Article Text

Abstract
Objective To investigate repetitive movements and the use of hand force as causes of treatment for distal upper extremities musculoskeletal disorders
Methods A cohort of 202 747 workers in a pension health scheme from 2005 to 2017 in one of 17 jobs (eg, office work, carpentry, cleaning) was formed. Representative electro-goniometric measurements of wrist angular velocity as a measure for repetition and expert-rated use of hand force were used in a job exposure matrix (JEM). Job titles were retrieved from the Danish registers. Outcome was first treatment in the distal upper extremities. In a Poisson regression model, incidence rate ratios (IRRs) of treatment were adjusted for age, calendar-year, diagnosis of rheumatoid arthritis and arm fractures. In further analyses, wrist velocity or hand force was added.
Results In men, wrist velocity had an IRR of 1.48 (95% CI 1.15 to 1.91) when the highest exposure level was compared with the lowest but with no clear exposure-response pattern. The effect became insignificant when adjusted for hand force. Hand force had an IRR of 2.65 (95% CI 2.13 to 3.29) for the highest versus the lowest exposure with an exposure-response pattern, which remained after adjustment for wrist velocity. Among women, no increased risk was found for hand force, while wrist velocity showed a significantly protective association with treatment.
Conclusions In men, occupational exposure to hand force more than doubled the risk of seeking treatment. The results for exposure to repetition were less clear. In women, we could not find any indications of an increased risk neither for force nor for repetition.
- workload
- longitudinal studies
- occupational health
- upper extremity
- ergonomics
Data availability statement
Data from the JEM are available upon reasonable request. Data from the Danish national registers are available through online access at Statistics Denmark under standard conditions.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Key messages
What is already known about this subject?
Some evidence exits of an association between measures of hand force and repetition and tendinitis of the wrist and epicondylitis of the elbow; however, these studies have often been limited by bias because of self-reported exposure and an outcome sensitive to time fluctuations.
What are the new findings?
We found a clear exposure-response association between expert-rated use of hand force in 17 different jobs and treatment for pain in the arms and hands in a private health scheme among men.
An effect of high repetition using technical measurements of wrist angular velocity was less evident and disappeared when controlling for use of hand force.
Among women we did not find any increased risk.
How might this impact on policy or clinical practice in the foreseeable future?
Preventive strategies should focus on reducing the use of hand force in the working population.
Introduction
Distal upper extremity musculoskeletal disorders (D-UEMSD) are highly prevalent among the working population with epicondylitis of the elbow and tenosynovitis of the hand or wrist as the most commonly recognised occupational diseases in the European Union.1 Musculoskeletal disorders are a leading cause of work disability and loss of productivity across Europe.2 Incidence of epicondylitis and hand or wrist tendinitis ranges from 0.45 to 7.0 per 100 workers depending on case definition and population.3 The most consistent non-occupational risk factors include age, female sex, obesity, psychosocial factors, previous injuries and inflammatory arthritis.4 5
Prospective studies have examined the work-relatedness of epicondylitis and hand or wrist tendinitis.5–12 Follow-up time ranges from 2 to 6 years and case definition varies from self-report to findings based on physical examination. Different definitions of exposure have been used to describe ranges of repetition, use of force, posture or hand-arm vibrations. Reviews have found some evidence of an exposure-response effect between force and risk of hand or wrist tendinitis and inconsistent associations with measures of repetition and posture alone.13 14 Combined exposures may be a multiplicative risk factor but a low incidence of disease in the studies combined with an uneven distribution of severe exposures in the study populations has prevented the investigation into such interactions.14 The risk of epicondylitis has been related to repetitive movements of the elbow, wrist or forearm and high force in combination with repetitive movements or awkward positions, but the evidence of force, posture and repetition as single risk factors is less clear.14 15
It is paramount to separate measures of exposure from outcome in a prospective design to draw causal conclusions. However, obtaining enough statistical power can be difficult when objectively measured exposures and outcomes are used. Often, registers will ensure the objective outcomes, but not when examining temporally fluctuating and under-reported diseases and conditions such as epicondylitis and hand or wrist tendinitis.16 17 In that case, close monitoring and follow-up is needed, and this is costly and time-consuming.
