Article Text

Abstract
Objectives To determine the impact of major legislative changes to New Zealand’s Occupational Health and Safety (OHS) legislation with the adoption of the Robens model as a means to control occupational risks on the burden and risk of work-related fatal injury (WRFI).
Methods Population-based comparison of WRFI to workers aged 15–84 years occurring during three periods: before (pre:1985–1992), after legislative reform (post-1:1993–2002) and after subsequent amendment (post-2:2003–2014). Annual age-industry standardised rates were calculated with 95% CI. Multivariable Poisson regression was used to estimate age-adjusted annual percentage changes (APC) for each period, overall and stratified by high-risk industry and occupational groups.
Results Over the 30-year period, 2053 worker deaths met the eligibility criteria. Age-adjusted APC in rates of worker WRFI changed little between periods: pre (−2.8%, 95% CI 0.0% to −5.5%); post-1 (−2.9%, 95% CI −1.3% to −4.5%) and post-2 (−2.9%, 95% CI −1.3% to −4.4%). There was no evidence of differences in slope. Variable trends in worker WRFI were observed for historically high-risk industry and occupational groups.
Conclusions The rate of worker WRFI decreased steadily over the 30-year period under examination and there was no evidence that this pattern of declining WRFI was substantially altered with the introduction of Robens-styled OHS legislative reforms. Beyond headline figures, historically high-risk groups had highly variable progress in reducing worker WRFI following legislative reform. This study demonstrates the value in including prereform data and high-risk subgroup analysis when assessing the performance of OHS legislative reforms to control occupational risks.
- injury
- wounds and Injuries
- accidents
- mortality
- epidemiology
Data availability statement
Data may be obtained from a third party and are not publicly available. The primary data used for this study were obtained from Archives New Zealand, Ministry of Justics and the National Coronial Information System administered by a third parties. These data are not publicly available.
Statistics from Altmetric.com
Key messages
What is already known about this subject?
Among Commonwealth industrialised nations Occupational Health and Safety (OHS) legislation based on the Robens model of performance-based self-management of occupational risks remains the preferred approach to legislating for OHS improvements in the working population.
Robens-styled OHS legislative reforms are generally considered to be a relative success internationally, however long-term evaluations of OHS outcomes to support this are rare.
What are the new findings?
Adoption of Robens-styled OHS legislation in New Zealand (NZ) maintained pre-existing trends of declining rates of worker injury fatalities, however, there was no evidence of interruption in rates of decline above and beyond previous prescriptive legalisation.
Beyond the overall 30-year trend of declining worker fatalities, selected subgroups with historically high risk of fatal injury saw mixed trends—decline, stagnation and increases in worker work-related fatal injury (WRFI) following OHS legislative reform.
How might this impact on policy or clinical practice in the foreseeable future?
This study found no evidence of change in the previous pattern of declining WRFI with adoption of Robens-styled OHS legislation to control occupational risks on 30-year trends in worker deaths.
Our findings suggest that changes in risk following Robens-styled OHS legislative reform in NZ were not evenly distributed across high-risk occupations/industries.
This study demonstrates that a more complete picture of OHS performance is obtained when data collected prior to reform is included in the analysis along with examination of subgroups with historical high risk.
