Article Text

Abstract
Background Occupational hand eczema (OHE) is common in hairdressers, and many leave the trade because of the disease. However, the exact impact of OHE on career length is unknown.
Objective To assess the effect of OHE on career length and risk factors associated with leaving the trade because of OHE in hairdressers followed-up for up to 35 years.
Methods A prospective cohort study of Danish hairdressers graduating between 1985 and 2007 (n=5219) was performed. A questionnaire was sent in 2009 and 2020. The Danish Labor Marked Supplementary Pension Scheme provided information on affiliation to the hairdressing profession. Career length was assessed by Kaplan-Meier analyses.
Results The median survival time was 12.0 (95% CI 11.0 to 13.0) years in graduates with OHE and 14.0 (95% CI 12.6 to 15.4) years in graduates without OHE (p<0.001). Graduates with a frequency of hand eczema (HE) of ‘once’, ‘several times’ and ‘almost all the time’ had a median survival time of 20.0 (95% CI 14.6 to 25.4), 12.0 (95% CI 10.7 to 13.3) and 7.0 (95% CI 5.6 to 8.4) years, respectively. Graduates with OHE that left the trade (partly) because of HE constituted 11.7% of the study population. Factors associated with leaving the trade because of HE included a history of atopic dermatitis (adjusted OR (aOR) 2.2 (95% CI 1.2 to 4.0), a history of a positive patch test (aOR 5.1 (95% CI 2.3 to 11.0) and allergy to hair dyes (aOR 9.4 (95% CI 3.4 to 25.6).
Conclusion Career length is reduced in hairdressers with OHE, especially if frequently relapsing or caused by contact allergy, for example, to hair dyes.
- Dermatology
- Dermatitis, Contact
- Epidemiology
- Occupational Health
Data availability statement
Data are available upon reasonable request from the National Allergy Research Centre, Denmark. Data consist of de-identified questionnaire data and career length estimates based on ATP data.
Statistics from Altmetric.com
WHAT IS ALREADY KNOWN ON THIS TOPIC
Occupational hand eczema (OHE) is a common work-related disease in hairdressers. High rates of dropouts during apprenticeship have been reported and the career length of hairdressers that have left the trade has been estimated to be less than 10 years. This has been attributed partly to hand eczema, but the exact impact of OHE on career length is unknown.
WHAT THIS STUDY ADDS
OHE reduces the career length of hairdressers, particularly if frequently relapsing. When compared with hairdressers without OHE, the risk of leaving the trade is increased by 20% by having OHE and by 90% if reporting to have had OHE ‘almost all the time’. This corresponds to a reduction in the career length by 2 and 7 years, respectively.
Hairdressers with OHE ‘almost all the time’ is a vulnerable subgroup characterised by a high prevalence of atopic dermatitis (AD) and a high prevalence of contact allergies.
The decision to leave the trade (partly) because of hand eczema was often caused by contact allergies, especially if due to hair dyes.
HOW THIS STUDY MIGHT AFFECT RESEARCH, PRACTICE AND/OR POLICY
There is a need for preventing OHE in hairdressers. When implementing preventive strategies to reduce the incidence of OHE in hairdressers, contact allergies, especially to hair dyes, should be considered as an important exposure in addition to wet work. Special protection is warranted in hairdressers with a history of AD.
Introduction
Occupational hand eczema (OHE) is a common work-related skin condition in hairdressers. The incidence rate of recognised OHE in Denmark is 33.4/10 000 hairdressers per year, making hairdressing the most commonly affected profession.1 OHE often causes job change, a decrease in quality of life and has a high cost-of-illness to society. Therefore, a better understanding of its consequences is needed when planning prevention and giving career guidance to patients with OHE.2 3
The lifetime prevalence of hand eczema (HE) has been estimated to 45.2% in hairdressers.4 Factors associated with OHE in hairdressers are wet work, a history of a positive patch test reaction and a history of atopic dermatitis (AD).4 5 The excessive exposure to irritants and allergens in hairdressing leads to onset of OHE already during apprenticeship. Studies including clinical examinations have shown a prevalence of moderate-to-severe HE in up to 43.2% of hairdressing apprentices and 31.9% of fully trained hairdressers.4 6–8
Among hairdressing apprentices who did not complete apprenticeship, 30.1% of German apprentices gave ‘skin problems’ and 42.1% of Danish apprentices gave ‘HE’ as (partial) reason for dropping out.7 9 Furthermore, a study on fully trained hairdressers showed that hairdressers who had left the trade had worked an average of 8.4 years in the trade, and that 23.1% of them gave HE as part of the reason for their career change.10 Factors associated with leaving the trade because of HE included a high frequency of HE and a history of AD.