Quantitative measurements for the exposure can be obtained by direct observation, self-report or technical measurements. Register information on job title and industry and measurements of job-related exposures can be combined in a job exposure matrix (JEM).18 This separates exposure and outcome and enables formation of large cohorts that can be followed for a long period of time.19–22 Using this method in the Danish registers an exposure-response effect of increasing wrist angular velocity on carpal tunnel syndrome has been found, but associations with force and combinations of force and repetition could not be examined due to lack of available force measurements.19 Expert-rated force has been used recently in JEMs, and may allow for investigation into combinations of force and repetition.23 24
In parallel with the public treatments of diseases, private sector health programmes have emerged that offer treatments for musculoskeletal pain. Using such a health scheme as an outcome measure, where access to treatment is easily available and not dependent on a doctor’s referral, may reveal more cases and strengthen the investigation into causality.
The purpose of this study was to investigate the association between repetitive movements of the wrist and the use of hand force and seeking treatment for pain in the distal upper extremities, using a JEM in a population covered in a health scheme.
Methods
Study population
We established a cohort of persons aged 18–65 years covered by a private Danish pension fund, the PensionDanmark Health Scheme (PDHS), between October 2005 and December 2017. The Danish Civil registration system allowed for linkage to national registers at Statistics Denmark. Annual information on the main occupational titles were added by using the Occupation and Industry Register in the Danish Occupational Cohort with eXposure data based on the Danish version of the International Standard Classification of Occupation and the Danish Industrial Classification of All Economic Activities.25–27 Educational level was derived from the Danish version of the International Standard Classification of Education.28
Exposure measurements
As a measure of repetition, we used the results of goniometric measurements from studies pooled in the EMINGO database, hosted by the Department of Occupational and Environmental Medicine, Lund, Sweden. Seventeen jobs were covered by the PDHS. Of these, 14 were measured in Denmark and 3 in Sweden, with the use of identical measurement protocols and equipment. The job functions in the Swedish measurements were comparable to Danish conditions.
The measurement programme has previously been described in detail.19 21 29 Briefly, companies and employees with exposures believed to be typical for the job titles selected for the study were asked to participate (see online supplemental table 1). Measurements were performed on healthy, right-handed individuals with no musculoskeletal complaints. Jobs were selected in order to secure large contrasts in exposure. Measurements in at least 10 men or 10 women or both (if job functions differed with sex) were considered to provide accurate job exposure estimates.30 Mean measurement time was 5.7 hours (3.1–6.7).
Supplemental material
Whole working day (excluding pauses) wrist measurements were performed using biaxial goniometers (SG75, Biometrics, Newport, UK) and person-worn data-loggers (Logger Teknologi, Åkarp, Sweden) with a sampling frequency of 20 Hz. Angular velocity (°/s) was selected as measure for repetition. The goniometers were placed on the dorsal side of the wrist with the proximal part in the midline between radius and ulna and the distal part over the third metacarpal bone. Analyses were made for both sides but in this study, we only report results from the right (and dominant) side.
As a measure of force, the following Expert-JEM was used: five physicians, specialised in occupational medicine rated the level of the daily duration of significant use of hand force in 33 job titles with representative goniometric measurements whereof 17 were covered in the PDHS. This was rated in five categories and noted on rating cards for each job title: ‘no or an insignificant part of the time’, ‘a small part of the time’, ‘some of the time’, ‘much of the time’ and ‘most of the time’, scored 1–5. It was believed that ordering by quantitative category boundaries was unlikely to add any important information as it is easier to assess duration on a qualitative than on a quantitative scale. Each card included a short description of the work tasks performed during the measurements. The expert placed the cards in the relevant rating categories with a further split into two subcategories, low and high. The latter group was then scored with an addition of 0.5 points to the main category score, resulting in 10 scores (1– 5.5 by steps of 0.5 score points). The experts received a written instruction and the instruction was further discussed at a meeting to ensure a common understanding of the rating task. Approximately 1 month after the first exposure rating the experts repeated their ratings, blinded to their first rating. The partial Spearman’s correlations and overall agreement (weighted kappa) were both above 0.80 (details will be published separately). The combined mean value of the ratings was used as the exposure value.
