selected one of two options for face and head protection: (1) traditional surgical cap, face shield and goggles or (2) a surgical helmet. The selected covering was then used for all four trial operations.
For each case, the surgeon was randomly assigned to either routine scrubs and protective gowns or to a cooling vest worn between scrubs and PPE. Due to the nature of the intervention, investigators and participants were aware of their treatment allocations. Randomisation was blocked so each surgeon was assigned twice to the (A) control condition and twice to the (B) cooling vest intervention, with each surgeon randomised to one of four sequences for their four surgeries: AABB, BBAA, ABBA or BAAB. Randomisation was based on computer-generated codes maintained in a web-based system that was accessed shortly before surgery.
Measurements
Ambient operating room temperature was maintained near 20°C4 and recorded from a digital thermometer positioned six feet from the operating room table at the level of the patient.
Surgeons rated their thermal comfort with a commonly used measurement approach4 before surgery and immediately afterwards on a 0–10 Likert scale, with 0 representing extreme cold, 5 being neutral and 10 representing extreme heat. A functionally similar thermal comfort scale, the Rohles Thermal Comfort Scale, has established validity and reliability.5
Skin temperature was measured with wireless TempTraq patches (Blue Spark Technologies, Westlake, Ohio, USA) which meet professional accuracy standards calibrated to an uncertainty of no more than ±0.1°C. Skin temperature sensors were attached to the surgeon’s upper chest, deltoid arm, thigh and calf with bioadhesive covers. None of the cutaneous thermometers was located under or near an ice pack. Mean skin temperature was estimated from temperatures on the chest, arm, thigh and calf.6
The surgeons’ core body temperature was monitored by a validated wireless iThermonitor WT701 biosensor (Raiing, Boston, Massachusetts, USA). The thermometer has a precision of ±0.5°C, but over many measurements in many surgeons, provides an accurate estimate of core temperature with an average bias of just 0.14°C.7 8
Surgeons cognitive performance was assessed with the Cleveland Clinic Cognitive Battery (C3B) (Qr8 Health; Cleveland, Ohio, USA), The C3B is a computer-based self-assessment of visual memory tests, VMT (episodic and delayed memory) and processing speed test (PST) (information processing speed and incidental memory) that is described as reliable and valid in five substudies.9 The VMT consists of 7 symbols placed on a 4×6 cell checkerboard for 10 s. The symbols are removed and the participants return the symbols to the assigned square in five separate trials. Two points are awarded if both the location and symbol are placed in the correct square. A maximum score for 5 trials is 70.10
The PST display consists of a randomly generated symbol-digit key at the top of the screen and the participant inserts the appropriate digit below each symbol consistent with the key, moving automatically from left to right. Each row contains 15 symbols and automatically appears and is repeated for a total of 120 s. Both total correct and total incorrect responses are recorded.10
The surgeons’ cognitive performance was tested prior to the surgical hand scrub and immediately after surgery while in the operating room. Distractions were minimised by having the surgeon wear a sound-reducing headset each time the C3B was administered. Additionally, interruptions and distractions (ie, phone call, pager, staff, equipment) were recorded because the PST is a timed module and interruptions could reduce performance.
Sweat-soaked scrub clothing is uncomfortable and can generate a perception of thermal discomfort.11 The surgeons’ perception of sweat-soaked scrub clothing was rated using a Likert scale from 0=‘not wet at all’ to 10=‘fully drenched’. The Borg Rating of Perceived Exertion Scale12 is a reliable measure of exertion and is a widely accepted tool for measuring effort and exertion.13 14 The surgeons were asked to rate the level of exertion needed to perform the surgical procedure using The Borg scale, ranging from 6 (no exertion) to 20 (maximal exertion) after completing the surgical procedure.