Introduction
Many of the advanced industrialised nations in the Commonwealth, including the UK, Canada, Australian and New Zealand (NZ), have adopted an approach to Occupational Health and Safety (OHS) legislation influenced by the principles developed in the 1972 report by Lord Alfred Robens, commonly referred to as the ‘Robens model’.1 2 The Robens model for health and safety legislation focuses on the imposition of health and safety duties on employers and other stakeholders through the competent self-management of occupational risks using processes of regular identification, risk analysis and elimination, isolation, mitigation or control of workplace hazards.2
Performance-based Robens model OHS legislative reforms as a means of controlling occupational risks are generally considered to contribute to substantive reductions in worker fatalities such as in the UK.3 There has been little empirical evaluation of the impact of this approach on worker fatalities outside of the UK. Evaluations are limited by difficulties in robustly measuring any direct relationship between regulatory change and subsequent changes in workplace health and safety outcomes.4 5 Other explanatory pathways, such as population level shifts in the industrial and occupational composition of national economies,6 may have a substantial influence on observed changes, alongside legislative approaches. A recent meta-analysis showed moderately strong evidence of reductions in fatal and non-fatal injuries from the introduction of OHS legislation, however none of the included studies examined Robens-styled OHS legislation.7
NZ, a country with a resident working population of approximately two million people aged 15–84 years,8 has a unique history from which significant learning may be gained on the implementation of a deregulated OHS system. NZ has national OHS legislation influenced by the Robens Model and a single regulator; OHS legislation covers all workers. The enactment of the Health and Safety in Employment (HSE) 1992 Act (table 1) signalled a major change in the approach to preventing occupational injury. It replaced many ad hoc, sector-specific, prescriptive items of legislation with a single Act based on performance-based duties of care with voluntary industry standards across most places of work. A subsequent HSE Amendment Act in 2002 (table 1) further widened inclusion of worker groups and introduced worker participation rights.9 Over this historical period there have been major shifts in the structure of the NZ economy from a predominantly primary produce and manufacturing economy towards a growing consumer focused service economy. For example, the largest employer in 1985 was Manufacturing, replaced in 1995 by Community and Personal Services, then by Retail Trade and Accommodation in 2010.10
Historical context of Occupational Health and Safety Legislation in New Zealand: before prescriptive legislation (preperiod) and after (self-managing legislation in two phases; postperiod 1 and postperiod 2)
An implicit objective of both these Acts was a reduction in the rate of fatal injury involving workers. The aim of this study was to test whether this occurred by comparing work-related fatal injury (WRFI) rates prior to the legislative reform (preperiod: 1985–1992) with two subsequent periods following legislative reform: the HSE Act 1992 (post-1: 1993–2002) and the HSE Amendment Act 2002 (post-2: 2003–2014). A secondary objective was to examine whether the legislative changes affected occupational and industry groups differently. Consistent with the objective of these legislative reforms, this study will test the hypothesis that adoption of Robens-styled OHS legislation changed the pre-existing rate of decline in the rate of WRFIs in NZ11 12 over the period 1985–2014.
Methods
Study design
This retrospective population-based observational study of NZ workers used aggregated data from three iterations of the WRFI Study (WRFIS spanning the periods 1975–1984, 1985–1994 and 1995-2014.11–14
Each iteration of the WRFIS used broadly similar methodology and compatible definitions to comprehensively review Coronial case files to identify cases meeting the criteria for work-relatedness.11 12 14 15 Due to the unavailability of industry and occupation denominators for the period 1975–1984, the main analysis in this study uses the most recent 30 years of this dataset (1985–2014).
Work-related fatal injury
All workers aged 15–84 years who died in NZ from an injury that occurred while working during 1985–2014 were included. Those engaged in a work activity for pay, profit or for payment in-kind were defined as workers. Deaths to official volunteers and delayed deaths, where a direct work exposure led to the injury incident (such as work-related fatigue of an off-duty worker), and deaths occurring more than 1 year after the injury incident, were excluded. Work-traffic fatalities (those fatally injured in the course of their work while operating motor vehicles on public roads) were also excluded from this analysis as data for these incidents was not available for some of the 30-year period. Finally, ‘catastrophic’ incidents that resulted in ten or more worker deaths were excluded as these incidents are rare and have the potential to swamp the underlying trends in worker fatalities which are predominantly single fatality incidents.
Data sources
Data for this study came from two sources: the Ministry of Health’s Mortality Collection, a national register of deaths and their cause, and Coronial case files of Coronial investigations into sudden and unexpected deaths that occur within NZ. Deaths as a result of injury were selected from the Mortality Collection as those with an International Classification of Diseases 10th revision Australian Modification (ICD-10-AM) underlying cause of death external cause code (E-code) within the range V01-X59, X85-Y34, Y85-86, Y87.1, Y87.2 and Y89.9, with corresponding E-codes mapping to ICD-9-AM used for deaths prior to 2000.16 This range excludes injury deaths due to legal intervention, medical misadventure/complications, suicide or war. The subset of injury-related deaths was matched to Coronial case files, which were either archived by the Department of Justice (1985–2007) or collated by the National Coronial Information System (July 2007–2014).
Small differences in the data sources used to compile the cohort occurred between time periods. The period 1985–94 used additional administrative data sets (most of which no longer exist), identifying 10 additional cases via this means,12 while the period 1995–2014 took advantage of obtaining complete access to Coronial records regardless of underlying cause of death to additionally review cases beyond the initial ICD selection criteria.13 WorkSafe NZ-notified worker fatalities were obtained for 2014 (only year of overlapping data); no cases were identified that were not already included from Coronial records review.