Outcome and health-related confounders
The PDHS covers mainly employees in blue collar work, skilled and unskilled. The health scheme provides members with access to medical services including physiotherapy and chiropractors at numerous private health clinics (for further details see Pedersen and Arendt31). The PDHS is owned by a not-for-profit labour market pension fund and operated by a private healthcare provider. The PDHS has existed since 2005 with stepwise inclusion of jobs in additional collective agreements. The purpose of the PDHS was to prevent and treat work-related illness but injuries originating from leisure time activities have since been included. Membership is provided by collective agreements between companies and workers. The mandatory, tax-deductible annual premium is €48 per member and is automatically deducted in the pension contributions. The use of the service is not reported to neither employer nor labour union. Number of treatments received are typically not restricted and no physician referral is required. All individual treatments in the PDHS are registered at every visit. Type of treatment and body region of concern are registered in the invoice sent by the healthcare provider to the PDHS. We used chiropractic and physiotherapeutic treatments of hands, wrists, elbows and arms as outcome. To ensure that the registered treatment was more than just a trial visit in a newly available service, we defined outcome as having a second treatment within 30 days after the first treatment.
First diagnosis of rheumatoid arthritis (RA, International Classification of Diseases, 10th Edition (ICD-10): M05) and any upper extremity fractures (ICD-10: S42, S47, S52, S54, S57, S58, S62) were identified through the Danish National Patient Register.32 RA was included as a confounding risk factor from the date of diagnosis and onwards and fractures were included for a period of 2 years after diagnosis.
Statistical analysis
The cohort was followed from the first day of coverage in one of the 17 jobs in the PDHS from 1 October 2005 until the date of the second treatment within 30 days after the first treatment, the last day of registered coverage or 31 December 2017, whichever came first. A person was allowed as many periods of coverage as possible but a minimum of 30 days in total was required.
Poisson regression models were used to determine incidence risk ratios (IRRs) of treatment in relation to wrist angular velocity, use of hand force and job. The logarithm of risk time was used as offset value.
The main analyses included the exposures (wrist velocity and use of hand force) as continuous and categorical variables. The data revealed an apparent skewness of sex-distribution across quintiles of exposure, requiring us to split analyses into men and women. We also performed Spearman’s rank correlation analyses between wrist velocity and use of hand force in quintiles.
We also analysed sex-specific associations between job groups and seeking treatment. To ensure enough power, only jobs with >300 persons were included. For male job groups, forklift operators were the reference group and for female job groups office workers were the reference group (ie, the lowest exposed job group).
As sensitivity analyses, we adjusted results for educational level (elementary, high school, vocational, higher or unknown). The importance of outcome definition was evaluated by calculating IRRs based on first ever treatment. We had outcome information available for the year 2018, but without register information on the diagnoses of RA and fractures. The effect of an additional year of follow-up was investigated, but only with adjustment for age and calendar-year. Effect of time covered in the PDHS was investigated by restricting analysis to only those covered for >90% of the time. We examined sex-specific interactions between high/low exposure using median split.
We report results as crude and adjusted IRRs with 95% CIs. Adjustments were made based on a directed acyclic graph for age, age×age, calendar year, diagnosis of RA and upper extremity fractures within the last 2 years (model 1). Finally, we multiple adjusted for the two exposures (repetition or hand force) (model 2).
Data were analysed using SAS V.9.4 (SAS Institute, Cary, North California, USA).
