Article Text

Abstract
Objectives To assess the impact of the COVID-19 pandemic on sick leave among healthcare workers (HCWs) in primary and specialist care and examine its causes.
Methods Using individual-level register data, we studied monthly proportions of sick leave (all-cause and not related to SARS-CoV-2 infection) from 2017 to February 2022 for all HCWs in primary (N=60 973) and specialist care (N=34 978) in Norway. First, we estimated the impact of the pandemic on sick leave, by comparing the sick leave rates during the pandemic to sick leave rates in 2017–2019. We then examined the impact of COVID-19-related workload on sick leave, by comparing HCWs working in healthcare facilities with different levels of COVID-19 patient loads.
Results HCWs had elevated monthly rates of all-cause sick leave during the COVID-19 pandemic of 2.8 (95% CI 2.67 to 2.9) and 2.2 (95% CI 2.07 to 2.35) percentage points in primary and specialist care. The corresponding increases for sick leave not related to SARS-CoV-2 infection were 1.2 (95% CI 1.29 to 1.05) and 0.7 (95% CI 0.52 to 0.78) percentage points. All-cause sick leave was higher in areas with high versus low COVID-19 workloads. However, after removing sick leave episodes due to SARS-CoV-2 infections, there was no difference.
Conclusions There was a substantial increase in sick leave among HCWs during the pandemic. Our results suggest that the increase was due to HCWs becoming infected with SARS-CoV-2 and/or sector-wide effects, such as strict infection control measures. More differentiated countermeasures should, therefore, be evaluated to limit capacity constraints in healthcare provision.
- COVID-19
- Sick Leave
- Health Personnel
Data availability statement
Data may be obtained from a third party and are not publicly available. The dataset of this study was the Emergency Preparedness Register for COVID-19 (Beredt C19), a strictly regulated register available to selected authorised researchers in Norwegian Institute of Public Health. The individual-level data that support the findings is thus not publicly available due to privacy laws. However, the data are accessible to authorised researchers after ethical approval and application to 'helsedata.no/en' administered by the Norwegian Directorate of eHealth.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
WHAT IS ALREADY KNOWN ON THIS TOPIC
Several studies reported on increased levels of sick leave, burn-out, mental health problems and plan of quitting among healthcare workers during the COVID-19 pandemic.
Many healthcare facilities experienced substantial capacity constraints during the COVID-19 pandemic.
WHAT THIS STUDY ADDS
The impact of the COVID-19 pandemic on sick leave among healthcare workers in Norway was substantial.
The impact was greater in areas with high COVID-19-related workloads compared with areas with low COVID-19-related workloads.
The increase in sick leave in areas with high COVID-19-related workloads was primarily due to SARS-CoV-2 infections and/or sector-wide strict infection control measures.
HOW THIS STUDY MIGHT AFFECT RESEARCH, PRACTICE OR POLICY
During periods with substantial variation in infection rates across geographical areas, more differentiated countermeasures may be necessary to limit capacity constraints in healthcare provision.
Introduction
Healthcare workers (HCWs) have played a crucial role in the response effort during the COVID-19 pandemic. However, the added workload and work-related stress during this period have been linked to elevated rates of burn-out, psychological problems and plans to quit.1–6 These findings align with research from previous novel viral outbreaks, for example, Severe Acute Respiratory Syndrome (SARS) and Middle East Respiratory Syndrome (MERS), finding increased psychological distress and burn-out among HCWs during a pandemic.7 8
In contrast to other recent viral outbreaks, the countermeasures introduced to limit the spread of the COVID-19 pandemic included comprehensive population-wide countermeasures, for example, strict quarantine and isolation requirements. Among the main reasons for these measures were ensuring sufficient capacity for medical treatment in a period of increasing demand.9 10 Although these measures limited the spread, they also restricted the availability of healthcare personnel, as many HCWs had to be isolated after becoming infected with SARS-CoV-2 or were quarantined due to close contact with infected individuals. Hence, the increase in sickness absence among HCWs during periods of high infection rates potentially also led to adverse health effects from additional work-related stress among those remaining at work.