Covariates
Sex and age (in years) at the time of death were obtained from the Mortality Collection. Industry, occupation and mechanism of the injury incident were encoded from text within each Coronial record. Major divisions of industry classifications in use at the time of data collection (1987 NZ Standard Industrial Classification and the 1996 and 2006 Australian and NZ Standard Industry Classification (ANZSIC)) were merged where necessary to obtain industry groupings that were compatible over time.17–19 From the first iteration of the WRFIS (1975–1984) the five industry groups with the highest rates of WRFI were identified as being ‘historically high risk’.11 Similarly, historically high-risk occupations were defined as the specific occupational groups (coded to the 1968 NZ Standard Classification of Occupation (NZSCO68))20 that had been estimated to have high rates of WRFI by the 1975–1984 WRFIS.11 These specific occupations were manually mapped across the NZSCO99 and the 2005 Australian and NZ Standard Classification of Occupation (ANZSCO V.1.0) and a binary variable was created to flag that the deceased was employed in an historically high-risk occupation.21 22 The Type of Occurrence Classification System was used to code mechanism of injury.23
Periods of legislative reform
Based on dates of enactment of the 1992 HSE Act and the 2002 HSE Amendment Act, three time periods reflecting different stages of OHS legislative reform were identified: pre (1985–1992), post-1 (1993–2002) and post-2 (2003–2014). Table 1 presents a summary of OHS legislation over this time.
Data analysis
To test the hypothesis that adoption of legislation based on the Robens model will have changed the rate of decline in the rate of WRFIs in NZ, the following assumptions were made. The first was that the general downward trend during the pre-period (1985–1992)12 occurred due to improved safety over time and, second, that this general trend would have continued regardless of the introduction of a new legislative approach. In addition, we assumed that the introduction of the HSE Act (1992) would, if effective, have increased the rate of decline, with the same assumption made for the subsequent introduction of the HSE Amended Act (2002). The pattern of decline was assumed to result in a change in slope rather than a downward ‘step’ in the level of risk of death because of the introduction of the Act and/or Amendment.
The analysis was conducted using Stata/SE V.16.24 Descriptive analysis included calculation of average annual frequency of fatal injury to workers and crude rates per 100 000 workers for each of the three periods defined by the legislation. Denominators, obtained from Statistics NZ, were employed (full and part time) usually resident population counts for those 15–84 years of age from six consecutive Censuses (1986, 1991, 1996, 2001, 2006, 2013). Intercensal annual denominator estimates were obtained using linear interpolation from available counts grouped by sex, age and either occupation or industry. Annual age standardised rates (ASR) and age-industry standardised rates (AISR) with 95% CIs were calculated using direct standardisation methods. For both the ASR and AISR, the denominators in the 30-year dataset were used as the standard population. A multivariable Poisson regression model was used to estimate the overall age-adjusted annual percentage changes (APC) for each period from the WRFI counts and worker denominator data (aggregated by year and age group). This model included two terms that allowed for a change in slope at two points in time corresponding to the timing of legislative reform. For more details of this model and the change in slope estimates, see online supplemental appendix 1. Using Stata’s ‘nlcom’ command, pre, post-1 and post-2 APCs were obtained from mathematical expressions that combined required coefficients from the model and exponentiated the results (online supplemental appendix 1). Versions of this model were used to estimate the impact of the legislation for historically high risk and specific high-risk occupational and industry groupings. Crude rates per 100 000 worker-years were calculated by mechanism of injury for each of the three periods.
Supplemental material
Results
From the 30 years of Coronial cases reviewed, 2153 deaths resulting from injury occurred in workers aged 15–84 years. Two ‘catastrophic’ incidents occurred during 1985 to 2014; worker deaths from these incidents, the 2010 Pike River Mine Explosion (n=29) and the 2011 Christchurch Earthquake (n=71), were excluded. The resulting dataset contained 2053 deaths.
Trends in numbers and crude mortality
The average annual frequency of injury deaths in workers reduced from 76.5 in the preperiod to 69.2 in the period following the 1992 HSE Act to 62.4 in the period following the 2002 HSE Amendment (table 2). The crude injury mortality rates also showed a reduction over the three periods (5.3, 4.2 and 3.2 per 100 000 worker years, respectively).
