Article Text

Abstract
There is consistent evidence of increased respiratory symptoms in occupational cleaners; however, uncertainty remains on type of respiratory health effects, underlying causal agents, mechanisms and respiratory phenotypes. We aimed to conduct a systematic review and if possible, a meta-analysis of the available literature to characterise and quantify the cleaning-related respiratory health effects. We searched MEDLINE and EMBASE databases and included studies that evaluated the association of any respiratory health outcome with exposure to cleaning occupation or products in occupational cleaners. A modified GRADE was used to appraise the quality of included studies. We retrieved 1124 articles, and after applying our inclusion criteria, 39 were selected for the systematic review. We performed a meta-analysis of the 21 studies evaluating asthma which showed a 50% increased pooled relative risk in cleaners (meta-relative risk (RR)=1.50; 95% CI 1.44 to 1.56). Population-based cross-sectional studies showed more stable associations with asthma risk. No evidence of atopic asthma as dominant phenotype emerged. Also, we estimated a 43% increased risk (meta-RR=1.43; 95% CI 1.31 to 1.56) of chronic obstructive pulmonary disease. Evidence for associations with bronchial-hyper-responsiveness, lung function decline, rhinitis, upper and lower respiratory tract symptoms was weaker. In our systematic review and meta-analysis, we found that working as a cleaner is associated with an increased risk of reversible and even irreversible obstructive airway diseases. All studies lacked quantitative exposure assessment to cleaning products; this would help elucidate underlying causal agents and mechanisms. Exposure control and respiratory surveillance among cleaners is warranted to prevent the associated respiratory health burden. Trial registration number: CRD4201705915.
- epidemiology
- public health
- respiratory
- meta-analysis
- occupational health
Statistics from Altmetric.com
Key messages
What is already known about this subject?
There is consistent evidence of increased respiratory symptoms in occupational cleaners worldwide. However, uncertainty remains on type of respiratory health effects, underlying causal agents, mechanisms and respiratory phenotypes.
What are the new findings?
We evaluated a broad range of respiratory health effects and estimated a 50% increased risk of asthma and 43% of chronic obstructive pulmonary disease among occupational cleaners. No evidence for a typical allergic respiratory phenotype emerged, suggesting that continuous exposure to irritant agents might cause both reversible and irreversible airway obstruction.
How might this impact on policy or clinical practice in the foreseeable future?
Enhanced exposure control and respiratory health surveillance among cleaners is warranted to avoid the associated respiratory health burden. All studies lacked quantitative exposure assessment to cleaning products; inclusion of such measures in prospective studies would help elucidate underlying causal agents and mechanisms.
Introduction
Occupational cleaners represent a significant proportion of the workforce in developed countries (about 4 million just in Europe), and mostly include ‘vulnerable’ social categories: women, migrants and low educated subjects.1 These figures are likely an underestimation given that many in this job sector are self-employed.
In the last decade, a consistent and growing evidence of an epidemic of ‘asthma-like’ respiratory symptoms among occupational cleaners has been reported worldwide.2 3 In addition, a recent large population-based study found an increased risk of spirometrically-defined chronic obstructive pulmonary disease (COPD) among cleaners, confirmed in never-smokers.4
Cleaners are exposed to a wide range of airborne agents that might contain either respiratory sensitisers or irritants.5 6 In particular, bleach and disinfectants have been associated with an increased asthma risk. However, most of the evidence is based on self-reported exposure that is likely to be biased towards cleaning agents with pungent odour so the causal agents remain unclear.7
In addition, the underlying mechanistic pathways are uncertain. There is no evidence of a classic IgE-mediated allergic asthma phenotype, so alternative pathways ranging from inflammatory to neurogenic have been proposed. Moreover, it is still largely debated whether persistent exposure to irritant agents in cleaning products could trigger and then sustain chronic airway inflammation with subsequent fixed airway obstruction.5 6
Given the uncertainty of causal agents, underlying mechanisms and type of respiratory health effects, we aimed to conduct a broad systematic review and if applicable a meta-analysis of the literature in order to characterise and quantify the respiratory health effects attributable to occupational exposure to cleaning products.
This is an important public health issue, also for the potentially important downstream implications for all end-users of cleaning products during domestic housekeeping, including vulnerable ‘bystanders’ such as children.