No studies have previously assessed the impact of OHE on career length in hairdressers. We aimed to estimate the effect of OHE on career length in hairdressers in a population followed-up for up to 35 years. Additionally, we re-examined the risk factors for leaving the trade because of HE with an emphasis on contact allergies.
Methods
A prospective cohort study of hairdressers graduating from Danish vocational schools between 1985 and 2007 was performed. A detailed description of methods and delineation of the study cohort has previously been published.4 In brief, all hairdressers graduating between 1985 and 2007 (n=8525) from the Danish Hairdressers Union were asked to participate in a survey. A postal questionnaire was first sent in 2009. Another follow-up questionnaire was sent in 2020 to respondents of the 2009 questionnaire (n=5219). A response rate of 61.2% (5219/8525) was obtained in 2009 and a response rate of 50.1% (2614/5219) was obtained in 2020 corresponding to 30.1% (2614/8525) of all hairdressers graduating form 1985–2007. Only data from respondents from the follow-up questionnaire in 2020 were included in the present study.
Data from registries
The Danish Labor Market Supplementary Pension scheme (ATP) provided information on payments made from the hairdressing profession for individuals in the cohort. ATP is a mandatory pension scheme in Denmark. Each contribution is tagged with the date of payment and type of profession. Employers are obliged to contribute on behalf of their employees if the employee works >10 hours/week. It is voluntary for independent hairdressers to contribute on their own behalf. ATP data includes payments from the beginning of apprenticeship which for Danish hairdressing apprentices constitutes 148 weeks (excluding 60 weeks in school).11 The time worked as a hairdresser was calculated as the sum of the number of years that a graduate had contributed to ATP. Thus, the yearly affiliation to the trade encompassed both the years worked as apprentice and as a fully trained hairdresser and did not contain potential career gaps, except maternity leave during continued employment, which was included in the numerator of individual person time.
Definition of outcome variables
HE was defined as an affirmative answer to the question ‘have you ever had hand eczema?’ (yes/no). OHE was defined as HE with onset during hairdressing apprenticeship or during work as a fully trained hairdresser. The onset of HE was assessed by the questions ‘When the hand eczema started, were you then a…’ (hairdressing apprentice/fully trained hairdresser/other) and ‘When did you have hand eczema for the first time?’ (year). It was possible for respondents to grade the frequency of their HE responding to the question ‘how often have you had eczema on your hands?’ as ‘once’, ‘several times’ or ‘almost all the time’. To have left the hairdressing trade (thus being an ex-hairdresser) was defined by the second response alternative to the question ‘what is your current occupation? ‘(I work as a hairdresser/I no longer work as a hairdresser)’. To have left the trade because of HE was defined as an affirmative answer to the question ‘I left the trade because of hand eczema’ (yes/no). See the online supplemental material for the definition of AD and patch test results.
Supplemental material
Statistics
Overall, OHEs influence on career duration was assessed by Kaplan-Meier analysis and OHEs influence on being an ex-hairdresser by Cox regression. A logistic regression was used to assess factors associated with deciding to leave the trade because of HE among hairdressers with OHE.