Average annual frequencies and crude rates of workplace injury deaths in New Zealand workers during three time periods with different legislation, 1985–2014
While overall trends were for declining numbers and crude rates of WRFI over the three periods defined by the HSE legislation, the trends were not all uniform and there were some notable exceptions to this trend. Rates of WRFI in female workers increased from 0.3 to 0.5 per 100 000 worker years over the three periods, although the rates and numbers of deaths were notably smaller than for males, who constitute 96% of the total WRFI for this 30-year period. A substantial increase in the crude rate between the pre-1 and post-1 period was observed for workers in the Transport, Storage and Communication and the Electricity, Gas and Water sectors. A similar pattern was observed for the occupational grouping of Hunters and Trappers, however the small number of fatalities meant the rates were imprecise. While the general pattern was for varying degrees of decline over the three legislative periods, some occupation sub-groups, such as Mining Plant Operators Pilots/Flight crew and Fishery workers, experienced comparable crude mortality rates for the pre and post-1 periods followed by substantively lower rates in post-2. The largest occupational group considered, Farmers/Farm Workers/Farm machinery operators, experienced increasing rates over time from 11.6 per 100 000 worker-years pre-HSE legislative reform to 20.3 per 100 000 worker-years in post-2. Deaths of workers in the largest industry (Agriculture, Fishing and Forestry) contributed to 44% of all WRFI for this 30-year period, with crude injury mortality rates relatively consistent over the three time periods at around 20–22 per 100 000 worker-years.
Trends in adjusted mortality rates
Annual rates of injury deaths in workers, although variable from year-to-year, indicate a declining trend over the period under examination (figure 1). Age and industry-standardised rates for 1985–2014 did not differ dramatically from the pattern observed in the crude rates (figure 1).

Crude, age industry-standardised (AIS) and predicted age industry-adjusted (AIadj) rates (95% CI) of workplace injury deaths in workers by year, in New Zealand during 1985–2014, with the addition of crude rates for 1975–1984. HSE, Health and Safety in Employment.
The overall estimated age-adjusted APC (adjAPC) in the incidence rates of injury deaths in workers during the period prior to legislative reform was very similar to that estimated for both post periods (table 3). During the preperiod an annual reduction of 2.8% (95% CI 0.0% to 5.5%) was estimated compared with reductions of 2.9% (95% CI 1.3% to 4.5%) and 2.9% (95% CI 1.3% to 4.4%) per year, respectively, for post-1 and post-2. No evidence of differences in changes in slope at either post-1:pre or post-2:post-1 was observed.
Age-adjusted annual percentage change (APC) and estimated changes in slopes in yearly incidence rates of workplace injury deaths in New Zealand workers during three time periods with different legislation, 1985–2014
Trends in rates of worker WRFI varied by high-risk industry groups and occupational groups (figure 2, table 2). In the models used to estimate this, there was minimal evidence of unexplained variation over and above that expected for the Poisson distribution. For those employed in the transport, storage and communication industry, an annual increase of 2.4% (95% CI −6.4% to 11.2%) was estimated for the period prior to legislative reform, a larger annual increase of 4.8% (95% CI 0.1% to 9.6%) for post-1 and then a post-2 reduction of 8.1% (95% CI 4.1% to 12.1%). Despite the wide CIs for the adjAPC estimates, the change in slope for the post-2 period compared with post-1 was statistically significant (p=0.001) for this industry group. Estimates obtained from combining five specific industries that were historically high-risk indicated small annual reductions that increased in magnitude over time (adjAPC pre: −0.2%, post-1: −1.5%, post-2: −2.7%); the corresponding change in slope estimates were consistent with chance alone. Estimates obtained from combining thirteen specific historically high-risk occupations followed a different pattern over time with annual reduction followed by a small increase at post-1 then reduction at post-2 (adjAPC pre: −3.1%, post-1: 1.4%, post-2: −1.6%) but again the change in slope estimates could be due to chance alone. Forestry workers were estimated to have a 7.0% annual increase in work-related injury fatalities prelegislative reform, an 8.5% annual reduction during post-1, followed by an 8.7% annual increase during post-2, with both changes in slope (post-1:pre and post-2:post-1) statistically significant (p=0.03 and p=0.002 respectively). Workers in farming occupations also had considerable fluctuation between the periods (adjAPC pre: −1.6%, post-1: 5.9%, post-2: −1.1%); the post-2:post-1 change in slope was statistically significant (p=0.03).

