Article Text

Abstract
Background Though there is increasing evidence on the effect of long working hours (LWH) and stroke, few studies have distinguished stroke subtypes. We examined the associations between LWH and ischaemic or haemorrhagic stroke after adjusting for cardiovascular risk factors.
Methods From a national population-based cohort CONSTANCES, baseline questionnaires and initial health examinations were used to retrieve sociodemographic and cardiovascular risk factors from 2012 to 2018. LWH were defined as self-reported working time≥10 hours daily for at least 50 days per year. Incident cases of stroke were collected using International Classification of Disease codes recorded in the National Health Data System. Associations between LWH and stroke were investigated using multinomial models adjusted for cardiovascular risk factors.
Results Among the 160 751 participants who were free from stroke at baseline, exposure to LWH≥10 years was reported by 20 723 participants, and 190 incident cases of stroke were identified, including 134 ischaemic and 56 haemorrhagic. Exposure to LWH was associated with an elevated odds of ischaemic stroke (OR=1.61 (1.04–2.49)) and haemorrhagic stroke (OR=2.50 (1.38–4.53)) in unadjusted models. In adjusted multivariable models, only the LWH association with haemorrhagic stroke remained significant (aOR=1.92 (1.01–3.09)).
Conclusions LWH were associated with stroke, though it remained significant for haemorrhagic stroke only after adjustments. Differences in direct and indirect biological pathways and lack of power in the ischaemic subgroup may explain these results and further studies on the impact of mediating and effect measure modifying factors are needed. Nevertheless, policies that attenuate effects of both LWH and cardiovascular risks factor are warranted.
- Epidemiology
- Public health
- Longitudinal studies
- Occupational Stress
Data availability statement
Data may be obtained from a third party and are not publicly available. The data of the CONSTANCES cohort are protected by our national regulatory agency (‘Commission nationale de l’informatique et des libertés’, n°910486). However, the CONSTANCES cohort is ‘an open epidemiological laboratory’ and access to study protocols and data is available on reasonable request.
Statistics from Altmetric.com
WHAT IS ALREADY KNOWN ON THIS TOPIC
More than 400,000 deaths by stroke were estimated to be caused by long working hours (LWH) in 2016
Few studies have differentiated the effect of LWH on ischemic and hemorrhagic stroke while considering strong cardiovascular risk factors
WHAT THIS STUDY ADDS
Prolonged exposure to LWH was associated with increased stroke occurences in unadjusted models, but the association remained significant only for hemorrhagic stroke
Lack of power and differences in direct and indirect biological pathways may explain this result, with a predominant mediation by modifiable behaviours for ischaemic strokes
HOW THIS STUDY MIGHT AFFECT RESEARCH, POLICY OR PRACTICE
More studies, even underpowered ones, are needed to better understand the association between LWH, cardiovascular risk factors and stroke.
Better controls and interventions on both occupational exposures and lifestyle factors are needed to reduce the global burden of stroke.
Introduction
The effect of long working hours (LWH) on cardiovascular diseases has been widely documented.1 Systematic reviews and meta-analyses from the WHO/ILO (International Labor Organization) joint estimates of disease reported sufficient evidence of harmfulness associated with working more than 55 hours per week for stroke and ischaemic heart diseases.2 3 Though the strength of the association between LWH and stroke was moderate compared with other occupational exposures, the high prevalence of LWH lead to an estimated 400 000 deaths by stroke in 2016, with a population attributable fraction close to 7%.1 Stroke, however, is a broad term that conflates two different types of disease with different pathophysiology: ischaemic stroke is caused mainly by the clotting of a cerebral artery and haemorrhagic stroke is caused by the rupture of a cerebral artery.4 5 The WHO/ILO systematic review did not report enough information to differentiate the effect of LWH on risk of stroke subtypes. Among the reviewed studies, some reported a higher risk of haemorrhagic stroke.6 7 These studies, however, did not consider potentially strong confounding and effect measure modifying factors, such as diabetes and smoking, nor did they account for duration of exposure to LWH, which has been shown to influence the association between LWH and stroke.8 9 However, there is little evidence on the confounding factors on the relation between LWH and stroke. Thus, future models assessing the effect of LWH on stroke should at least include known cardiovascular risk factors and consider behavioural risk factors depending on their relevance.
To better understand the relationship between LWH and stroke, our aim was to examine a large population cohort for associations between LWH and incident cases of ischaemic and haemorrhagic stroke, while accounting for an array of cardiovascular risk factors.