While there have been some studies finding increased sick leave among HCWs during the COVID-19 pandemic,11–13 population-wide longitudinal evidence on the impact of increased COVID-19-related workload is lacking. Improved knowledge of the mechanisms underlying increased sickness absence among HCWs during the pandemic, and its different phases, may be important for the development of public health policies, for example, when facing new variants of SARS-CoV-2 or other viral outbreaks.
The objective of this study was to assess the impact of the COVID-19 pandemic on sick leave among HCWs in primary and specialist care and examine its causes. More specifically, we aimed to (1) present estimates of the impact of the pandemic on all-cause sick leave and sick leave not related to SARS-CoV-2 infection among HCWs in primary and specialist care in Norway and (2) examine how the impact varied between healthcare facilities with high and low COVID-19-related workloads.
Methods
Study design and data sources
The study was designed as a register-based observational study using data from BEREDT C19 (BC19), a population-wide emergency preparedness register established to provide rapid knowledge about the COVID-19 pandemic.14 BC19 is a linked individual-level database with data on demographics (The National Population Register), primary care utilisation from general practitioners and emergency wards (Norway Control and Payment of Health Reimbursement, KUHR), specialist care utilisation (Norwegian Patient register), SARS-CoV-2 infections (the Norwegian Surveillance System for Communicable Diseases) and employment data (the Employer and Employee register).
Our study population included all Norwegian residents who in January 2020 were between 30 and 55 years old and had an active employment contract as a HCW. The HCWs were followed each month from January 2017 to January 2022 (37 564 persons; 63 months per individual; 2 366 532 person-months in total). Individuals who died or emigrated during the study period were censored from the month of death or emigration and onwards. HCWs were identified by their occupational code in the employment data, and separated into working in primary and specialist care by the employer’s industrial classification code (see table 1 for specific codes). Within specialist care, we only included employment contracts from public hospitals (identified by the organisation number), corresponding to 99.2% of the employees within specialist care. If an employee was registered with more than one active employment contract, we selected the employment contract with the latest starting date. Online supplemental figure A1 provides a graphical presentation of the sampling procedure.
Supplemental material
Descriptive statistics for workers in primary and specialist care, and HCWs working in healthcare facilities with high and low COVID-19-related workload
Outcomes
Our outcome of interest was doctor-certified sick leave from 2017 to early 2022. Sick leave was identified by its unique reimbursement code used by physicians in primary care (code L1). In addition, because Norwegian law required workers with a positive test to stay at home in isolation,15 we also defined a sick leave event if an individual had positive SARS-CoV-2 test.
To assess whether potential increases in sick leave were caused by SARS-CoV-2 infection (isolation or quarantine), or other health problems, we separated between all-cause sick leave and sick leave not related to SARS-CoV-2 infections. To achieve this, we identified sick leave directly related to SARS-CoV-2 infection or quarantine as sick leave (L1) coded with the International Classification of Primary Care (ICPC-2) codes for detected/suspected COVID-19 (R991 and R992) and/or quarantine (A23), and/or a positive SARS-CoV-2 test the given month. Sick leave that was not coded with any of these ICPC-2 codes (R991, R992, A23) or a positive SARS-CoV-2 test, was defined as sick leave not related to SARS-CoV-2 infections. For the few cases where individuals were registered with both an event of sick leave directly related to COVID-19 and an event with sick leave not related to SARS-CoV-2 infection in the same month (0.83% of monthly sick leave events), we coded it as sick leave not related to SARS-CoV-2 infection.
All outcome variables were defined as one if the individual was registered with the given type of sick leave (all-cause or not related to COVID-19) the given month, and zero otherwise. All Norwegian employees are mandatory members of the national sick leave insurance scheme, which ensures full reimbursement of earnings lost due to sickness up to a generous ceiling and limited to 1 year.
Exposure
The workload of HCWs due to COVID-19-related consultations and hospitalisations varied significantly across the different regions in Norway. The spread of the SARS-CoV-2 virus was generally higher in densely populated areas, leading to a higher COVID-19-related workload for HCWs working in these areas. We used this variation to assess to what extent a higher COVID-19-related workload was associated with higher sick leave among HCWs.