Crude and predicted annual rates of workplace injury deaths in workers in New Zealand during 1985–2014 for historically and specific high-risk industries and occupations.
Trends in mechanism of WRFI
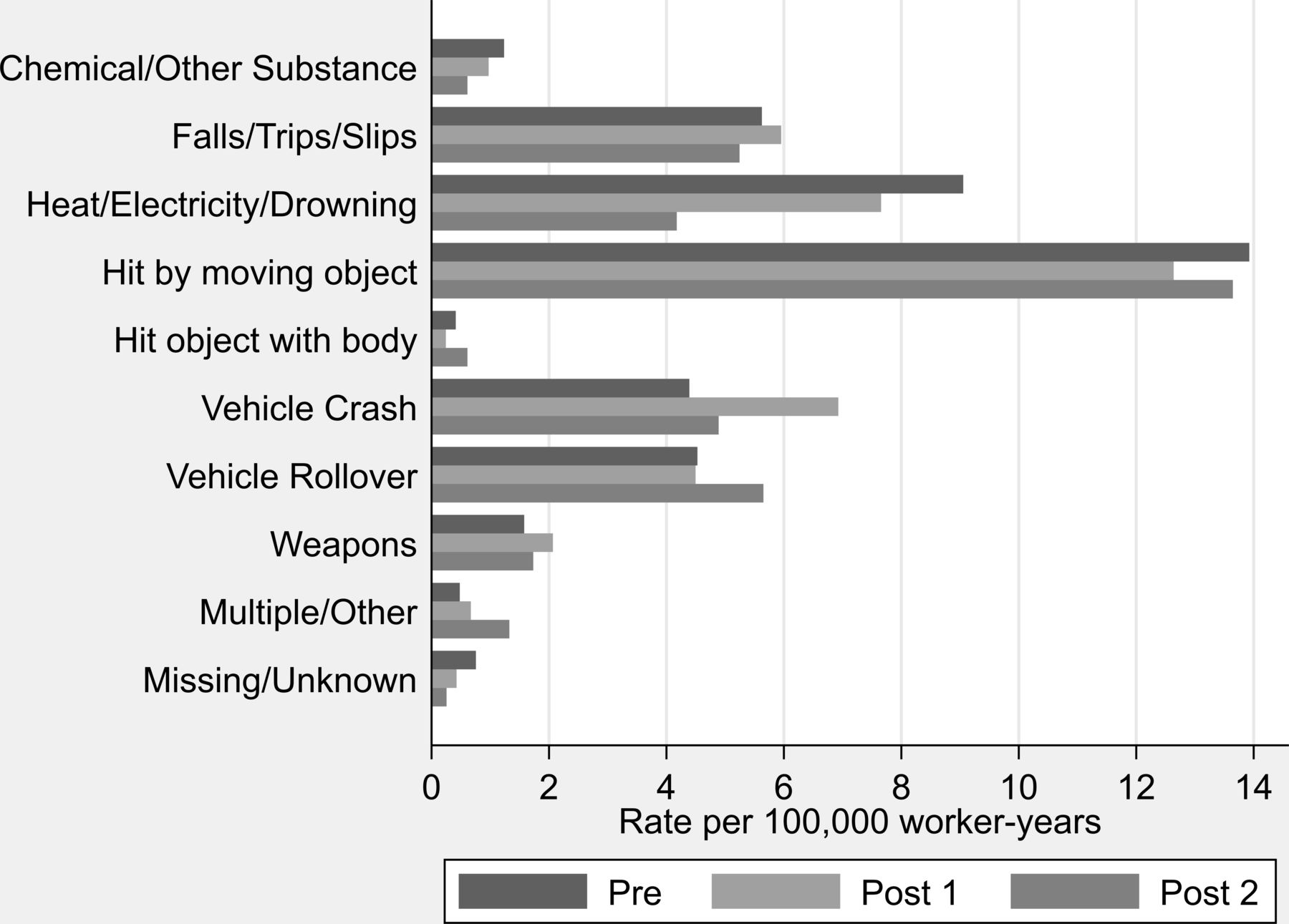
Rates of injury fatalities by mechanism were comparatively similar across each of the three periods (figure 3, online supplemental table 1). The only exception to this was consistent reductions in the rates observed for ‘heat, electricity and drowning’ deaths between the three periods (pre: 9.1, post-1: 7.7, post-2: 4.2 per 100 000 worker-years). The most common mechanism, ‘hit by a moving object’, accounted for a third of all worker injury fatalities that occurred over the 30 years; this equated to rates per 100 000 worker-years of 13.9, 12.6 and 13.7 for pre, post-1 and post-2, respectively.