Methods
Data origin
CONSTANCES (CONSulTANts des Centres d’Examens de Santé is a French population-based cohort created in 2012. Adults enrolled in the National Social Security system and aged 18–69 years were randomly selected. The cohort design and characteristics are detailed elsewhere.10 All participants underwent health screenings by medical professionals at Social Security affiliated centres and completed self-administered surveys that included ‘lifestyle’ and ‘occupational exposure’ questionnaires. Data from the cohort were linked to French National Health Insurance records to retrieve cases of stroke during the follow-up period (until 2018). These records are collected in the National Health Data System (SNDS), which evaluate all healthcare utilisation in our country.11
All working participants who completed the questionnaires during the data collection period (from 2012 to 2018) were included.
Variables of interest
From the self-administered questionnaires at baseline, we retrieved the following self-reported relevant variables: age (years), sex (female, male), smoking (never smoked, ever smoked<30 pack-years, ever smoked≥30 pack-years), occupational status using the French occupational and social classification system12 with the first digit (high-skilled white-collar jobs, self-employed/chief executive officer/professional jobs, low-skilled white-collar jobs, blue-collar jobs) and exposure to LWH. Exposure to LWH was defined as a working time>10 hours daily for at least 50 days per year. Participants also reported the number of years they were exposed. In the statistical analyses, exposure to LWH was categorised as <10 years and ≥10 years of exposure consistent with sensitivity analyses from previous findings.8 9
We retrieved data on history of stroke (all subtypes together) and age of occurrence, diagnosed diabetes (yes/no), diagnosed high blood pressure (yes/no), diagnosed dyslipidaemia, hypercholesterolaemia or hypertriglyceridaemia (yes/no), family history of cardiovascular events (yes/ no) and body mass index (BMI) (kg/m2) from the medical interview at baseline where physicians questioned participants on medical diseases and examined them.
Main outcome
Cases of stroke were retrieved via a linkage between the CONSTANCES data and the SNDS, which collects International Classification of Diseases-10 codes from all hospitalisation across the country. We retrieved the principal diagnosis that allowed us to categorise stroke as haemorrhagic (I60-61-62 except I604/I605/I621) or ischaemic (I63-64 except I63.6). Codes were chosen accordingly to a previous study on stroke in the SNDS.13 Only the first case of stroke after study inclusion was considered. Cases of stroke that occurred before participants filled out the baseline questionnaire were not included, as well as participants with a history of stroke were excluded.
Statistical analyses