Results
Cohort characteristics
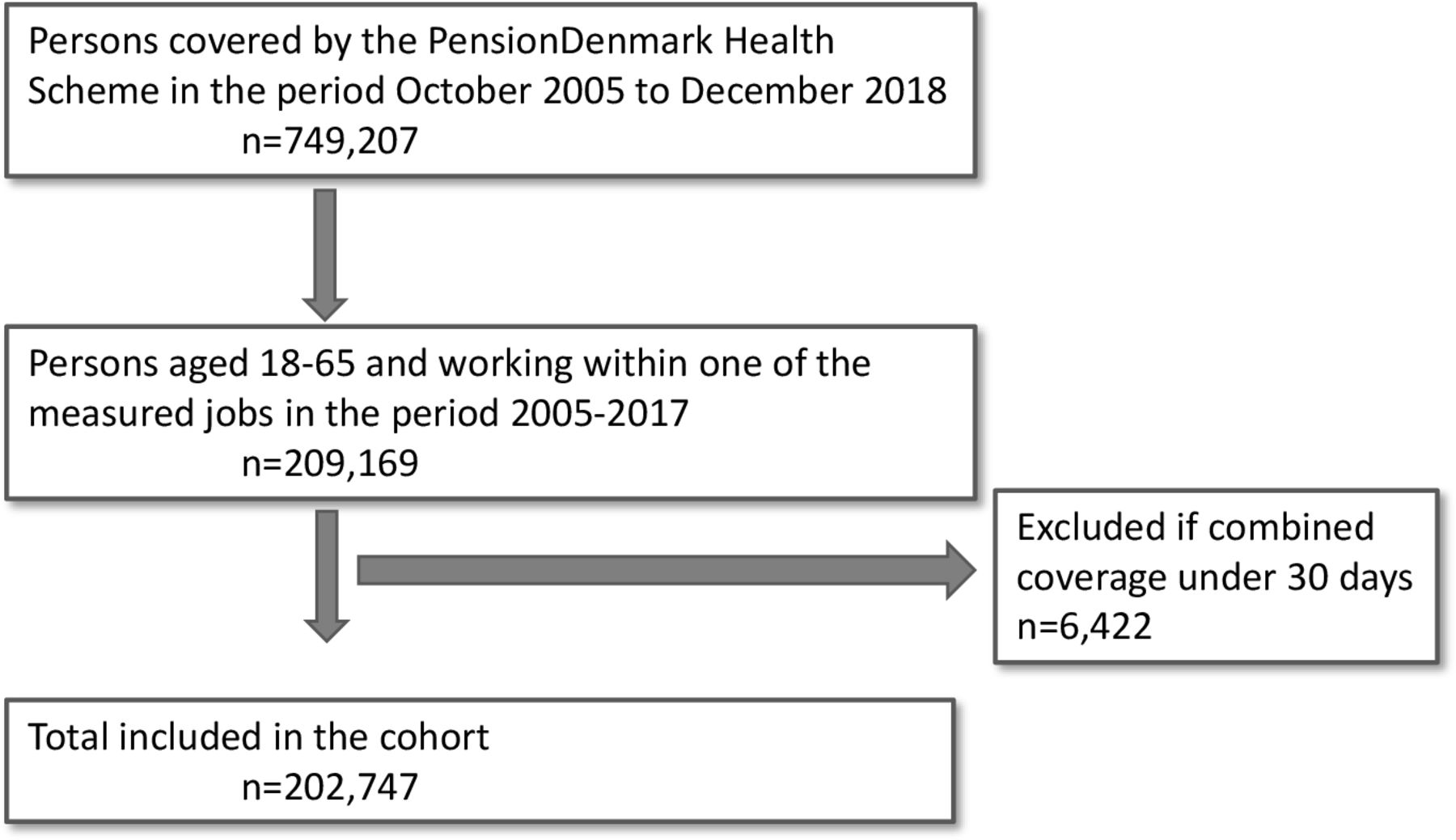
A total of 202 747 members were followed for 616 759.8 person-years (figure 1). Table 1 shows the characteristics of the 17 jobs whereof 3 jobs had measurements on both men and women. Almost 70% of the cohort was men. The age at entry was quite similar across jobs with hairdressers and pig farm workers as the youngest groups. The cohort members were followed for an average of 3.0 years with time covered as a truck drivers as the longest (4.4 years). Cohort members were covered in the PDHS for an average of 88% of the follow-up time.