Comparison of categorical data were done by χ2 tests. When performing Kaplan-Meier analysis, occupational status in terms of being an ex-hairdresser was used as the outcome and yearly affiliation to the hairdressing trade was the time scale. Career duration was reported as the median survival time. Graduates still working as a hairdresser at the end of the study period (March 2020) were censored. No other censoring events were considered. The study population was stratified by OHE (yes/no) and by the frequency of HE (once/several times/almost all the time). A log-rank test was used to test for statistically significant differences in survival between these subgroups. Further, two Cox-regression models were used to estimate the size of this difference, quantified as adjusted HRs (aHR). Both contained occupational status as an ex-hairdresser (vs being a current hairdresser) as the outcome variable, and sex (male/female), age (21–30/31–40/41–50/51–60/>60 years) and a history of AD (yes/no) as covariates. Further, one model additionally included OHE (yes/no), and the other the frequency of OHE (never/once/several times/almost all the time) as the respective explanatory variable of interest.
Factors associated with HE as a specific reason to have left the trade were solely analysed in the subgroup of ex-hairdressers with OHE, and therefore did not include censored individuals. In this subgroup, a logistic regression model was chosen to assess these factors. Thus, among ex-hairdressers with OHE, a comparison was made between those stating to have left the trade because of HE and those that left for other reasons. The dichotomous outcome variable was to have left the trade because of HE (vs to have left the trade but not because of HE, despite having (had) HE). Explanatory variables were sex (male/female), age (21−30/31−40/41−50/51−60/>60 years), a history of AD (yes/no), frequency of HE (once/several times/almost all the time), patch test history (not patch tested/negative patch test/positive patch test) and allergy to hair dyes, preservatives, perfume, nickel or other were used as explanatory variables. Wet work was not included in the analysis, as only information on current wet work was available, which was confirmed by 86.8% (2465/2848) of current hairdressers in the baseline study of this cohort and only in 5.8% of ex-hairdressers.4 As a consequence of the homogeneity of wet work as an exposure, it was not identified as a risk factor for OHE. A logistic regression model was used to identify risk factors for having a frequency of HE of ‘almost all the time’ versus ‘once’. Explanatory variables were sex, age, a history of AD, a history of positive patch test and contact allergies. A p value<0.05 considered significant. Statistical calculations were performed in IBM SPSS Statistics V.25.
Results
Characteristics of the study population
The characteristics of the study population have previously been published.4 In brief, 50.1% (2614/5219) hairdressers graduating from Danish vocational schools from 1985 to 2007 responded to the follow-up questionnaire in 2020. 96.3% (2518/2614) of respondents were women, the median age at follow-up was 49.0 years (range 33–82) and 6.0% (155/2569) had a history of AD. The lifetime prevalence of OHE was 40.9% (1068/2612) (table 1). Graduates with OHE reported a frequency of HE of ‘once’, ‘several times’ and ‘almost all the time’ in 16.5% (175/1058), 59.8% (633/1058) and 23.6% (250/1058) of cases. In 2020, 57.3% (1497/2614) of respondents were ex-hairdressers (figure 1). Respondents and non-respondents in 2020 were identical in 2009 in terms of the proportion of ex-hairdressers, the prevalence of HE and the prevalence of a history of AD. ATP data were available for 91.2% (2385/2614) of the study population.