Methods
Literature search strategy, selection criteria and quality appraisal
We conducted the systematic review following the PRISMA guidelines, and we registered the search protocol in PROSPERO (CRD42017059150) on 21 March 2017. We searched the electronic bibliographic databases ‘Ovid MEDLINE(R) 1946 to 2017’ (PubMed) and ‘Embase 1947 to 2017’ on 24 March 2017. The search was then updated to 31 July 2020. OpenGrey database was also screened to retrieve ‘grey literature’ using broad, concise search terms covering the domains of ‘Occupational cleaning’ and ‘Respiratory outcomes’. The search strategy used free-text terms which were adapted for each database in combination with ‘MeSH’ filters where appropriate (online supplementary table S1). All studies examining occupational cleaning and exposure to cleaning products including disinfectants as the exposure and any respiratory disease, symptom or lung function measure as an outcome were eligible for inclusion. Of note, ‘cleaning products’ is used throughout this paper to designate the broader category of cleaning products and disinfectants. Healthcare workers performing cleaning job tasks were also included. To maximise the number of articles, there were no restrictions on the publication date, and PhD theses captured by the grey literature search were also included. Only articles written in English were included. Case reports, editorials, letters and reviews were excluded. Finally, studies on outdoor cleaners (eg, road cleaners) and cleaners working in industrial/factory settings were excluded as they were likely to have been exposed at workplace to other occupational respiratory toxicants (eg, isocyanates, food respiratory allergens, welding fumes, metals, gas, dusts, diesel exhausts and so on) or to use cleaning agents specific for industrial applications (eg, highly alkaline detergents for heavy industrial soiling). The full list of inclusion/exclusion criteria is in online supplementary table S2. Two authors (OA and SS) independently assessed the retrieved references against the inclusion criteria, and in case of disagreement, consensus was achieved by consulting a third reviewer (SDM). Endnote X7.1 was used as reference management software. Given that virtually the entire evidence in occupational epidemiology comes from observational studies, a modified GRADE system8 was used for the quality appraisal of the included articles. In particular, we considered ‘a priori’ as the best study design to assess a causal association a prospective observational cohort instead of a randomised clinical trial because not applicable in this occupational epidemiology context. All the other GRADE criteria were kept as per the original system, including the final scoring classification into high, moderate, low or very low.