The measure of COVID-19-related workload for a HCW was defined as the share of total activity that was related to treating COVID-19 patients at the healthcare facility where a HCW was working. For HCWs in primary care, the measure was defined as the average share of COVID-19-related consultations (ICPC-2: R911, R992, A23) among the primary care providers in the municipality (ie, COVID-19-related consultations/total amount of consultations) (figure 1A). For HCWs in specialist care, we used the share of COVID-19-related hospital days (ICD-10 code: U071) at the hospital where the HCW was employed (ie, COVID-19-related hospital days/total amount of hospital days) (figure 1B). Our exposure captures workload due to the treatment of COVID-19 patients, and does not account for workload related to additional infection control measures implemented across the healthcare sector during the pandemic.

The distribution of the COVID-19-related workload across HCWs in primary and specialist care. The quintiles (1st, 2nd– 4th and 5th) of the COVID-19-related workload are indicated by colours. Panel (A) shows COVID-19 consultations for HCWs in primary care. Workloads were assigned based on the share of COVID-19-related consultations in the municipality in 2020 and 2021 (y-axis). Workers were ordered from low to high COVID-19-related workload (x-axis). Panel (B) shows COVID-19-related hospital days for HCWs in specialist care. Workloads were assigned according to their health trusts. Workers were ordered from low to high COVID-19-related workload (x-axis). HCWs, healthcare workers.
To examine the impact of COVID-19-related workload during the pandemic, we divided HCWs into two groups: low and high COVID-19-related workload, operationalised by the first and fifth quintile (lowest and highest 20%) of COVID-19-related activity, based on the healthcare facility where they worked. The use of quintiles for grouping was partly arbitrary, and we, therefore, present robustness checks of the main results using tertiles and a median split—see online supplemental figure A5,A6. The quintiles were created by ranking HCWs according to the COVID-19-related workload from low to high, separately for HCWs in primary and specialist care. HCWs among the first 20% (first quintile), that is, with the lowest COVID-19-related workload, were then assigned to the low COVID-19-related workload group (Q1). Workers among the highest 20% (fifth quintile) were assigned to the high COVID-19-related workload group (Q5) (figure 1). The remaining HCWs (2nd–4th quintile) were not included in the parts of our analysis where these groups are used. All HCWs in the same municipality or health trust were assigned to the same quintile. Therefore, the sizes of the quintiles do not reflect exactly 20% of the working population (figure 1). See online supplemental table A1 for descriptive statistics on the high and low exposure groups, and online supplemental figure A2 for how COVID-19-related activity varied over time.
Statistical analyses
First, to assess the overall impact of COVID-19 on all-cause sick leave and sick leave not related to SARS-CoV-2 infections, we estimated and plotted monthly rates of sick leave working in primary and specialist care, for the years 2017–2019, 2020, 2021 and early 2022. The rates were calculated as the number of employees with at least one doctor-certified sick leave registration in each month, divided by the total number of employees. Second, we examined how the impact varied with different levels of COVID-19-related workloads. This was done by comparing the monthly sick leave rates—all-cause and not related to SARS-CoV-2 infections—between HCWs exposed to low vs high COVID-19-related workload. This was operationalised by the first and fifth quintile, and using the period 2017–2019 within each exposure group as a reference. By comparing the low and high exposure groups over time, we were able to account for both potential time trends in sick leave prior to COVID-19 and potential differences between the low and high exposure groups that existed prior to the pandemic.
All means and models were estimated on individual level data, that is, following the same individuals over the whole period. This strategy mitigates potential bias from changes in sample composition over time, a common concern in repeated cross-sectional studies. We estimated all confidence intervals using standard errors clustered on the level of the individual, to account for within-person correlation across time. All analyses were run in STATA MP V.16 and R V.4.02.