Occupational status and characteristics of Danish hairdressers graduating from 1985 to 2007
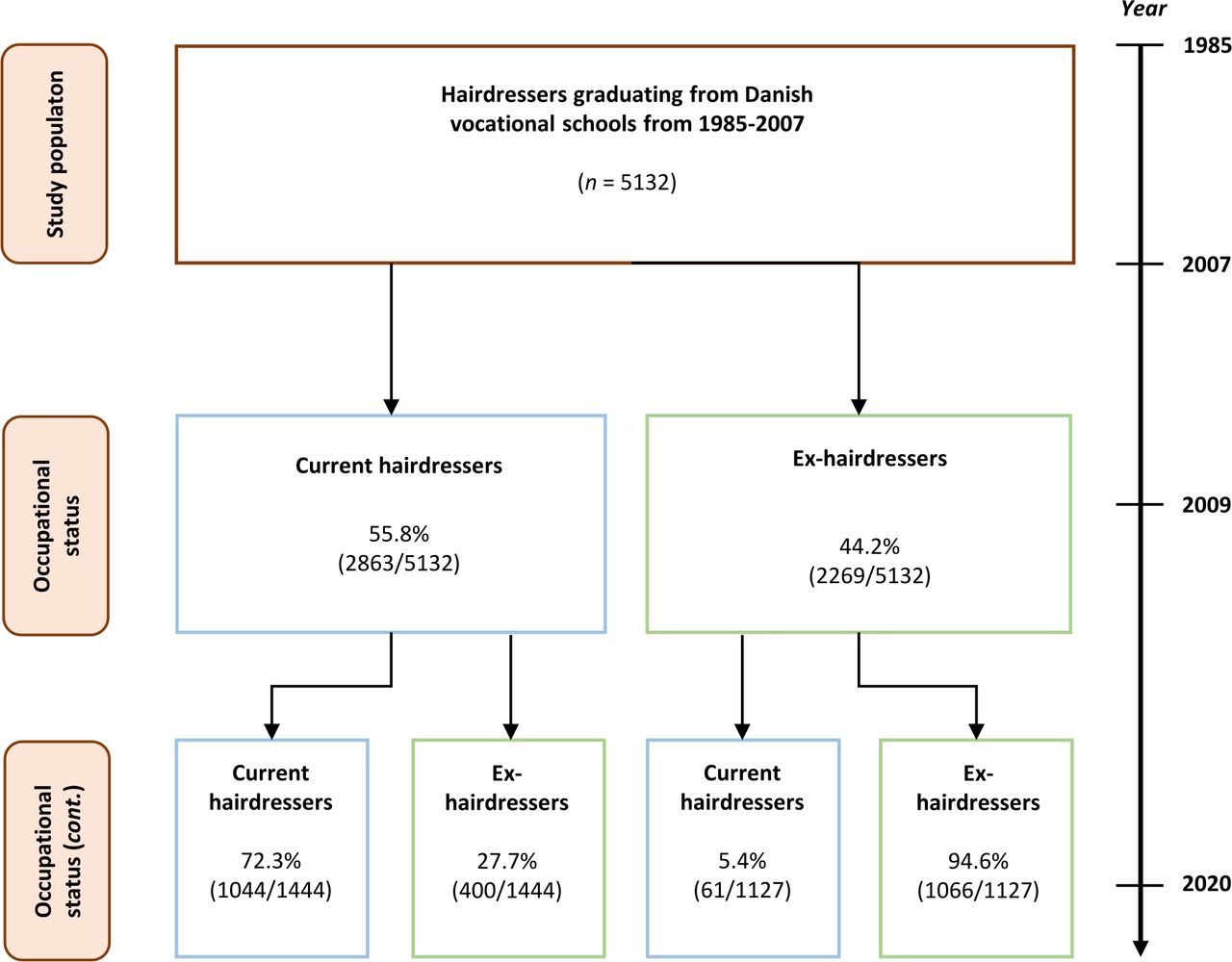
Proportion of hairdressers graduating from 1985-2007 that leaves and rejoins the trade across time.