Flow chart of the creation of the cohort.
Characteristics of the cohort: persons covered in the PensionDanmark Health Scheme in the period 2005–2017 aged 18–65 years
There was low correlation between quintiles of wrist angular velocity and hand/wrist force (Spearman’s correlation coefficient 0.04). Sex distribution varied considerably across quintiles of exposures (table 2). Men had more risk time with fractures than women and persons with RA were present in the cohort for only a very short time after the diagnosis. More than half of the cohort was skilled workers, 35.7% unskilled and 3.5% higher educated.
Distribution of potential confounders across quintiles of exposures
A total of 1085 first-time treatments was found, with elbows and arms (forearm or upper-arm) accounting for 86.4% of the treatments. Hands and wrists accounted for 4.6% and 9.0% of the treatments, respectively. The body regions did not differ between men and women. Men had a lower incidence rate than women of 15.3 vs 24.0 treatments per 10 000 person-years (table 3).
The risk of treatment for pain in the distal upper extremities with increasing levels of wrist angular velocity and exertion of force
Wrist angular velocity
Analysing wrist angular velocity as a continuous variable, we found a small but significant association among men in model 1 (table 3). Adjusting for force did not alter this result (model 2). Wrist angular velocity as categorical exposure had a significantly increased risk among men in the highest tertile compared with the lowest tertile, with an IRR of 1.48 (95% CI 1.15 to 1.92) in model 1. Estimates became insignificant after adjusting for hand force in model 2.
Among women, a significantly protective association with increasing wrist angular velocity was found in both models. Only the highest tertile was significantly different from the lowest in wrist angular velocity. However, the same jobs were categorised in high velocity and medium hand force and therefore the effect of adjusting for hand force was small.