Results
Table 1 presents summary statistics for our sample. We studied primary care workers ( N =60 973) and specialist care workers ( N =34 978). The majority of our sample consisted of women, 87% in primary care and 79% in specialist care, with an average age of 42.1 in primary care and 41.2 in specialist care at the onset of the pandemic. Specialist care had a considerably higher share of physicians or nurses compared with primary care (91% vs 37%). This difference reflects that primary care supply consists of a substantial group of health professionals (42%) and personal care workers (21%), which typically are involved in caring for the elderly (table 1).
Sick leave before and during the COVID-19 pandemic
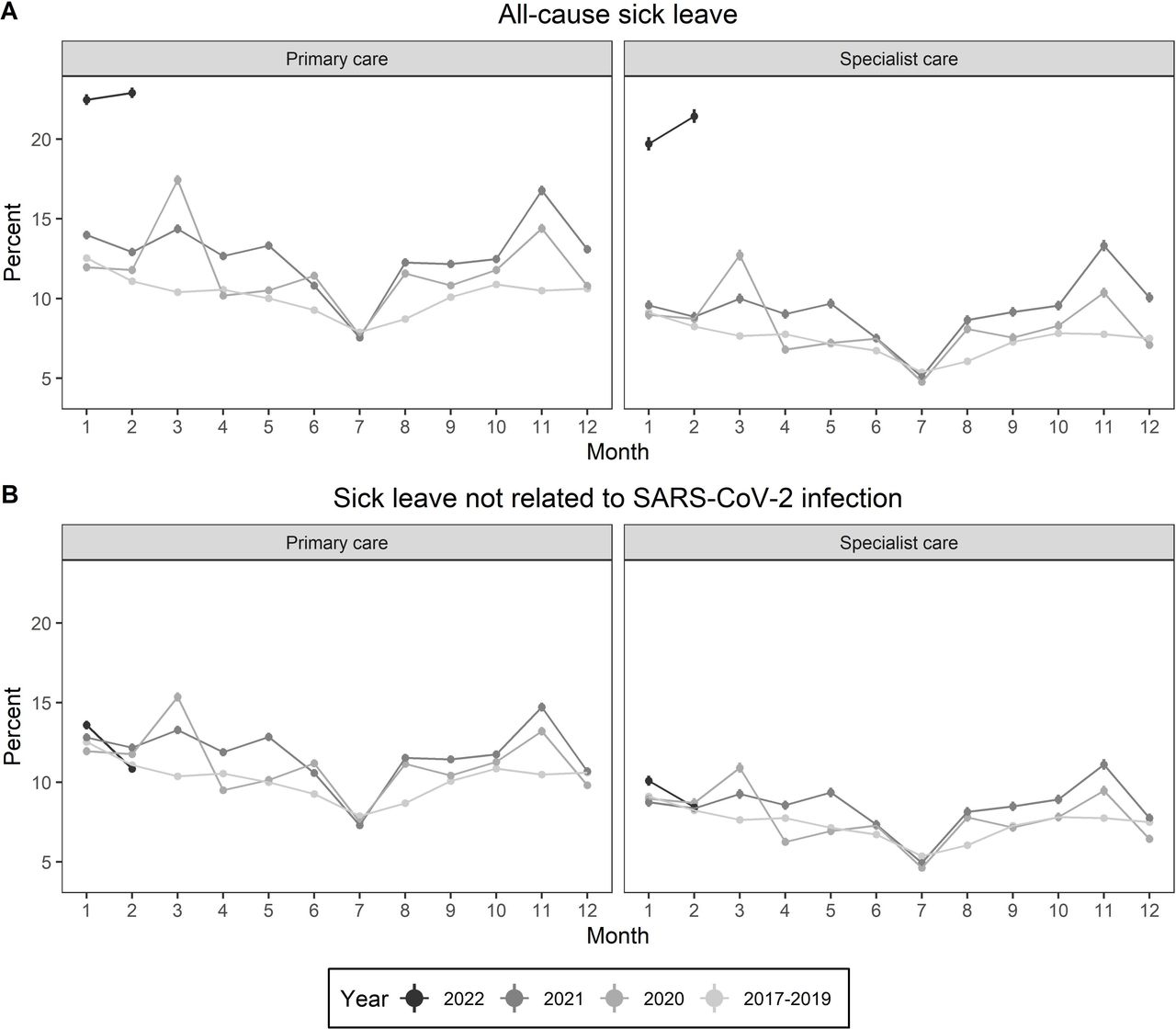
The rates of all-cause sick leave were substantially elevated during the pandemic compared with previous years. Compared with the rates in the corresponding months of 2017–2019, the average monthly increase in all-cause sick leave during the pandemic was 2.8 (95% CI 2.67 to 2.9) and 2.2 (95% CI 2.07 to 2.35) percentage points in primary and specialist care, respectively (online supplemental table A2). There was a particularly strong increase in all-cause sick leave during the fall of 2021 and early 2022 (figure 2A), for example, in February 2022, the rates were 22.9% in primary care and 21.5% in specialist care, compared with 11.1% and 8.2% in 2017–2019 (online supplemental table A3). For sick leave not related to SARS-CoV-2 infections (figure 2B), the average monthly increases during the pandemic were 1.2 (95% CI 1.29 to 1.05) and 0.7 (95% CI 0.52 to 0.78) percentage points in primary and specialist care, respectively (online supplemental table A2).