Kaplan-Meier survival analysis: career duration
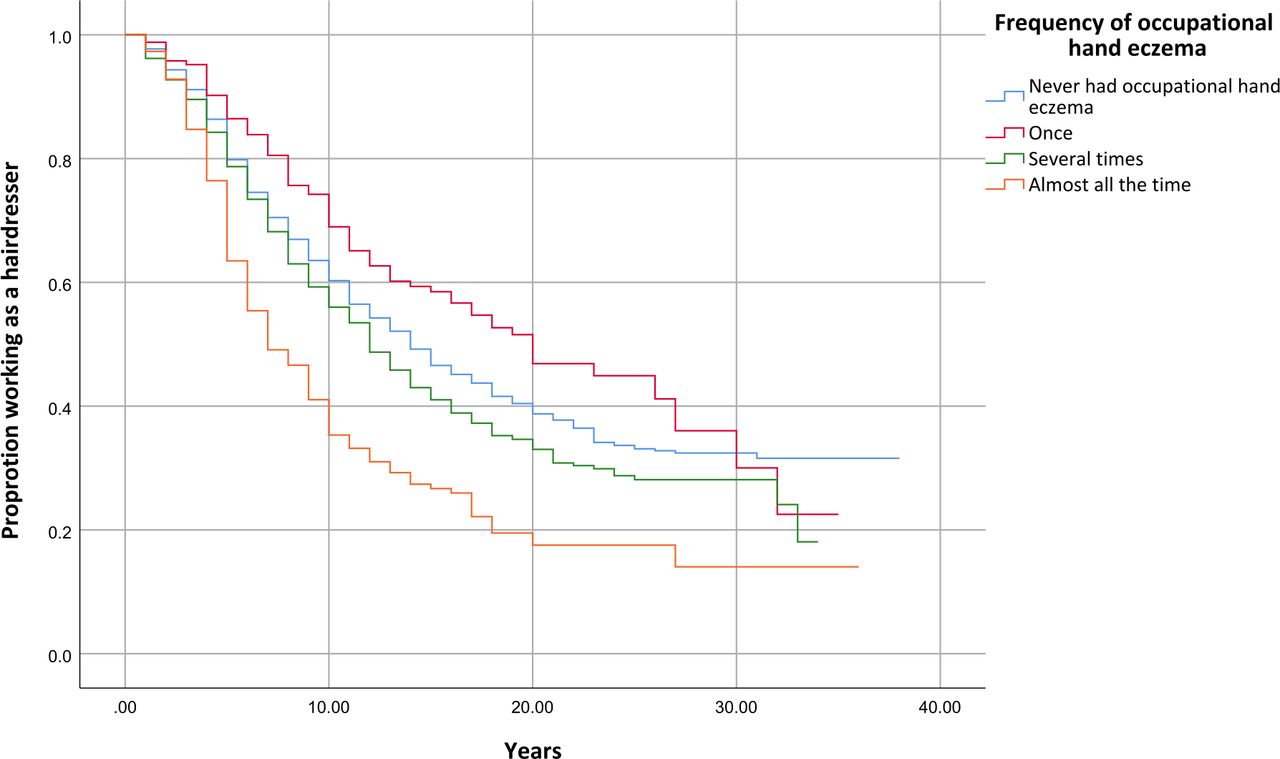
A median survival time of 13.0 (95% CI 12.2 to 13.8) years was observed for the total study population. Graduates with OHE had had a median survival time of 12.0 (95% CI 11.0 to 13.0) years and graduates without OHE had a median survival of 14.0 (95% CI 12.6 to 15.4 (p<0.001) years (online supplemental table 1, online supplemental figure 1). The median survival times decreased with an increasing frequency of OHE. Graduates with a frequency of HE of ‘once’, ‘several times’ and ‘almost all the time’ had a median survival time of 20.0 (95% CI 14.6 to 25.4), 12.0 (95% CI 10.7 to 13.3) and 7.0 (95% CI 5.6 to 8.4) years, respectively. Graduates with a frequency of HE of ‘once’ had higher median survival time than hairdressers without OHE (p=0.02) (table 2, figure 2).
Characteristics and career length of graduates with or without occupational hand eczema (OHE)

{kind=link}
{kind=link}
Kaplan-Meier survival analysis of hairdressers with occupational hand eczema reporting on their frequency of hand eczema (n=969).
The median survival time in the subgroup of all ex-hairdressers (n=1330) was 7.0 (95% CI 6.6 to 7.4) years. No difference was observed between the median survival time of ex-hairdressers with and without OHE being 7.0 (95% CI 6.5 to 7.5) in both subgroups (p=0.63) (online supplemental table 1). Thus, ex-hairdressers with and without OHE did not differ in the tendency leaving the trade. However, ex-hairdressers with OHE stating specifically to have left the trade because of HE had a lower median survival than ex-hairdressers with OHE stating not to have left because of HE being 6.0 (95% CI 5.4 to 6.6) and 8.0 (95% CI 7.2 to 8.8) (p=0.001), respectively (online supplemental table 1, online supplemental figure 2).