The Rating of Fatigue scale measures the surgeons’ perceived level of fatigue by asking the surgeon to rate how fatigued they feel after completing the surgical procedure. The scale ranges from 0 (not fatigued) to 10 (totally fatigued and exhausted) and has high levels of convergent validity when measured during ramped cycling to exhaustion, resting recovery and daily living activities.15
Data analysis
For all analyses, we used modified intention to treat, which we defined as including all randomised surgeons who received at least some amount of study intervention (cooling vest or no cooling vest) for each of 4 surgeries (100% participation rate). We summarised surgeons’ demographic information (table 1) and surgical characteristics (table 2) using appropriate summary statistics (ie, means±SD, medians (Q1, Q3), or N (%)). Balance between cooling vest and no cooling vest surgeries on potentially confounding variables (ie, the preoperative factors in table 2) was assessed by absolute standardised difference (ASD), defined as the absolute difference in means, mean ranks or proportions divided by the pooled SDs. Imbalance was defined as ASD>0.358 (1.96 × ) (Austin, 2009).16 We planned a priori to consider adjusting for imbalanced baseline variables in all analyses (table 1).
) (Austin, 2009).16 We planned a priori to consider adjusting for imbalanced baseline variables in all analyses (table 1).
Demographic characteristics of surgeons
Characteristics of surgery by treatment group
Primary outcome
We assessed the treatment effect of the cooling vest versus no cooling vest on surgeons’ thermal comfort using a repeated measures linear model including variables for treatment, sequence (ie, the randomised cross-over pattern for each surgeon; AABB, BBAA, ABBA, BAAB) and period (first, second, third, fourth), and accounting for the within-subject correlation across periods using an autoregressive first-order (AR (1)) correlation structure. The cross-over sequence used was optimal in several ways because (1) each treatment appears the same number of times within each sequence and within each period and (2) the first-order carryover effects precede every other treatment the same number of times.12 We tested for evidence of a differential carryover effect by assessing the treatment-by-period interaction. If no interaction was detected, we planned to remove the interaction and assess the treatment effect in a main effects model. As well, the intervention and control groups were well balanced on the number of temperature measurements as a surrogate for length of the case, in each primary and secondary analysis we adjusted for this variable to avoid any confounding bias due to length of the case.
Sensitivity analysis
Since the thermal comfort outcome can be considered to be ordinal, we conducted a sensitivity analysis using a generalised estimating equation (GEE) proportional odds model with robust variance while modelling the within-subject serial correlation using an independence correlation structure.
Secondary outcomes
We assessed the treatment effect of the cooling vest versus the control condition of the surgeons’ average across (1) mean skin temperature and (2) core body temperature, each using a repeated measures linear model to account for correlation across the four periods within each surgeon as in the analysis of the primary outcome.
Second, we fit a repeated measures linear model on the individual continuously measured temperatures during surgery (not average for the case) assuming a compound symmetry correlation matrix and testing the three-way interaction between treatment, period and time, as well as two-way interactions among these factors. Since there was an evidence of treatment-by-period interactions, we reported the treatment effects collapsing over period as in the primary analysis but also within each period.
Sensitivity analysis
Since approximately 15% of the 120 surgeries lasted longer than 150 min, we truncated the temperature analysis after 150 min to eliminate a potential bias of a reduced cooling effect in longer surgeries. We then estimated treatment effect as in the above analysis.
Third, we assessed the effect of the cooling vest versus no vest on surgeons’ measure of cognitive performance using a repeated measures linear model as in the primary analysis, but adjusting for preoperative cognitive performance.
Finally, we assessed the effect of the cooling vest versus no vest on surgeons’ perceived exertion (Borg scale) using a GEE proportional odds model for the ordinal outcome with robust variance while modelling the within-subject serial correlation using an independence correlation structure. We also tested the treatment-by-time interaction. We assessed the treatment effect on surgeons’ perception of sweat-soaked clothing and perceived rating-of-fatigue, each using a repeated measures linear model to account for correlation across the four periods within each surgeon as in the analysis of the primary outcome.
Sensitivity analysis
Since the proportional odds assumption appeared to be violated in the GEE model for surgeons’ perceived ergonomic workload, we also fitted a repeated measures linear model for this outcome, accounting for correlation across the four periods within each surgeon.