Monthly all-cause sick leave rates (A) and sick leave not related to SARS-CoV-2 infections (B) with corresponding 95% CIs in primary and specialist care for the years 2017–2019, 2020, 2021 and early 2022. See online supplemental table A2 for corresponding tables.
COVID-19-related workload and sick leave
All-cause sick leave rates among HCWs with low and high COVID-19-related workloads followed similar trends prior to the pandemic (figure 3A, online supplemental table A4). The average monthly difference between HCWs with low and high COVID-19-related workload from January 2017 to February 2020 was 0.96 (95% CI 0.66 to 1.27) percentage points in primary care, and 0.63 (95% CI 0.31 to 0.95) percentage points in specialist care. However, during the pandemic, the corresponding differences were 2.02 (95% CI 1.64 to 2.39) and 1.05 (95% CI 0.66 to 1.44) percentage points, respectively. The change in this difference was statistically significant both in primary and specialist care (p<0.001 and p=0.028). The strongest increase was in January 2022. For HCW in primary care, the sick leave rates were 18.1 in areas with a low COVID-19-related workload and 26.64 in areas with a high COVID-19-related workload (figure 3A), that is, the all-cause sick leave rate was 8.55 percentage points higher in areas with high COVID-19-related workload (figure 3B). The corresponding difference for HCWs in specialist care was 5.15 percentage points. In our alternative exposure measurements, where we split HCWs into high and low COVID-19 workload based on tertiles and the median, the difference in all-cause sick leave between HCWs with high and low COVID-19 workloads is smaller (online supplemental figures A5,A6). This is as expected, as the difference in average workload in the different groups is smaller when the exposure measurement is based on a weaker contrast.