Supplemental material
Statistical methods for meta-analysis
To quantify the cleaning-related respiratory health effects, we considered for meta-analyses the studies included in the systematic review that showed a high/moderate quality according to the GRADE scoring. We pooled the main reported effect measures between occupational exposure to cleaning products or cleaning occupation and each respiratory health outcome by using fixed-effects9 or random-effects methods10 as appropriate based on the Higgins I2 statistic. Significant within-studies heterogeneity is typically considered to be present if I2 is ≥50%.11 Also, subgroup analyses by epidemiological study type were performed. Pooled risk effect estimates were presented as meta-relative risks (RRs) and 95% CIs. The meta-analysis was performed using the command ‘metan’ in the statistical software STATA V.15.
Results
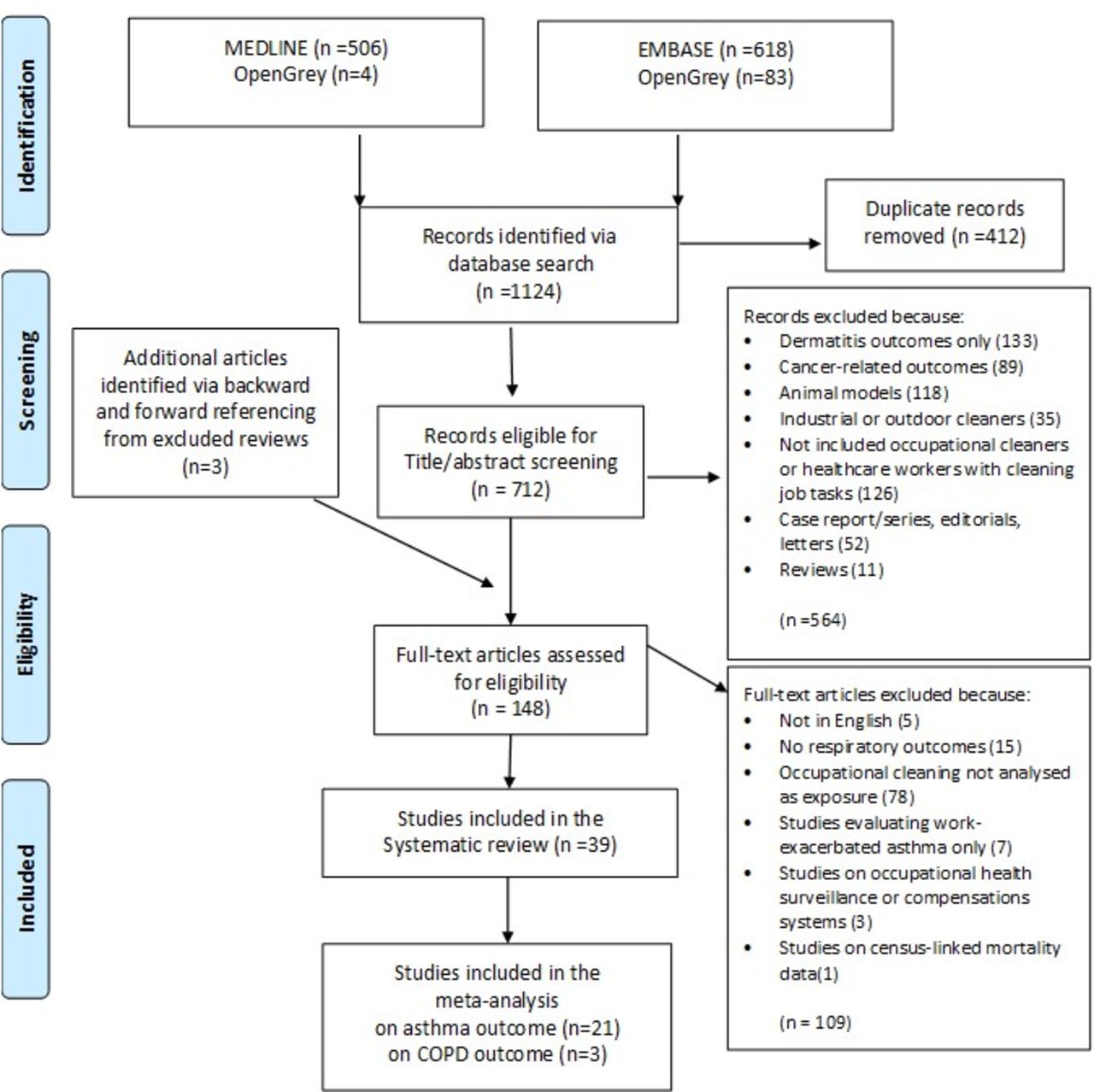
From our electronic database search, 1124 articles were retrieved. After removing record duplicates, 712 articles remained eligible for title and abstract screening. Of note, from forward and backward referencing of the removed review articles, we identified three additional records. After abstracts screening, 148 articles remained eligible for full-text article review. After applying our inclusion/exclusion criteria, 39 studies remained to be included in the final qualitative synthesis (figure 1).

PRISMA flow diagram showing screening and selection of articles related to occupational cleaning and health outcomes resulting from the search in electronic bibliographic databases.
Based on our quality appraisal, most of the studies included reached a moderate GRADE score (online supplementary tables S3–S5), the three studies included that were retrieved using OpenGrey scored very low in quality and we decided to not include them in the final systematic review (online supplementary table S6).
We managed to perform a quantitative meta-analysis among 21 high/moderate quality studies evaluating asthma risk and three high quality studies on COPD risk with comparable effect measures (figures 2 and 3, respectively). For the other evaluated outcomes, important differences in both exposure and outcome definition (eg, bronchial-hyper-responsiveness (BHR) defined using self-reported symptoms versus standard methacholine challenge test) prevented us from pooling these studies in a meta-analysis.