Sample size justification
Sample size was estimated for 90% power at 0.05 significance level to detect a difference of 2 or more (on a scale of 0–10) on surgeons’ self-rated thermal comfort with vs without a cooling vest. With an estimate SD of 3 for thermal comfort in each of the intervention and control conditions, and an assumed within-subject correlation of 0.5 between intervention and control outcomes, the estimated SD of the within-subject difference would be 3.0, and at least 26 participants (ie, intervention and control pairs) were needed based on a paired t-test, an appropriate simplification compared with the used repeated measures analysis.
We conservatively recruited 30 surgeons. Our power was further increased because each provider was studied during 4 surgeries instead of 2 by virtue of our 4-period cross-over design, for a total of 60 intervention versus control pairs in the analyses. Even assuming a much smaller within-subject correlation of 0.10, 47 pairs would be necessary whereas our trial actually had 60. The detectable difference corresponds to an effect size (Cohen’s D) of 0.66, which is medium. For the 3 secondary outcomes using a significance criterion of 0.05/3=0.017, we would have 90% power to detect an effect size of 0.76. Without previous access to data or analysis, we increased the sample size to 30 surgeons to account for potential drop-outs. SAS statistical software V.9.4 was used for all analyses.
Results
We enrolled 30 surgeons, each participating during four operations, for a total of 120 surgeries. Surgeons were randomly assigned to one of the four different treatment sequences (AABB, BBAA, ABBA, BAAB). Surgeons’ demographic information is reported in table 1 and surgery characteristics in table 2.
Primary outcome
Comparisons of surgeons’ self-rated thermal comfort scores (0–10 Likert scale, with 5=comfortable) are presented in table 3. The cooling vest significantly reduced the surgeons’ mean thermal scores in a repeated-measures linear model across the 4 periods while, after adjusting for baseline thermal comfort, with mean (SE) of 4.5 (0.19) for cooling vest and 6.6 (0.19) for no-cooling vest, and estimated difference in means (cooling vest minus no-cooling vest) of −2.1 (95% CI −2.7 to –1.6) points, p<0.001, table 3. No treatment-by-period interaction was found (p=0.94), implying no evidence of differential carryover effect, an important assumption for a cross-over trial.