Cox regression: the association between OHE and being an ex-hairdresser
Graduates with OHE had a higher risk of leaving the trade, compared with graduates without OHE (aHR 1.2 (95% CI 1.0 to 1.4) (table 1). Leaving the trade was additionally associated with a history of AD (HR 1.3 (95% CI 1.0 to 1.6)). Further, an interaction between a history of AD and OHE (aHR 1.4, 95% CI 1.1 to 1.8) was identified. Graduates with a frequency of HE of ‘almost all the time’ (aHR 1.9 (95%CI 1.6 to 2.3) and ‘several times’ (aHR 1.2 (95% CI 1.1 to 1.4) had an increased risk of leaving the trade, when compared with graduates without OHE (reference) (table 1). Graduates who had only had OHE ‘once’ had a decreased risk being ex-hairdressers (aHR 0.8 (95% CI 0.6 to 1.0)). An interaction between a history of AD and a frequency of HE of ‘almost all the time’ (aHR 2.1 (95% CI 2.1 to 1.5–3.0) was found. No interaction with a frequency of HE of ‘once’ or ‘several times’ were found.
Proportion of ex-hairdressers who left the trade because of HE
The proportion of ex-hairdressers with OHE that stated HE as (part of) the reason to leave the trade was 51.7% (307/594). Conversely, 48.3% (287/594) of those with OHE that left trade did so for other reasons (online supplemental figure 3). Ex-hairdressers with OHE that left the trade because of HE constituted 11.7% (307/2614) of the study population and 22.4% (307/1370) of all ex-hairdressers.
Logistic regression: factors associated with reporting to have left the trade because of HE
Among ex-hairdressers with OHE, those stating to have left the trade because of HE were characterised by (a) a history of AD, (b) a history of a positive patch test and (c) allergy to hair dyes, when compared with ex-hairdressers with OHE that left for other reasons (table 3). Among ex-hairdressers that left the trade because of OHE 17.3% had a history of AD (adjusted OR (aOR) 2.21 (95% CI 1.23 to 3.98). A total of 60.9% (187/307) had history of a positive patch test (aOR 5.05 (95% CI 2.31 to 11.02); risk estimated with negative or lacking patch test as reference. A positive patch test specifically to hair dyes were seen in 26.1% (80/307) of ex-hairdressers that left the trade because of OHE (aOR 9.37 (95% CI 3.43 to 25.61), reference being those testing negative along with those in whom patch testing was not performed). No association was found with sex, age, debut of OHE as a hairdressing apprentice or fully trained hairdresser, a history of a negative patch test or allergy to perfume, preservatives, nickel.
Characteristics of ex-hairdressers with occupational hand eczema that left the trade (n=594), either because of hand eczema or for other reasons
Discussion
In this study we assessed the effect of OHE on career length in hairdressers followed-up for up to 35 years after graduation. Career length in hairdressers with OHE was reduced with frequency of HE being an important determinant for reduced career length. Compared with graduates without OHE, the risk of leaving the trade increased by 20% in graduates with OHE and by 90% in graduates with a frequency of OHE of ‘almost all the time’, according to Cox regression analyses. Half of graduates with a frequency of OHE of ‘almost all the time’ had left the trade by the 7th year in the profession, compared with the same attrition achieved only in the 14th year in graduates without OHE. These estimates include the time worked as a hairdressing apprentice (148 weeks or 2.8 years), indicative of OHE having a considerable impact on career length.11 In addition, graduates with OHE ‘almost all the time’ were identified as a vulnerable subgroup with a high proportion of ex-hairdressers (74.0%), a high prevalence of history of AD (20%) and a high prevalence of contact allergies (64.4%). Interestingly, having had OHE ‘once’ decreased the risk of being an ex-hairdresser (aHR 0.78; borderline significance). Thus, hairdressers with HE ‘once’ may represent a substratum of the study population whose skin tolerates the work environment, either due to a low prevalence of AD or due to knowledge of preventing of HE, that is, compliance with glove use and use of emollients. Such compliance with protective measures may be related to the wish to remain in the job. Despite these favourable conditions, they still experience a single episode of HE, most likely because of the high exposure to irritants and allergens in hairdressers’ work environment.