Associations between LWH and stroke were examined using crude and adjusted multinomial logistic regression models. Multivariable models were adjusted for cardiovascular confounding variables, including age, sex, BMI, high blood pressure, diabetes, dyslipidaemia, familial history of cardiovascular disease and smoking, as well as occupation. We did not include alcohol in our final model because it was not significantly associated with stroke risk in the univariable analyses and because of potential risk of collinearity with other variables in the final model. Survival analyses were not chosen as the primary analyses because the focus of this study was the risk of stroke and not the time to event or when the stroke occurred, as we considered the life-time cumulative exposure. However, Cox regression models were run as sensitivity analysis . All analyses were performed using R software (V.4.0.4, packages compareGroups, EpiDisplay, survival).
Results
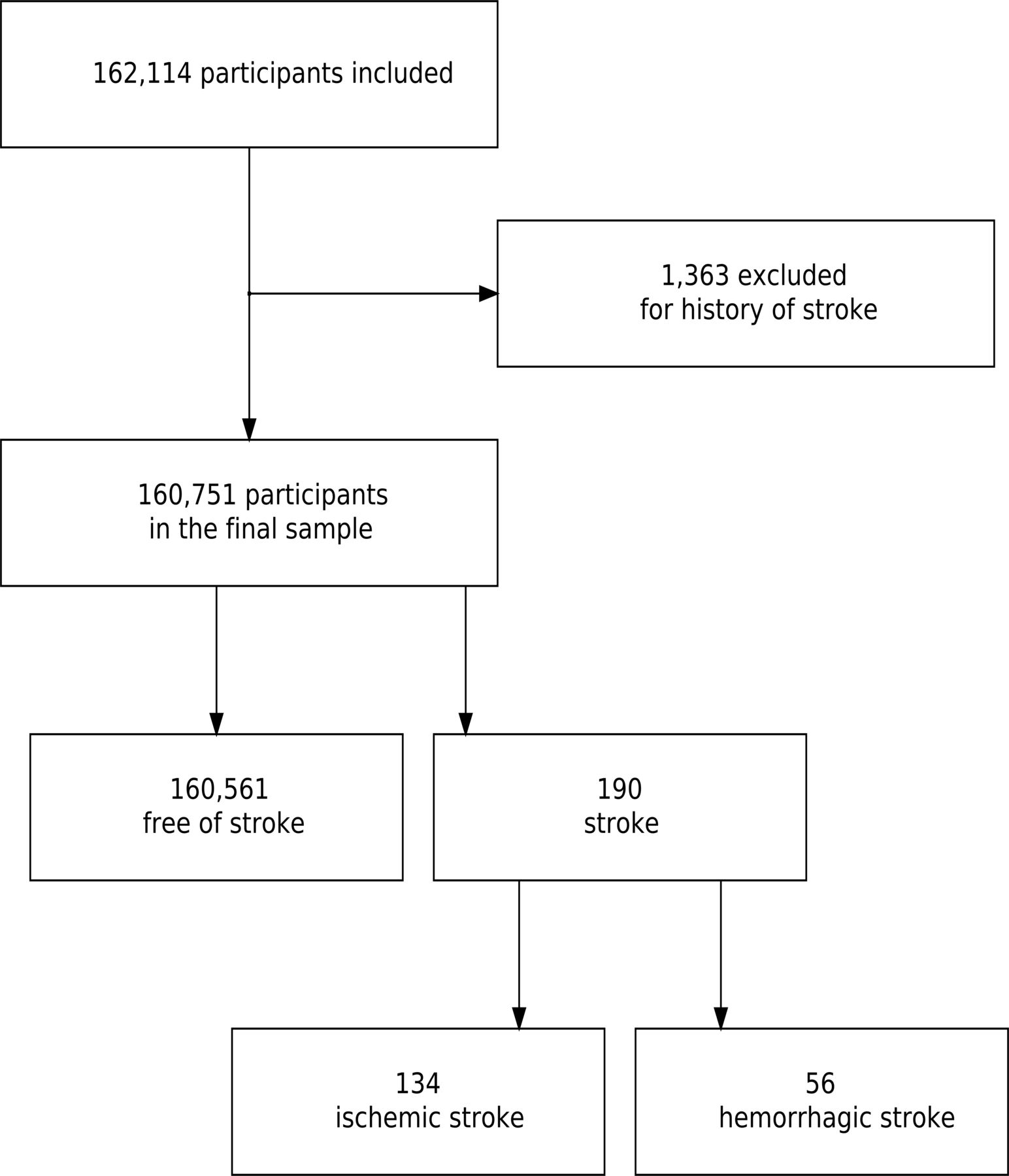
Figure 1 illustrate the sample studied from the initial population. From the years 2012 to 2018, 162 114 participants were eligible. After excluding 1363 participants from the study for having a history of stroke, the final sample size was 160 751 participants, free from stroke at baseline. A description of the population according to stroke subtype is presented in table 1. There were 20 763 participants (13.4%) who reported exposure to LWH for more than 10 years, and 190 incident cases of stroke (0.12%) comprising 134 ischaemic and 56 haemorrhagic strokes. Self-employed/chief executive officer/professional jobs were the most exposed to LWH (table 2), with a mean duration of exposure (5.49 years) contrary to low-skilled white-collar jobs, which had the least mean duration of exposure (1.65 years). The median for the time from last year of exposure reported to stroke event was of 7 years (mean 11.4 years), the median follow-up time was 3 years (IQR 2–5 years) and the median for time from inclusion to stroke event was of 2 years (IQR 1–3 years).

{kind=link}
Route diagram of the studied sample.
Description of the population according to stroke subtype
Exposure to long working hours according to occupation
In crude models, exposure to LWH was associated with an elevated odds of ischaemic stroke (OR=1.61 (1.04–2.49)) and haemorrhagic stroke (OR=2.50 (1.38–4.53)) (table 3). However, in adjusted multivariable models, statistical significance waned for LWH associations with ischaemic stroke (aOR=1.01 (0.63–1.63)) and remained significant for haemorrhagic stroke (aOR=1.92 (1.01–3.09)). Age, sex and diagnosed diabetes were significantly associated with ischaemic stroke, whereas only age and smoking were significantly associated with haemorrhagic stroke. Associations were similar when running Cox regression models (table 4). Exposure to LWH≥5 years (reference<5 years) was also associated with haemorrhagic stroke (aOR=2.33 (1.27–4.27)) but not to ischaemic stroke (aOR of 1.02 (95% CI, 0.66 to 1.58)).
Crude and adjusted multinomial logistic regression assessing association between long working hours and stroke
Crude and adjusted Cox regression models assessing association between long working hours and stroke
Discussion
Haemorrhagic stroke was associated with prolonged exposure to LWH after adjusting for cardiovascular risk factors.