In our sensitivity analysis considering the thermal comfort scores to be ordinal, median (quartiles) of 4 (3.5, 5) for cooling vest and 7 (6, 7) for no-cooling vest were observed, with estimated proportional OR for having a lower (better) thermal comfort score in cooling vest versus no-cooling vest of 16 (7, 39), p<0.001 (table 3.)
Secondary outcomes
The case-average mean of skin temperature differences in means were lower with the cooling vest than without, −0.23 (95% CI −0.40°C to –0.06°C), p=0.011 (table 3 and figure 1). There was no evidence of a treatment effect for the cooling vest for the case-average mean of core body temperature, with estimated difference in means of −0.13 (95% CI (−0.33°C to 0.07°C), p=0.194 (table 3 and figure 2). Individual patient temperature profiles over time are given in online supplemental figures 1,2
Supplemental material
Supplemental material
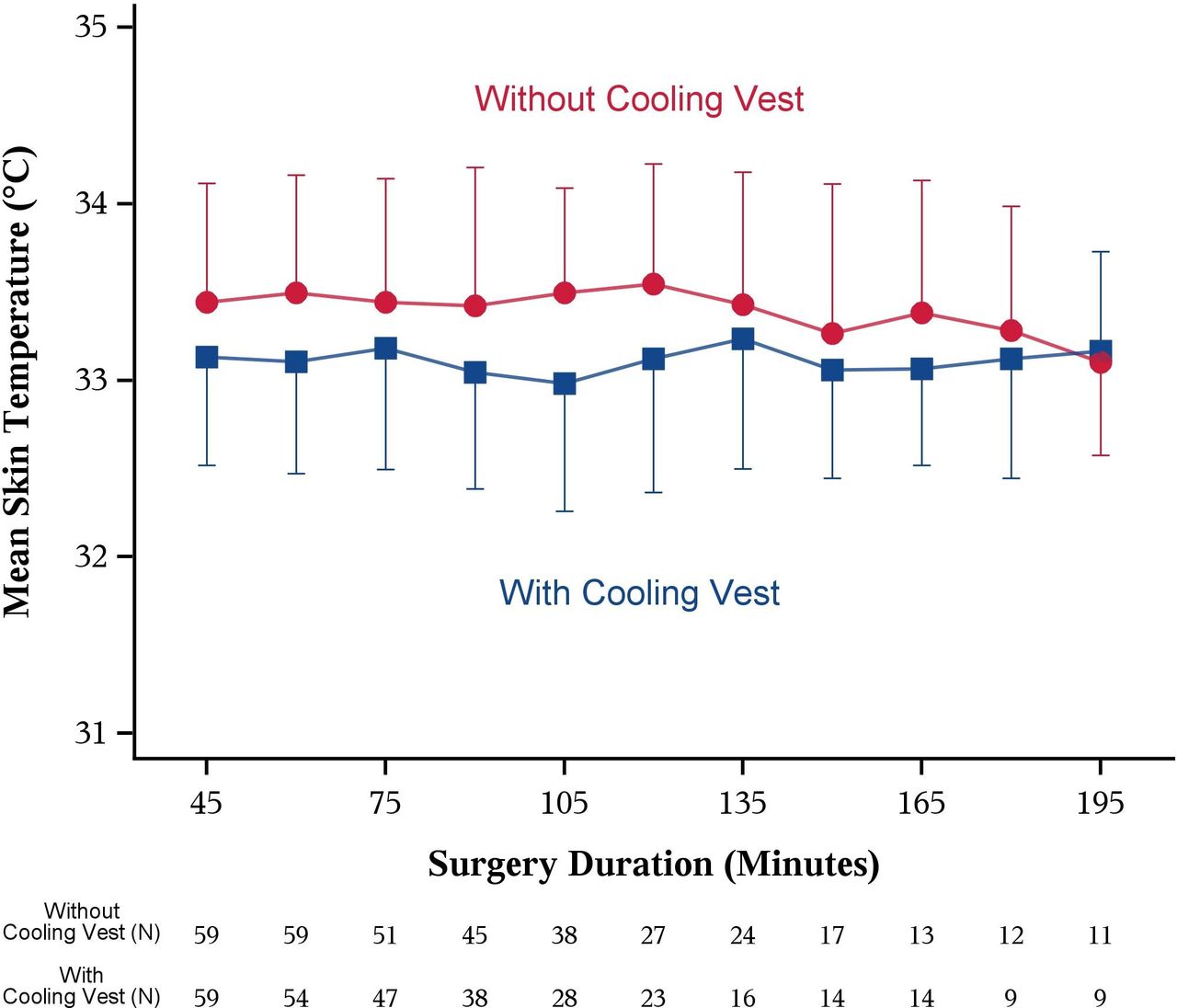
Mean skin temperature over time by treatment. Data points represent means±SDs of mean skin temperature for a case, ignoring surgeon and period.

{kind=link}
{kind=link}
Core body temperature over time by treatment. Data points represent means±SDs of mean skin temperature for a case, ignoring surgeon and period.
Treatments effect on the primary and secondary outcomes measured once per period (N=120 surgeries, 30 surgeons)
In sensitivity analyses, skin and core temperatures were analysed using continuously measured (repeated-measures) data for a case as the outcome. Three-way and two-way interactions across treatment, period and time are presented in online supplemental table 1. For mean skin temperature, the treatment-by-period (p=0.006) and treatment-by-time (p=0.006) interactions were significant, but not the three-way interaction (p>0.99) or period-by-time interaction (p=0.88). As for core body temperature, the treatment-by-period (p<0.001) was significant. The sensitivity analysis gave similar results (online supplemental table 1, rows 3 and 4).