A general tendency to leave the trade was evident, as ex-hairdressers with and without OHE had identical career length in terms of a median of 7 years. Career termination in hairdressers seems therefore to be multifactorial with OHE being one of many reasons to leave the trade. This is in line with other notable reasons such as ‘musculoskeletal complaints’ ‘allergies’, ‘various personal reasons’ and ‘work conditions’ previously having been reported.5 10 12 Nevertheless, graduates with OHE that left the trade (partly) because of HE constituted 11.7% of our study population and had a shorter career length (median 6 years) compared with those that left for other reasons (median 8 years).
We identified the associations with reporting to have left the trade because of OHE to be: (1) a history of AD, (2) a history of a positive patch test reaction and (3) an allergy to hair dyes. In patients with recognised OHE seen by a dermatologist, risk factors for job change were previously identified as young age, a positive patch test (regardless of relevance) and severe HE.13 As these risk factors largely overlap with the associations of deciding to leave the trade because of OHE, both the tendency of OHE to reduce career length in the total study population and particularly in hairdressers stating to have left the trade because of OHE is not surprising. Interestingly, in a 7-year follow-up study of patients with HE, contact sensitisation was found to be inversely related to job change.14 The authors speculated that this was due to knowledge of how to avoid the offending allergens. We found the association with leaving the trade to be almost two times higher for hair dye allergy compared with a history of a positive patch test in general. Thus, hair dye allergy seems to lead to career change rather than preventive avoidance in hairdressers. This inability to remain in the profession is explained by the high prevalence of hair dye allergy among hairdressers and the high frequency of hair dye exposing procedures performed by hairdressers.4 15 16 No association was seen with allergy to nickel, preservatives or fragrances. As the prevalence of nickel allergy in Danish hairdressers and matched controls patch tested in Denmark is identical and Danish hairdressers’ tools generally seem to release low levels of nickel, this lack of association seems reasonable.15 17 Our cohort has graduated since three epidemics of contact allergy to preservatives, namely methylchloroisothiazolinone (MCI) in combination with methylisothiazolinone (MI) in the 1980s, methyldibromo glutaronitrile (MDBGN) in the 1990s and MI in the 2000s.18 As the latter was caused primarily by cosmetics, including rinse-off products, the lack of association with preservatives is not as obvious. Moreover, in a perhaps more selected clinical sample of hairdressers patch tested for suspected contact allergy to hair cosmetic ingredients, a roughly tripled prevalence of preservative contact allergy (to MDBGN and MCI/MI at the time) compared with consumers also tested for hair cosmetic-related contact dermatitis has been identified.19 Concerning MI alone, MI was first introduced in the European baseline series in 2014, possibly leading to a (general) underdiagnosis of MI contact allergy until that time which is why hairdressers leaving the trade before 2014 due to MI allergy may not have known the cause of their disease.20 Lastly, the lack of association with contact allergy to nickel, preservatives, and perfumes may be explained by these not being as relevant and potent allergens as hair dyes, represented by p-phenylenediamine.
The tendency of OHE to cause early career change has previously been shown by Meding et al, who conducted a follow-up study of patients with HE from Swedish general population. In their cohort, 8% had changed profession because of OHE at baseline, compared with only 3% at a 15-year follow-up.21 22 Most of the abandoned jobs were high-risk occupations for OHE like hairdressing, but the prevalence of job change because of OHE was much lower compared with our findings. Overall, hairdressers seem to change profession because of HE much more often than the general working population.