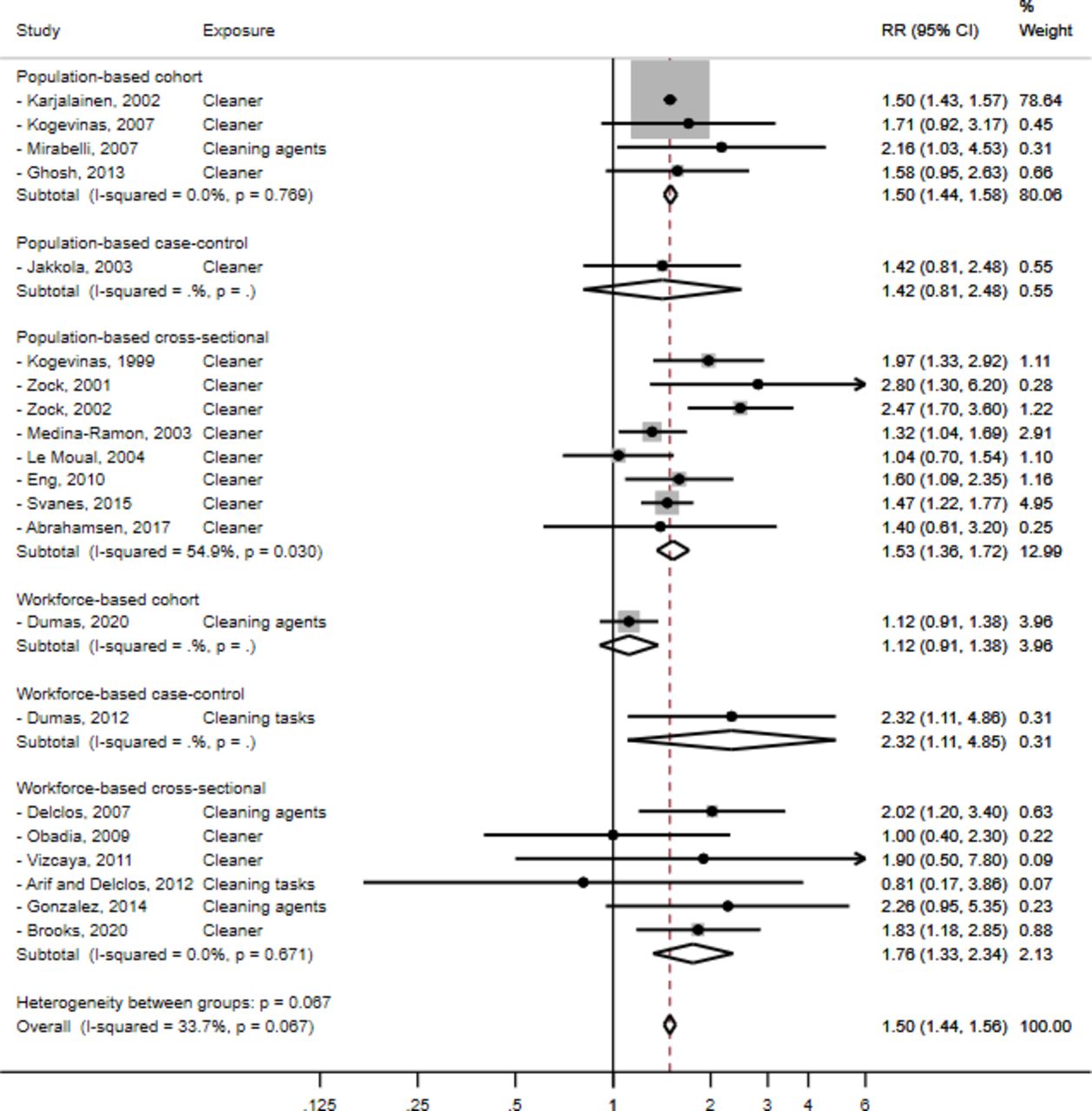
Meta-analysis of 21 studies evaluating the association between occupational cleaning exposure and asthma risk. RR, relative risk.

{kind=link}
{kind=link}
{kind=link}
Meta-analysis of three studies evaluating the association between occupational cleaning exposure and COPD risk. COPD, chronic obstructive pulmonary disease; RR, relative risk.