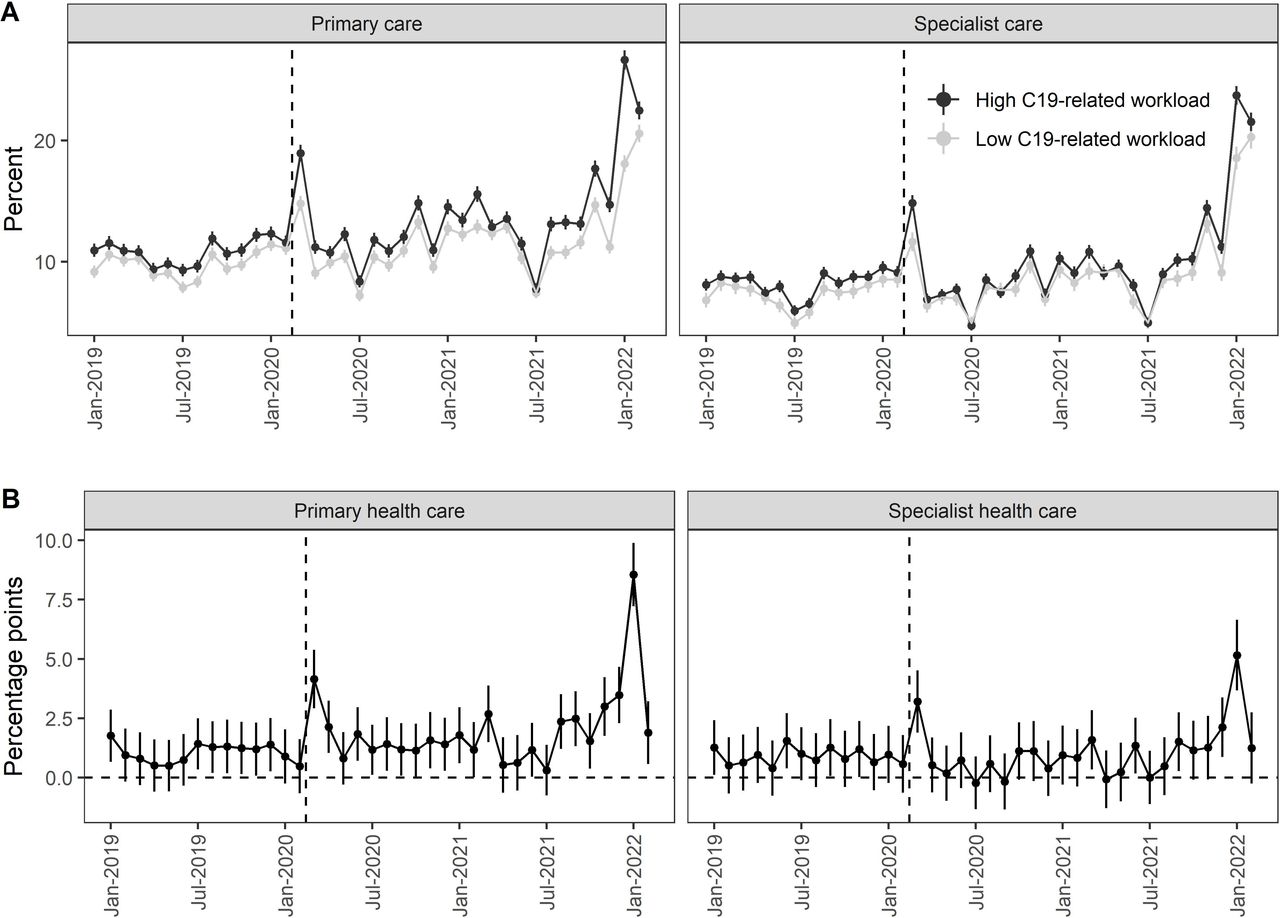
Monthly all-cause sick leave rates in primary and specialist care. (A) shows monthly rates of all-cause sick leave from 2019 to February 2022, for HCWs in health facilities with high and low COVID-19-related workload. (B) shows the difference between them. See online supplemental figure A3 for a 2017–2019 preperiod. HCWs, healthcare workers.
COVID-19-related workload and sick leave not related to SARS-CoV-2 infections
After excluding sick leave related to SARS-CoV-2 infections, there were not clear differences between healthcare providers with a high and low COVID-19-related workload (figure 4, online supplemental table A5), both before and during the pandemic. Since there was no SARS-CoV-2 related sick leave prior to the pandemic, the average monthly difference prior to the pandemic was the same as the difference in all-cause sick leave as described above. During the pandemic, the difference between HCWs with low and high COVID-19-related workload was 0.83 (95% CI 0.46 to 1.2) percentage points in primary care, and 0.24 (95% CI −0.14 to 0.62) percentage points in specialist care. However, compared with the difference between the high and low exposure groups prior to the pandemic, the difference in sick leave during the pandemic was not significantly higher within primary care (p=0.49), while in specialist care there was a significant reduction (p=0.038) (figure 4B).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Monthly rates of sick leave not related to SARS-CoV-2 infection in primary and specialist care. (A) shows monthly rates from 2019 to February 2022, for HCWs in health facilities with high and low COVID-19-related workload. (B) shows the difference between them. See online supplemental material for a 2017–2019 preperiod. HCWs, healthcare workers.