Supplemental material
Because treatment-by-period interactions were found for both outcomes, we assessed the treatment effect collapsing across periods as well as within period (online supplemental table 2A). The cooling vest significantly reduced the mean of mean skin temperature collapsing over periods (difference in means of −0.19 (−0.25°C to –0.13°C), p<0.001, and particularly in the second and third periods, with an estimated difference in means (vest minus no vest) of −0.30 (95% CI −0.46°C to –0.14°C; p<0.001) and −0.41 (95% CI (−0.57°C to −0.25°C; p<0.001). The cooling vest reduced overall mean core body temperature (−0.14 (95% CI −0.20°C to –0.08°C) and in the first, third and fourth periods, with an estimated difference in means (vest minus no vest) of −0.18 (95% CI (−0.32°C to −0.02°C), p=0.022, –0.30 (95% CI −0.45°C to –0.15°C), p<0.001 and −0.21 (95% CI −0.36°C to –0.06°C), p=0.005. The sensitivity analyses gave similar results (online supplemental table 2B).
Supplemental material
There was no evidence of a treatment effect for the cooling vest for either of the two cognitive performance outcomes (table 3), with estimated difference in means of 0.03 (95% CI −2.44 to 2.51), p=0.979, for the PST and 0.88 (95% CI −2.25 to 4.01), p=0.569, for VMT. Finally, the cooling vest also reduced surgeons’ perception of sweat-soaked clothing with estimated difference in means of −2.9 (95% CI −3.7 to –2.1), p<0.001 as well as their perceived rating of fatigue with a difference in means of −0.95 (95% CI −1.6 to –0.28), p=0.007 (table 3). Surgeons’ perceived ergonomic workload was also lower with the cooling vest versus no cooling vest, with the estimated proportional OR of 2.3 (95% CI 1.2 to 4.5), p=0.019, estimating that vest wearers were 2.3 times more likely to have a lower (better) score. The sensitivity analysis for perceived ergonomic workload using a linear mixed effects model provided similar results, with estimated mean difference of −0.78 (95% CI −1.5 to –0.09), p=0.028 (table 3).
Discussion
Thermal comfort is strongly correlated with mean skin temperature,17 whereas autonomic thermoregulatory responses such as sweating and shivering are about 80% determined by core temperature.18–21 Across the skin surface, the upper chest and face are about twice as sensitive as other areas. Our results show that a conductive cooling vest worn by surgeons under PPE while performing surgery lowers skin and core body temperature and improves perceptions of thermal comfort, fatigue and exertion. However, cooling did not improve visual memory or processing speed.
Skin is remarkably sensitive to even tiny changes in temperature. Therefore, it is unsurprising that surgeons reported feeling cooler and sweating less while wearing the cooling vest. Their perceptual improvement for exertion and fatigue was presumably because the cooling vest reduced thermal strain. Prolonged physical exertion and fatigue in physically demanding environments can potentially lead to occupational injuries,22 although at temperatures considerably exceeding those experienced by surgeons. Improved thermal comfort with a cooling vest is consistent with studies conducted in real time2 23 and simulation24 and extends previous work by evaluating surgeons in a clinical environment.