Respiratory health outcomes
Asthma
We included in the systematic review 21 studies evaluating associations between asthma and occupational cleaning (and/or exposure to cleaning products) conducted in a broad range of countries (Europe, USA, South America, Canada and New Zealand) in the last two decades (table 1). Thirteen studies were based on general population samples,12–24 and eight were conducted within workforces.25–32 The majority used a cross-sectional design. In terms of outcome definition, ‘adult-onset asthma’ among current or ever cleaners was mainly used as a proxy to define ‘occupational asthma’ or the broader category of ‘work-related asthma’ outcomes, based on a self-reported doctor’s diagnosis or asthma symptoms/medications. Of note, studies evaluating work-exacerbated asthma only were not included. Most of the studies used a standard job-title approach as proxy for occupational exposure to cleaning products. Six studies assessed exposure to specific agents included in cleaning products by using an expert-based exposure assessment or a semiquantitative job-exposure matrix approach.13 17 18 26 27 33 Evidence of a positive exposure-response relationship emerged by using duration of employment as a cleaner or frequency/intensity/duration of cleaning tasks as proxys for exposure. Most of these studies were conducted among hospital cleaners and evaluated frequency and intensity of exposure to disinfectants during cleaning tasks.21 25–27 None actually managed to measure cleaners’ personal exposure to cleaning agents, so no dose-responses based on concentration metrics were evaluated. Both population-based and workforce-based studies found a positive association between occupational cleaning and asthma risk. Among the eight workforce-based studies,25–32 mainly conducted among hospital healthcare workers, risk estimates were more instable because based on smaller samples. Of note, among healthcare workers emerged positive exposure-response trends for asthma risk and exacerbations for frequency of cleaning tasks, especially when applying disinfectants/sterilising agents.25 Exposures to ammonia and bleach showed the highest associations with asthma risk both in workforce-based and population-based studies.19 20 Also, cleaning products in spray format were found more strongly associated with asthma symptoms or asthma exacerbations compared with liquid and powder products. Of note, we did not include in the systematic review a French population-based case-control study that evaluated asthma severity only33 and a cross-sectional study of cleaners in Brazil because a composite outcome of asthma/rhinitis symptoms was evaluated.34
Summary of epidemiological studies (chronological order) assessing the associations between cleaning occupation, tasks or agents and asthma in population-based and workforce-based studies
Meta-analysis for asthma outcome
Based on our GRADE quality appraisal (online supplementary table S3), we selected 21 studies on asthma with high/moderate quality score for meta-analysis.
Where studies reported more than one risk effect estimate for asthma, we selected for quantitative summary the one that best-defined occupational asthma: for example, we favoured the effect estimate for asthma diagnosis after start work among current cleaners over estimates for ever adult asthma diagnosis among ever cleaners.
The population-based studies showed a clear increased risk of asthma among cleaners, irrespective of the study design, with the highest pooled risk estimate among cross-sectional studies (meta-RR=1.53; 95% CI 1.36 to 1.72). Workforce studies found positive, but less stable associations (ie, wider CIs), with the highest pooled risk among cross-sectional studies (meta-RR=1.76; 95% CI 1.33 to 2.34).
Overall, the pooled meta-analysis of the 21 studies, showed a 50% increased risk for asthma (meta-RR=1.50; 95% CI 1.44 to 1.56; I2=33.7%; p=0.07) (figure 2). Based on the heterogeneity tests between studies, fixed methods were applied to pool the risk estimates.
No evidence of publication bias or small-study effects was detected (Egger’s test p=0.23) (online supplementary figure S1).
Bronchial hyper-responsiveness
Among the three studies included in the systematic review that evaluated non-specific BHR as respiratory outcome among occupational cleaners a weak positive association was found (table 2).23 26 35 In particular, only one study found a clear association with BHR even if assessed using a symptoms score questionnaire instead of an objective a specific bronchial challenge test.26 One study found an association in ex-smokers only,22 and one did not find a statistically significant association.35 Two studies included in the systematic review were not included in table 2 because evaluated BHR only in a combined outcome with asthma symptoms.16 22
Summary of epidemiological studies (chronological order) assessing the associations between cleaning occupation, tasks or agents and BHR and UTRS and LTRS
Respiratory symptoms