Wrist force
The association between use of hand force and treatment was significant and unaffected by adjusting for wrist angular velocity among men, with an IRR of 1.50 (95% CI 1.38 to 1.63). Hand force had a clear exposure-response effect on the outcome in model 1, with an IRR of 2.23 (95% CI 1.83 to 2.72) and 2.65 (95% CI 2.13 to 3.29) in the second and third tertiles, respectively (table 3). This effect was still evident after adjusting for angular velocity.
Neither as a continuous nor a categorical variable was the use of wrist force positively associated with treatment among women in both models.
Job groups
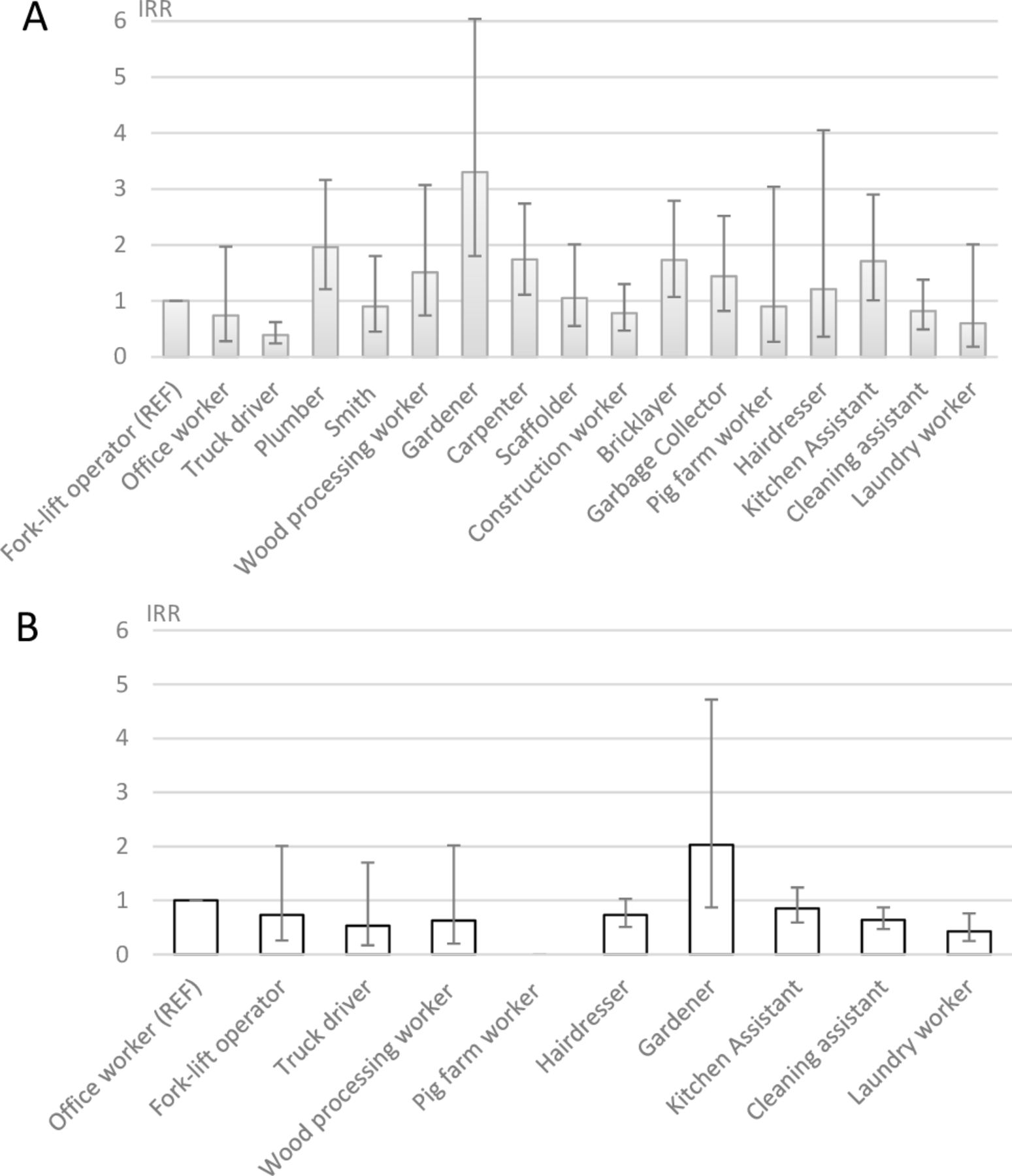
Figure 2 shows the sex-specific associations between job group and treatment in jobs with >300 persons represented. Incidence rates ranged from 6.2 to 65.9 per 10 000 person-years. Compared with fork-lift operators, several jobs showed a significantly higher adjusted IRR ranging from 1.71 to 3.30 among men (figure 2A). Truck drivers had a significantly lower risk of treatment for D-UEMSD. Among women, an increased risk, although non-significant, compared with office workers was found only among gardeners, IRR 2.03 (95% CI 0.87 to 4.72). Cleaning assistants and laundry workers had a significantly decreased risk with an IRR of 0.64 (95% CI 0.47 to 0.87) and 0.43 (95% CI 0.25 to 0.76), respectively (figure 2B).

{kind=link}
{kind=link}
Association between treatment for pain in the upper extremities and job title, adjusted incidence rate ratio (IRR) sorted by increasing wrist velocity. REF indicates reference group. (A) Men: job titles with >300 men. (B) Women: job titles with >300 women. Adjusted for age, age×age, calendar-year and diagnoses of rheumatoid arthritis and fractures of the wrist, elbow or arm.