Supplemental material

{kind=link}
{kind=link}
{kind=link}
Rates of fatal injury to workers in the workplace in New Zealand by mechanism and period (Pre:1985–1992, post 1:1993–2002, post 2:2003–2014; N=2053).
Discussion
Adoption of Robens-styled OHS legalisation in NZ in 1992 and in amendments in 2002 resulted in a continuation of the pre-existing pattern of decline in the rates of WRFI in workers with few changes in the underlying mechanism of fatal injury observed. Beyond headline figures, historic high-risk industry and occupational groupings demonstrated different changes in rates of decline in worker fatalities with the estimated change for two subgroups being unlikely to be due to chance alone. Taken together these findings are not consistent with the hypothesis that the adoption of a Robens-styled OHS legislative approach would result in additional benefit to pre-existing declining trends in worker WRFI.
There has been very little previous evaluation of the role of regulatory design on the impacts of OHS legislation.5 A UK evaluation of worker fatalities that focused on the cumulative headline trends over a 40-year period following the implementation of the Robens approach into OHS legislative frameworks reported an 85% reduction from 651 worker deaths in 1974 to 171 worker deaths in 2010/11 (0.6 fatalities per 100 000 workers).6 Up to half of the substantive decline in UK worker fatalities, however, was attributable to changing industry structure, such as significant declines in employment in mining and manufacturing.6 While the current study supports the overall trend in reduction of worker deaths (ie, 26% reduction between 86 worker deaths in 1985 and 64 worker deaths in 2014) this analysis is extended by including a preperiod demonstrating that legislative reform did not substantially alter the pre-existing trajectory of declining rates of worker WRFI in NZ, even after adjusting for structural changes in the workforce.
While we are not aware of other studies that have conducted similar pre–post analysis of the influence of Robens-styled OHS legislative reforms on worker WRFI it is important to consider other possible explanations for why there is a lack of evidence to support the study’s hypothesis. The available WRFI data might not be sufficiently powered to identify small changes in OHS outcomes. The lack of observed step change in WRFI trends during the transition period between old and new legislation confirmed our a priori assumption that the legislative changes (putting the onus on businesses to self-manage OHS risk) is likely to have been spread over time with some business being early adopters whereas others delayed their adoption. This is likely to blunt the rate changes between the periods examined as the impacts of the legislative changes on worker deaths will not be immediate, nor evenly distributed.
The changes towards a deregulated legislative environment with light enforcement might be less effective at managing OHS risks. NZ’s partial implementation of the principles of the Robens approach across two legislative periods also makes it difficult to generalise back to the UK experience and may, in part, also explain our findings. Another possible reason is that it is generally accepted that NZ had ‘light implementation’ of the Robens model, roundly criticised for having unclear accountabilities, poorly resourced enforcement and regulation, and late inclusion of worker representation.9 25
Our internationally novel dataset on WRFIs spanning a 30-year period, with consistent data availability, provided a unique opportunity to examine the impact of the adoption of the Robens model to OHS legislation of WRFIs. Few studies have empirically evaluated the impact of OHS legislative reforms using a robust quasi-experimental study design with nationally consistent and reliable population level data with a long time series with substantial preimplementation and postimplementation follow-up. Where possible data were adjusted for population level demographic age and industry changes, and used comparable definitions and methods to allow for meaningful comparisons over the period.