Skin temperature of 32°C–33°C corresponds to a homoeostatic state with no apparent changes in cognitive performance; however, skin temperatures of 36°C and higher can impair cognitive performance, especially for complex tasks.25 It is thus unsurprising that surgeons’ mean skin temperatures near 33°C with and without the cooling vest did not alter cognitive performance.23 26 Our results are consistent with Morley et al who examined cognitive performance (memory, attention and reaction time) in fireman during simulated emergencies that prompted a rapid increase in body temperatures under protective clothing and found there were no immediate changes to cognition.27 These results support that fact that rapid increases in temperature under PPE are not high enough to impact cognitive performance. Preserved cognitive performance is reassuring for safe care provided to patients during surgical procedures. However, it remains possible that higher ambient temperatures in paediatric operating rooms could provoke sufficient thermal strain and discomfort to impair cognitive performance.26
Limitations
There are well-known circadian thermoregulatory variations. For example, core temperature varies nearly 1°C over the diurnal cycle, typically being lowest near 3:00 hours and highest near 15:00 hours.28 All of our surgeries took place during typical working hours between 7:00 and 17:00 hours when circadian changes in core temperature are usually small, and 76% began between 7:00 and 10:00 hours. The circadian variation in body temperature presumably exceeded the difference in core temperature induced by the cooling vest. Nonetheless, humans control core temperature to within a few tenths of a °C. Therefore, a 0.2°C difference in core temperature with and without the cooling vest is physiologically meaningful, as confirmed by the reported difference in thermal comfort. We note though that the treatment effect means of 0.2°C and 0.3°C fall within the range of measurement error for individual readings. However, the device’s accuracy is reasonable for multiple readings across multiple people with a measured bias of just 0.14°C.8
Surgeons performed the cognitive test once before the trial started and before and after each of four operations. Therefore, it is possible that learning improved their scores over time. However, our trial was randomised and our statistical analysis considered order and period. The 10-min cognitive test is based on three different modules with over 16 000 variations and it is doubtful that any of the patterns were repeated. It is thus unlikely that learning substantively influenced our results. Because the surgeons were not blinded to the actual cooling intervention, their expectations could potentially generate a placebo effect. However, the within-subject design was used to detect any real difference that might exist between the intervention and control conditions.
Our protocol did not exclude female surgeons. Although we would have welcomed women, none was available. Men and women’s responses to warm temperatures differ because female core body temperatures are typically 0.3°C higher, and because of cyclical effects of oestrogen and progesterone, and use of hormonal contraceptives, pregnancy and menopause.29 This study was conducted in real time during total-joint replacements with predictable operation times, similar physical demands and included surgeons of various ages, body size and varying levels of training. However, we planned a priori extensive within-subject analysis to adjust for imbalanced baseline variables. This allowed for sufficient control in a field study to ensure adequate internal validity to maintain a degree of realism. Our results thus appear generalisable over a range of similar operations requiring physical exertion, although future studies should include women.
Conclusion
Surgeons who wore a cooling vest during surgery reported improved thermal comfort, decreased sweating, less fatigue and less perceptual exertion. Objective measures showed that visual memory and processing speed was maintained, and that skin and core temperatures were lower while wearing the cooling vest. Therefore, while thermal discomfort during major orthopaedic surgery is largely preventable, cooling does not affect cognition.
Data availability statement
Data are available on reasonable request. The data that support the findings of this study are available from the authors, on reasonable request. It can be addressed to FAR-P (RODRIGF3@ccf.org), the project leader.
Ethics statements
Patient consent for publication
Ethics approval
This study involves human participants and was approved by Cleveland Clinic Institutional Review Board (IRB) Federalwide Assurance (FWA00005367) Study number: IRB 20-214. Participants gave informed consent to participate in the study before taking part.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Twitter @OutcomesRC
Contributors JEB designed the study and acquired funding to conduct the research, wrote the original draft and provided substantive revisions to the manuscript; JEB will act as the guarantor for the paper. FAR-P conducted the research, wrote the original draft, reviewed and edited the manuscript, and provided substantive revisions to the manuscript. YH and EJM provided an extensive formal analysis and interpretation of the findings, wrote the original draft, and offered substantive revisions to the manuscript. MB conducted blinded data entry and commented on the manuscript. MRB contributed to the design and commented on the manuscript. SMR contributed the battery assessment, gave input to interpretation of the findings and provided substantive revisions to the manuscript. DIS contributed to the design, interpreted the findings, wrote the original draft and provided substantive revisions to the manuscript.
Funding This investigator-initiated study was funded by Cardinal Health (Dublin, Ohio, USA).
Disclaimer The funders had no role in conducting this study, in the writing of the report, or in the decision to submit the article for publication. All inferences, opinions, and conclusions drawn in this report are those of the authors and do not reflect those of the funding agency.
Competing interests SMR receives royalties regarding the C3B software. JEB receives royalties regarding the CoolSource Cooling system and as a co-principal investigator, an investigator initiated study grant was received from Cardinal Health to study the CoolSource Cooling System. No other authors have any competing interests.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.