Sensitivity analyses
Adjusting for educational level attenuated results, leaving only results among men statistically significant. Using the first ever treatment as outcome did not change the overall results, although the inverse association with categorical wrist angular velocity among women became statistically significant in model 2. An additional year of follow-up or restricting analysis to those covered for >90% of the time did not change the results. Fully adjusted interaction analyses with dichotomised high (H)/low (L) force (F)/velocity (V) for men showed an IRR of 3.88 (95% CI 3.09 to 4.87) for HF/LV, 2.36 (95% CI 1.77 to 3.15) for LF/ HV and 2.66 (95% CI 2.08 to 4.87) for HF/ HV. For women IRRs of HF/LV, LF/ HV and HF/HV were 0.44 (95% CI 0.14 to 1.42), 0.69 (95% CI 0.50 to 0.99) and 0.77 (95% CI 0.56 to 0.99), respectively.
Discussion
Key results
The aim of this study was to analyse whether repetitive and forceful movements were associated with pain requiring treatment in the arms or hands. With the use of a JEM based on objective measurements of repetitive wrist movements and expert-rated hand force, we found that the use of hand force, controlled for repetitive movements, increased the risk with an exposure-response pattern in men, but not in women. Increasing velocity of the movements of the hand, controlled for force, did not increase the risk of pain requiring treatment in neither men nor women. In fact, high velocity had a significant protective effect in women.
Limitations
Some methodological limitations must be addressed. Outcome definition was based on the reported anatomical region of concern by the treating physiotherapist or chiropractor at the time of treatment. This gives the advantage of being a real-time observation but may limit the specificity of the outcome. We anticipated that seeking treatment for pain in the hands, wrists, elbows and arms primarily represented disorders such as epicondylitis of the elbow and tenosynovitis of the hand or wrist. Treatment for functional limitations is also a possibility, although expected to be a minor part. However, we were not able to perform analyses on elbow and hands separately. This lack of specificity in outcome might have diluted the associations. The PDHS as a source of outcome is unvalidated and future studies are needed to confirm our results.
A possible bias could have been different care-seeking behaviour in job groups or between sexes, for example, because of accessibility or information.33 However, the population was homogenous regarding educational level why this bias may have been limited. The use of the PDHS was comparable to the use of physical therapy in the general population. According to Statistics Denmark, approximately 6%–8% of the Danish population had at least one treatment with doctor-referred physiotherapy annually in 2008–2018 compared with 5%–7% of the members in the PDHS in the same period.34 Also, leisure time physical activity was not known and may be an unmeasured confounder, but previously the confounding effect on pain outcomes have been minor.35
A JEM entails the risk of non-differential misclassification of individual exposure due to variation within groups compared with the variation between groups.36 37 The job groups were selected to represent large exposure variation to counteract the effect of such misclassification. Angular velocity was chosen over mean power frequency as the measurement of repetition, as it has been shown to be consistently associated with carpal tunnel syndrome, tendinitis and elbow disorders.19 38 The fewer job groups and a lower absolute number of events might explain the results among the women.
The expert-rated use of force did not take sex into account, which may have caused misclassification. As an example, male and female gardeners had quite different angular velocity but the same level of force in our JEM. This might represent a misclassification, as male gardeners typically perform more strenuous tasks than females. Comparison with a gold standard using objective measures of force, such as electromyography, is difficult due to lack of comparable studied jobs. However, as an example, hairdressers have been studied with electromyography and relatively high levels of muscular activity and low levels of rest were found compared with jobs traditionally considered to be forceful such as meat cutters.38 This was not reflected in the expert-rating of force of the hairdressers, exposing the difficulties in choosing the relevant exposure measure for force. The possible misclassification using the expert-rated force will in such case result in too low estimates and may to some extent explain the negative findings among women. The strength of this study is the prospective design and the use of objective exposure and outcome, avoiding recall bias. However, the methods used are crude and introduces non-differential biases and entails risk of attenuation of results and negative findings, such as among the women. Therefore, the positive associations found among the men are more reliable.