Discussion
In a study of 95 951 HCWs in Norway from 2017 to February 2022, we found significant increases in all-cause sick leave rates and sick leave not related to SARS-CoV-2 infections during the pandemic. The increases were particularly strong in primary care, and during the later phases of the pandemic. The increase in all-cause sick leave was especially high in February 2022 with relative increases of 106.3% (from 11.1% to 22.9%) and 162.3% (from 8.2% to 21.5%) in primary and specialist care, respectively (figure 2). HCWs in areas with a high COVID-19-related workload had a stronger increase in sick leave than HCWs in areas with a low COVID-19-related workload. This difference in increase by area was not observed when excluding sick leave related to COVID-19 from the analyses.
Comparison to previous studies
To our knowledge, our study is the first to compare the development in sick leave between healthcare facilities with different levels of COVID-19 workloads, prior to and during the pandemic, covering both primary and specialist care. While previous studies on sick leave among HCWs during the pandemic have been based on limited samples or time periods,11–13 this study includes all HCWs working in publicly provided primary and specialist care over a 5-year period (2017–2022). As such, our study sheds important new light to a recent register-based study performed in the UK, covering the period 2019–2020 (1.5 year) only. Excluding sickness absence due to SARS-CoV-2 infections, the UK study finds an overall decrease of 21.5% in sickness absence during the early phase of pandemic among HCWs employed by the National Health Service trusts (weeks 11–20). However, substantial increases were found for absence due to infectious diseases, respiratory problems and mental illness. Our study finds that while sick leave related to SARS-CoV-2 infections likely were the main cause of increased sick leave during the pandemic, there was a significant increase in sick leave not related to SARS-CoV-2 infections (1.18 percentage points in primary care and 0.65 percentage points in specialist care). These increases were stronger in primary care and during later phases of the pandemic, highlighting the importance of considering primary care and a longer time period in understanding the impact of the pandemic on sick leave among HCWs. The differences in findings between these studies can be attributed to various factors, including the duration of the study period, differences in infection rates, and the institutional setting, such as job security and compensation.
Other studies of HCWs during the pandemic, mostly based on convenience sampling and small sample sizes, found an increase in mental complaints, such as burn-out and depressive mood in HCWs during the COVID-19 pandemic.3–6 Although our sick leave measure cannot serve as a proxy for mental health, we found that the increase in sick leave could be attributed to a combination of SARS-CoV-2 infections and/or sector-wide factors, such as strict infection control measures and/or a general feeling of threat to the own safety when working as a HCW during this period. Hence, our study suggests that sector-wide factors, rather than the work-activity related to treatment of COVID-19 patients, may have been the more important source of increased work-related stress during the pandemic.
Strengths and limitations of this study
A strength of our study is the detailed individual-level administrative registers used to study developments in sick leave during the COVID-19 pandemic. By contrasting the development in areas with high and low COVID-19-related workloads, it allows for credible estimates of both the magnitude of the impact, and exploring the underlying mechanism. The sample is based on all active HCWs in the months before the pandemic, which could be interpreted as both a strength and weakness. A strength of this approach is that our analysis is not biased by changes in the sample composition over time—a typical challenge in repeated cross-sectional studies. A limitation is that it cannot inform about changes in the inflow and outflow of HCWs due to the pandemic. To minimise how this affects our results we only included HCWs aged 30–55, that is, excluding young HCWs that were likely to be students during the period of 2017–2019 and HCWs likely to retire during the pandemic. In addition, as Norway had a lower proportion of COVID-19 patients than most other countries,16 the external validity of our results is restricted to countries with similar COVID-19 infection rates and restrictions.
Another potential limitation is that when analysing the impact of COVID-19-related workload, we contrasted the first and fifth quintile of the distribution. The differences in all-cause sick leave between the high and low exposure groups would vary with how these groups are constructed, with larger differences when applying stronger contrasts and smaller differences when comparing, for example, above and below mean. In online supplemental material, we present results on all-cause sick leave using median split (online supplemental figure A5) or tertiles (online supplemental figure A6). As expected, the estimated differences between the groups are smaller, suggesting a dose–response relationship between our measure of COVID-19-related workload and impact on all-cause sick leave.