Eleven studies (five workforce and six population based) investigated as outcomes lower (LRTS) and upper (URTS) respiratory tract symptoms, such as cough, wheeze or chest tightness, and itchy or runny nose, respectively (table 2).21 24 29 30 35–41 Eight of the 11 studies explored only LRTS and found an increased risk for higher duration of exposure and among those working as cleaners compared with controls. In one study, this increased risk was confined to women although no formal gender interaction was tested,29 while in another study, there was evidence of a positive exposure-response (OR of wheeze of 1.46; 95% CI 1.18 to 1.83 for exposure between 1 and 4 years and of 1.62 (95%CI 1.34 to 1.96) for exposure >4 years.21 One cross-sectional study in Spain showed increased risk of LRTS in cleaners, but failed to reach conventional statistical significance.30 Finally, one study found a significant increase in phlegm (p=0.019) and dyspnoea (p=0.041) suggestive for chronic bronchitis.35 Three studies assessed also associations with URTS. One study showed a doubled risk for eye/nose/throat symptoms;40 the second found associations confined only to medium and not high exposures which were attributed by the authors to the healthy worker effect.36 The third found a significant increase in nasal (p<0.001) and throat symptoms (p<0.05).38
Rhinitis
Two population-based studies reported the association of cleaning profession with occupational rhinitis as outcome19 42 and one workforce-based assessed associations with the composite outcome rhinitis/asthma34 (table 3); most have shown small and statistically not significant increased risks. Phenotypes of rhinitis were examined by one study that found increased risk of perennial rhinitis among cleaners, especially women (OR=1.70 (1.09 to 2.64).42 Similarly in Brazil, female cleaners only had higher risk of a composite outcome rhinitis/asthma (rhinitis defined as self-reported sneezing or runny or blocked nose, without cold or influenza over the past 12 months).34 Neither of these studies conducted formal tests for gender interaction. Evidence from a cross-sectional study in Spain on current and former cleaners (domestic and non-domestic) showed increased and significant associations with rhinitis only for former domestic cleaners.19
Summary of epidemiological studies (chronological order) assessing the associations between cleaning occupation, tasks or agents and rhinitis, COPD, lung function and other health outcomes
COPD
Three studies examined the association between occupational cleaning exposure and COPD risk.4 21 43 A significant association of working as a cleaner and having spirometrically-defined COPD (ie, forced expiratory volume in 1 s, FEV1/forced vital capacity, FVC <lower limit of normal, LLN) was found in a recent large population-based cross-sectional analysis of 228 614 people in the UK Biobank study. A 43% risk increase (prevalence ratio, PR=1.43; 95% CI 1.28 to 1.59) was found for cleaning occupation, also confirmed in analyses restricted to never smokers and non-asthmatics.4 Also, a cross-sectional study of 13 499 Northern European cleaners reported an increased risk of self-reported COPD diagnosis (OR=1.69; 95% CI 1.29 to 2.20).21 Finally, a very recent workforce-based prospective cohort study among hospital nurses in USA found an increased incidence of COPD (self-reported doctor-diagnosis) for exposure to cleaning products and disinfectants (HR=1.35; 95% CI 1.14 to 1.59) for weekly self-reported exposure to any disinfectant)43 (table 3).
Meta-analysis for COPD outcome
Overall, the pooled meta-analysis of these three studies4 21 43 showed a 43% increased risk for COPD (meta-RR=1.43; 95% CI 1.31 to 1.56; I2=0.0%; p=0.38) (figure 3). Based on the heterogeneity tests between studies, fixed methods were applied to pool the risk estimates.
No evidence of publication bias was detected (Egger’s test p=0. 60) (online supplementary figure S2).
Lung function metrics
Seven studies (table 3) evaluated as outcome lung function metrics decline in occupational cleaners.23 31 37 44–47 The majority did not find significant differences in lung function among cleaners compared with controls. For example, one large multicentre population-based study found a significant decrease of cross-shift peak expiratory flow (PEF) only,23 and another found lower cross-shift FEV1, and PEF among cleaners with current asthma only.45 However, a recent international population-based longitudinal study found an accelerated lung function decline among professional cleaners (FEV1: −22.4 mL/year; p=0.03, and FVC: −15.9 mL/year; p=0.002).47 Also, a very recent workforce-based cross-sectional study in New Zealand found a significant decline in lung function metrics among cleaners compared with controls.31
Other health outcomes
Among other health outcomes evaluated to better clinically phenotype the specific respiratory health effects among cleaners, atopy has been the one mostly investigated, because asthma is commonly allergy-based and cleaning products often contain potent IgE-mediated sensitising agents such as chloramine-T, ortho-phthalaldehyde and enzymes. One large multinational study showed a lower prevalence of atopy in cleaners compared with office workers (38.3% vs 60.9%; p<0.05).23 Of note, a workforce case-control study found higher atopy in cleaners with asthma than without (42% vs 10%, respectively), also associated with higher total IgE serum levels (geometric mean ratio: 2.9; 1.5–5.6).46
Fractionated exhaled nitric oxide (FeNO), a marker of airways inflammation and eosinophilic infiltration that has been associated with atopic asthma, has also been investigated. Three studies investigating FeNO in exhaled breath condensate after acute (preshift versus postshift) exposure to cleaning products containing chlorine did not found a significant difference between cleaners and controls.44 46 48 Of note, in one of them, a positive association of exposure to cleaning products with biomarkers of oxidative stress and inflammation (ie, malondialdehyde (MDA), 4-hydroxynonenal (4-HNE), nitrates (NO3-), in the exhaled breath condensate was found48 (table 3).