Although our analyses were limited to WRFI in workers and exclude those fatally injured in road-traffic incidents, it is important to remember that fatal workplace injuries are an important outcome indicator of OHS legislative performance. Our study does not contain a control group (control groups rarely exists in these types of population interventions), but we have used an interrupted times-series approach, a recognised method for evaluation of whole population interventions. Adjustment was limited and unable to examine other relative contributions. Age-standardised analysis was based on a slightly smaller sample with 17 cases missing age: 1–3 per year with a total of 12 in the preperiod and 5 in post-1, but this is unlikely to have importantly altered the study findings. A lack of consistent historical data on other time-varying confounders, such as full time equivalent employment for an estimate of time-at-work, and imperfect concordance mapping across occupational and industry classifications, constrained this analysis. For example, use of employed usual resident denominator includes full and part-time workers equally and could be inflating denominators, particularly for the older and female workforce. Although ‘catastrophic’ incidents involving ten, or more, worker deaths were excluded, the inclusion of smaller clusters of fatalities resulting from one event which may result in less than 10 fatalities, such as a fishing boat capsize, may inflate industry and occupation-level estimates for a period. The choice of analytical approach to examine trends using Poisson regression was informed by a desire to understand how fast OHS legislative reforms were achieving reductions in rates of worker WRFI. Other analytical analyses have focused on cumulative impact comparing incidence rates to track progress of OHS legislation. Aggregation of data by high-risk industry and occupation was necessary to overcome the analytical constraints of dispersed data with relatively few deaths in a number of categories, however, this limits the generalisability of these analyses as other countries will have different combinations of high-risk industries and occupations to NZ. In addition, limits to the extent of disaggregation in requests for Census population-level denominator data restricted our examination of other factors of interest such as region and deprivation.
Previous research has demonstrated that using underlying cause of death, as defined by the WHO using the ICD classification, substantially undercounts injury deaths theoretically defined as an injury on the causal pathway to death.26 An undercount in injury deaths could impact the study findings, but is likely to be small as none of the iterations of WRFIS data collection used for this analysis solely relied on ICD underlying cause of death to identify injury deaths.
Subsequent to the HSE Amendment Act 2002 new OHS legislation, the Health and Safety at Work Act 2015 (HSWA 2015),27 based on the Australian Model Act and Regulations also derived from Robens principles,28 has been enacted in response to the catastrophic Pike River Mine Explosion that killed 29 miners in NZ in 2010. While our dataset is unable to examine the impact of this new Act and its provisions, the findings of this analysis serve as baseline data for any future evaluation of the impact of the HSWA 2015 on worker fatalities in NZ. Future research could also consider the feasibility of an evaluation of the Robens model in NZ using serious non-fatal work-related injury as the outcome.
Conclusion
While the rate of worker WRFI decreased steadily over the 30-year period under examination, there was no evidence that this pattern was affected by the introduction of Robens-styled OHS legislative reforms to control occupational risks in NZ. Beyond the overall trend, historically high-risk industries and occupations had highly variable progress in reducing worker injury fatalities over and above the previous prescriptive legislative approach. This study demonstrates the importance of including a preperiod and examining changes in trends between periods to examine the impact of OHS legislative reform. Equally, it is important to look beyond headline figures to identify where OHS legislative reforms may be resulting in the least or most benefit.
Data availability statement
Data may be obtained from a third party and are not publicly available. The primary data used for this study were obtained from Archives New Zealand, Ministry of Justics and the National Coronial Information System administered by a third parties. These data are not publicly available.
Ethics statements
Patient consent for publication
Ethics approval
This study involves human participants and was approved by University of Otago Human Ethics Committee (Ref15/065) and Health and Disability Ethics Committee (Ref OTA/99/02/008/AM05).
Acknowledgments
The authors are grateful to staff from Archives New Zealand, Coronial Services—Tribunals Division at Ministry of Justice, New Zealand and the National Coronial Information System—Victorian Department of Justice and Regulation, Australia for the provision of coronial files. We would like to acknowledge our research assistants for their careful review and coding of coronial files. We would also like to acknowledge the memorandum of understanding between the Council of NZ University Librarians (CONZUL) and Statistics NZ through which we were able to access ‘prepaid’ customised tables of Census data.
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Contributors All authors were involved in conceiving the study. CC, SH, BMcN and RL collected, reviewed and coded the data at various iterations of the WRFIS. GD conducted the analyses with input from CC, RL, SH and TD. RL and GD drafted the manuscript. All authors reviewed the data analysis, read and approved the final manuscript. RL is the guarantor of the manuscript.
Funding This project was funded by the Health Research Council of New Zealand, grant number 16/173.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.