Finally, our measure of COVID-19-related workload was based on the share of treatment related to treating COVID-patients. Although this measure covers an important aspect of the additional workload among HCWs during the pandemic, it cannot clearly distinguish between causes that were general across all healthcare facilities. For example, the increased workload from sector-wide strict infection control measures. Also, there could be a sector-wide effect from the stress and uncertainty from being exposed to a high risk of infection when working as a HCW.
Policy implications
Our findings suggest that the health and work capacity of HCWs were severely affected by COVID-19. The impact of the pandemic on sick leave was twofold: a substantial increase in sick leave due to SARS-CoV-2 infections, but also an increase in sick leave related to other health conditions. This suggests that the prolonged and demanding nature of the pandemic had a comprehensive impact on the well-being of HCWs. Paradoxically, while strict countermeasures were periodically introduced to ensure sufficient capacity in the healthcare service, the strict quarantine requirements and infection prevention measures likely also contributed to additional sickness absence. Although the increase in sick leave among HCWs was substantial, we found that it was related to SARS-CoV-2 infections or sector-wide effects such as strict infection control measures, rather than increased workload from treating COVID-19 patients. Hence, our study stresses the need for more differentiated countermeasures, for example, by geographical region or type of HCW, to more efficiently protect healthcare capacity during high pandemic pressures.17
Conclusions
We found a substantial increase in sick leave among HCWs during the COVID-19 pandemic, especially in late 2021 and January 2022, and in areas with high COVID-19 patient loads.
Previous studies have found increased rates of burn-out and psychological problems among HCWs, causing concerns about the capacity of health service providers. This study finds that increased sickness absence among HCWs during the pandemic was not from treating COVID-19 patients, but rather related to HCWs becoming infected with SARS-CoV-2 and/or sector-wide effects, such as higher workloads due to strict infection countermeasures.
Data availability statement
Data may be obtained from a third party and are not publicly available. The dataset of this study was the Emergency Preparedness Register for COVID-19 (Beredt C19), a strictly regulated register available to selected authorised researchers in Norwegian Institute of Public Health. The individual-level data that support the findings is thus not publicly available due to privacy laws. However, the data are accessible to authorised researchers after ethical approval and application to 'helsedata.no/en' administered by the Norwegian Directorate of eHealth.
Ethics statements
Patient consent for publication
Ethics approval
This study involves human participants but the establishment of an emergency preparedness register forms part of the legally mandated responsibilities of The Norwegian Institute of Public Health (NIPH) during epidemics. The legal basis is the Norwegian Health Preparedness Act §2-4. Institutional board review was conducted by the Ethics Committee of South-East Norway, and the committee confirmed (4 June 2020, #153204) that external ethical board review was not required. We did not obtain verbal or written consent from the study population because the current study was based on routinely collected and anonymised register data. The law regulating official statistics in Norway implies that anonymised register data can be used for research. The law of statistics combined with the Ethics Committee of South-East Norway thus confirmed that informed consent was not necessary.
Acknowledgments
We thank the Norwegian Directorate of Health, particularly Olav Isak Sjøflot and his Department of Health Registries for their cooperation in establishing the emergencypreparedness register, and Gutorm Høgåsen and Anja Elsrud Schou Lindman for theirinvaluable work on the register.
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
B-AR and MG contributed equally.
Contributors B-AR and MG performed statistical analyses, drafted the manuscript. HG and KM contributed to drafting the article and critically revising it. All authors gave final approval for the version to be submitted. B-AR is responsible for the overall content as guarantor and accepts full responsibility for the finished work, and/or the conduct of the study, had access to the data, and controlled the decision to publish.
Funding The study was internally funded by the Norwegian Institute of Public Health.
Disclaimer The interpretation and reporting of the data are the sole responsibility of the authors, and no endorsement by the register is intended or should be inferred. The funding sources had no influence on the design or conduct of the study; collection, management, analysis, nor the interpretation of the data; preparation, review or approval of the manuscript; nor the decision to submit the manuscript for publication
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.