Interpretation
Our results among the men was in line with the results from other more recent prospective studies using both individual and group-based exposures, where a pattern of an exposure-response effect between force and a risk of D-UEMSD has been found. Thomsen et al used a task exposure matrix, prospectively, on the job titles of 3123 employees in 19 industrial settings and found insignificant effect of high repetition. Force, on an observer assessed 5-point scale, remained a significant risk factor when repetition was included in the model.39 Force was significantly associated with both self-reported pain and possible tendonitis based on physical examination. Harris et al followed 413 hand-intensive workers for 28 months in 3 months intervals for wrist tendinosis and found similar results of no association with any individualised measure of repetition adjusted for force.5 Per cent time spent in heavy pinch grip showed an exposure-response relationship after adjustment for repetition, although statistical power was low due to sample size. Nordander et al used wrist angular velocity and wrist extensor muscular activity from pooled studies in a cross-sectional design.38 Associations were found between angular velocity and prevalence rates of complaints in the right elbow and hand and symptoms of carpal tunnel syndrome in both sexes and medial epicondylitis among men only. However, the cross-sectional design did not allow for causal conclusions and no adjustments for force were made.
A systematic review where only 2/12 studies were prospective and a wide range of outcomes were included have found that force and repetition interact significantly.40 As combinations of exposures were limited in our study, interpretations of our interaction results should be done with caution, and the interaction effects between force and repetition needs to be confirmed in well-designed studies reducing the risk of recall bias. Our study cohort mainly consisted of organised, skilled and unskilled workers, and might only be generalisable to similar populations. However, as we used generic exposure variables and the range of exposure was wide, especially among men, covering both very low and very high exposed workers, the results may have broad application.
Future research on occupational exposure and D-UEMSD should focus on further disentanglement of repetitive movements, use of hand force to explore exposure-response associations and possible interactions. This should be possible by including additional jobs with goniometric measurements or applying expert-rated JEMs on large populations in prospective designs in order to close the exposure information gaps that now exist.
Conclusion
The purpose of this study was to investigate the association between repetitive movements of the wrist and the use of hand force and pain in the arm and hand. We found a weak association with repetition among men but without a clear exposure-response pattern and no association among women. We found that exertion of force was convincingly associated with seeking treatment among men. This was not found in women, probably due to some degree of exposure misclassification and a lower number of investigated job groups.
Data availability statement
Data from the JEM are available upon reasonable request. Data from the Danish national registers are available through online access at Statistics Denmark under standard conditions.
Ethics statements
Patient consent for publication
Ethics approval
In Denmark, register and questionnaire studies do not require approval by committees on biomedical research ethics. The project was approved by the Knowledge Centre on Data Protection Compliance under the records of processing regarding health science research projects within the Capital Region of Denmark (VD-2018-521).
Acknowledgments
The authors thank Henrik Enquist and colleagues at the Department of Occupational and Environmental Medicine, Lund, Sweden for hosting and providing access to the EMINGO database. They also thank PensionDanmark for providing access to the PDHS database for research purposes. They also thank Tine Steen Erichsen, Ellen Bøtker Pedersen and Jens Peter Bonde, Department of Occupational and Environmental Medicine, Bispebjerg and Frederiksberg Hospital, University of Copenhagen for expert-rating for the JEM together with the authors Charlotte Brauer and Jane Frølund Thomsen. Finally, they thank Thomas Heilskov-Hansen, Department of Occupational and Environmental Medicine, Bispebjerg and Frederiksberg Hospital, University of and Annett Dalbøge, Department of Occupational Medicine, Danish Ramazzini Centre, Aarhus University Hospital, for the collection of technical exposure measurements in Denmark.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Contributors JFT, CBL, LCT, CB, EMF and JAP designed the study and JAP, JFT and EMF acquired the data; JAP and EMF analysed the data and JAP drafted the manuscript; JFT, LCT, CBL, CB, EMF and JAP interpreted the data. All authors critically reviewed the draft for important intellectual content. All authors agreed to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Funding This study was supported by grants from the Danish Working Environment Research Fund (grant # 20175100917) and The Research Centre for Hairdressers and Beauticians (grant # 150217).
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.