Strengths and limitations
Our study population only comprised graduated hairdressers, that is, individuals who dropped out already during apprenticeship were not taken into account. In Germany, the proportion of hairdressing apprentices who drop out has been estimated to 48.1% (1218/2532) with 39.1% (245/560) reporting skin problems as a reason.7 Thus, the overall proportion leaving the trade because of HE is potentially underestimated. The use of ATP data to estimate the yearly affiliation to the trade provided a precise and objective estimate for each participant in the cohort but does come with the shortcoming of payments to ATP only being mandatory for employed hairdressers, and not for self-employed. The career length may therefore be underestimated if graduates become salon owners, decide not to contribute on their own behalf and stay in the trade. A publication from ATP stated that 26% of salon owners did not contribute on their own behalf in the period 2005–2009, however the proportion of salon owners in our study is unknown.23 The effect of age-related retirement seems negligible as only 1.1% of our study population was above 60 years of age. The definition of OHE as HE with onset as apprentice or as fully trained hairdresser is expected to be highly sensitive, but potentially includes graduates with non-occupational HE. Furthermore, this definition of OHE potentially introduces an immortal time bias in the survival analysis of hairdressers with OHE, as participants with OHE needed to have worked a certain time in the trade to have had a chance to get OHE, in contrast to those without OHE, who could leave anytime. However, the median time to onset of OHE was merely 2.0 years, including apprenticeship, (online supplemental figure 4) which is why we deemed immortal time bias to be of limited impact.
In terms of secular trends in the Kaplan-Meier survival analysis, no significant difference in median survival time for hairdressers graduating from 1985 to 1993 and from 1994 to 2007 was observed, being 13.0 (95% CI 11.8 to 14.2) and 14.0 (95% CI 12.7 to 15.3) (p=0.08) respectively. However, hairdressers graduating from 1994 to 2007 tended more than those graduating from 1985 to 1993 to report to have had HE (OR 1.4, 95% CI 1.2 to 1.6) and have allergy to hair dyes (OR 1.5, 95% CI 1.0 to 2.1). No difference was observed in the proportion with a high frequency of HE or with a history of a positive patch test (online supplemental table 2). Although some of the factors associated with deciding to leave the trade because of HE changed across time, these differences were deemed small enough to perform an overall Kaplan-Meier survival analysis. This is a compromise that in turn provides a valuable insight into the impact of OHE in a cohort of hairdressers, spanning almost a complete career length.
Conclusion
The career length in hairdressers with OHE is decreased, with the frequency of HE being an important risk factor. Contact allergy, especially to hair dyes, is a strong indicator of leaving the hairdressing profession because of HE.
Data availability statement
Data are available upon reasonable request from the National Allergy Research Centre, Denmark. Data consist of de-identified questionnaire data and career length estimates based on ATP data.
Ethics statements
Patient consent for publication
Ethics approval
This study involves human participants and was approved by The Danish Data Protection Agency (reference number P-2019-346). Participants gave informed consent to participate in the study before taking part.
Acknowledgments
The Danish Hairdressers’ and Beauticians’ Union, The Danish Hairdresser Association and The Danish Labor Market Supplementary Scheme.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Contributors MH: writing original draft, formal analysis and conceptualisation (support), guarantor. JPT: critical review and editing. CZ: critical review and editing. WU: critical review and editing. JDJ: critical review and editing and conceptualisation.
Funding This study was funded by an unrestricted grant from the Danish Hairdressers and Beauticians Union (grant number: not applicable).
Competing interests MH has no competing interest. JPT has received consulting fees from Coloplast and honoraria from Pfizer, AbbVie, Regeneron, Sanofi-Genzyme, LEO, Lilly, Almirall and has participated on a Data Safety Monitoring Board or Advisory Board for Pfizer, AbbVie, Regeneron, Sanofi-Genzyme, LEO, Lilly, Almirall, Arena, Aslan. CZ has received consulting fees from Jansen Cilag, Novartis and Leo Pharma and is a board member of the European Academy of Dermatology and Venereology. WU has a grant agreement for providing data management and analysis in the EFISS project of the IDEA/IFRA project group, has received travel reimbursement for attending IDEA project meeting in Munich August 2019 and is an external expert for the ‘Scientific Committee on Consumer Safety’ (SCCS) of the EU. JDJ has received grants from National Environmental Protection Agency and Leo Foundation, received an honorarium for lecture at The Yearly Meeting of Spanish Dermatologist, is head of Cosmetic Council and advisor to the Danish Minister of Environment (unpaid), President Elect in European Society of Contact Dermatitis (unpaid) and editor-in-chief for the journal Contact Dermatitis.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.