These results are similar to findings in other epidemiological studies.6 Our study further distinguishes ischaemic and haemorrhagic stroke in the association with LWH, while accounting for an expansive array of cardiovascular confounders alongside number of years of LWH exposure. Both ischaemic and haemorrhagic stroke had significant associations in crude bivariate analyses but our study could find an association between ischaemic stroke and LWH in adjusted models. Lack of power may explain this difference as there were relatively few events. Another possible explanation is that the relation between the different risk factors and their influence on the association between LWH and stroke is different for ischaemic and haemorrhagic stroke. A predominant indirect pathway may exist for ischaemic stroke and thus, the effect of LWH may be mediated by modifiable behaviours. Several studies14 15 have shown that LWH are associated with negative health behaviours that are also known risk factors for ischaemic stroke.4 Elsewhere, LWH are also described as increasing the risk of cardiac arrhythmias.16 Stress-related mechanisms, caused by acute and chronic stress, may participate in a proinflammatory and hypercoagulability setting that leads to cardiovascular disease.17 18 The effect of LWH on the risk of haemorrhagic stroke remains after adjusting for cardiovascular risk factors, suggesting a direct pathway, or factors that possibly precipitate the occurrence of stroke. The effects of LWH on health are complex and several authors have highlighted the need of studies to better understand their effect on several unhealthy behaviours and diseases.19 20 LWH is associated with stroke with sufficient level of evidence.2 However, the underlying causal pathway remains unclear as well as the role of associated risks factors that can have a confounding effect or a mediating effect. This study highlights the need for exhaustive causal analyses, which differentiates ischaemic and haemorrhagic strokes.
The definition of LWH is unusual compared with the weekly working time hours used in many studies but some advantages. First, it allows consideration of atypical working hours (long shifts) that may not fit into the usual ≥55 hours a week, as well as ‘rush period’ with increase workloads for some jobs that usually have normal working hours. Second, it was possible to estimate life-time cumulative exposure to LWH. However, its main limit is that it assesses LWH as a binary variable and it differs from the usual definition of LWH in weekly hours, making direct comparison with other studies more complex, though generally, associations are similar with other studies.2 6
The main limitation of this study is the lack of power, especially in the case of ischaemic stroke, which may be caused by the relatively small number of events. Stroke remains a rare event, especially when excluding participants with a history of stroke. However, even after full model adjustments, we found a significant association in the haemorrhagic subgroup, which had fewer events than ischaemic stroke subgroup. This study together with others new studies could help clarify the effect of LWH on the risk of stroke in a future meta-analysis, which underlines the importance of individuals studies to share their results, even in the case of lack of power, we found a significant association in the haemorrhagic subgroup, which had fewer events than the ischaemic stroke subgroup. In addition, self-reported exposure could be a source of recall bias, modestly influencing results, even though the baseline questionnaire was completed and retrieved independently of the outcome. Moreover, there is a possibility of potential residual confounding, in particular related to working conditions. Lastly, some potential confounder for haemorrhagic stroke could not be considered. For example, estrogen–progestin or blood pressure drugs were not available, as well as blood pressure control which may explain why high blood pressure was not significant in the multivariable analysis, in addition to the lack of power of the study. The large population-based cohort and the extensive adjustment for cardiovascular confounding variables are the main strengths of this study. The design of the study also allowed for identifying incident cases of stroke and stroke subtypes based on medical records from a national health database.
These analyses highlight the possible differences in the association between prolonged exposure to LWH and subtypes of strokes, all limitations considered. Further studies are needed to better understand the causal pathways and possible mediators and effect measure modifiers. Reducing the global burden of stroke related to LWH, nevertheless, need better controls and interventions on both occupational exposures and lifestyle factors.
Data availability statement
Data may be obtained from a third party and are not publicly available. The data of the CONSTANCES cohort are protected by our national regulatory agency (‘Commission nationale de l’informatique et des libertés’, n°910486). However, the CONSTANCES cohort is ‘an open epidemiological laboratory’ and access to study protocols and data is available on reasonable request.
Ethics statements
Patient consent for publication
Ethics approval
This study involves human participants and was approved by All study participants provided written informed consent prior to enrollment. The study had institutional review board approval for research on human subjects (Commission nationale de l’informatique et des libertés, n° 910486, ‘Comité consultatif sur le traitement de l’information en matière de recherche’, n°10.628). The study was approved by the Angers University Hospital ethic committee (approval #2021-186). Participants gave informed consent to participate in the study before taking part.
Footnotes
Contributors MF is the guarantor of the study. MF and AD conceived and designed the study. MF and AD performed data analysis and drafted the manuscript. MF, GS, JL, AL, FP, AS, YR and AD analysed the results and critically reviewed the manuscript. All authors read and approved the final manuscript.
Funding No funding for the study (Authors are paid by their institutions). The CONSTANCES Cohort Study was supported and funded by the Caisse nationale d’assurance maladie (CNAM); it is an ‘Infrastructure Nationale en Biologie et Santé’ and benefits from ANR (ANR-11-INBS-0002) grant funding. CONSTANCES is also partly funded by Merck Sharp & Dohme (MSD), AstraZeneca, Lundbeck and L’Oréal through Inserm-Transfert. None of these funding sources had any role in the design of the study, collection and analysis of data or decision to publish.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.