Grey literature
As above stated, the three studies included from searching the OpenGrey database were excluded from the final systematic review because of the low quality or missing information to assess the GRADE scoring (online supplementary table S6).
Briefly, one very small workforce surveillance study found increased asthma prevalence diagnosed via PEF diary among hospital cleaners.49 Another workforce survey found a non-significant higher prevalence of self-reported asthma and chronic bronchitis among hospital cleaners compared with administrative controls.50 A small population cross-sectional study showed a higher prevalence of BHR (based on histamine challenge test) and associated respiratory symptoms (eg, cough, phlegm, wheezing) compared with office workers.51
Discussion
Our systematic review examined for the first time a broad variety of respiratory health effects in association with occupational exposure to cleaning products.
We found a clear increased risk of asthma among occupational cleaners that we quantified by performing a meta-analysis into 50%. Of note, the majority (15 out of 21) of the studies included in the meta-analysis used cleaning occupation as a proxy for occupational exposure to cleaning agents and therefore were not susceptible to recall bias. Most of the studies were cross-sectional by design and evaluated asthma as self-reported doctor’s diagnosis or asthma symptoms; only a few managed to assess it by objective lung function tests. Also, supporting positive exposure-relationship by duration of employment or exposure (mainly self-reported) to cleaning agents was found.
Weaker positive associations were found for BHR, LRTS, URTS and rhinitis. In particular, BHR was increased among cleaners although within individual studies, this rarely reached conventional levels of statistical significance. Among the LRTS assessed, chronic cough and wheezing were reported as increased among cleaners, often when evaluated in association with an asthma diagnosis. Among the URTS, a weaker, but interesting, association with inspiratory breathing suggestive for irritant vocal cord dysfunction was found. Also, rhinitis was inconstantly found increased among cleaners, and only when associated to exposure to high molecular weight allergens in cleaning agents.
Interestingly, the majority of studies did not find an association with single lung function metrics as outcomes, namely FEV1, FVC and FEV1/FVC ratio. This is maybe due to well-known low sensitivity of occasional spirometry tests to detect occupational asthma or suggesting that if asthma-like symptoms arise in cleaners, it may not be due to airway obstruction but to other underlying mechanisms. Of note, a recent international population-based longitudinal study reported significant lung function decline associated with cleaning work that would support long-term respiratory health-effects.47
In addition, we found an increased COPD risk for cleaning occupation that we managed to quantify into 43% based on three high quality large population-based studies. It is noteworthy that the largest of the two used a spirometry-based definition of COPD and managed to confirm these findings in both never smokers and non-asthmatics, so ruling out residual confounding by both tobacco and asthma. This result is important because COPD has been largely linked to other occupational exposures such as generic VGDF (ie, vapour, gas, dust, fumes) exposure, but the evidence for cleaning agents is still scarce.
In relation to the potential associated respiratory phenotypes, no clear association with allergy or exhaled FeNO (ie, biomarker of airway inflammation in patients with asthma) was found, but an association with biomarkers of oxidative stress and inflammation (ie, MDA, 4-HNE and NO3-) was reported.
Among the evaluated potential causal agents, chlorine-based cleaning products, such as bleach were found associated with increased asthma risk,37 but also ammonia, quaternary ammonium compounds, disinfectants and sterilising agents such as ethanolamide, and glutaraldehyde, especially among healthcare workers performing cleaning tasks.27 As expected, cleaning products in spray format were associated with an higher asthma risk.22 Nevertheless, the lack of personal quantitative exposure assessment to the above agents and their pungent odour make these findings potentially susceptible to recall bias.
Overall, our findings seem to support the still debated hypothesis that cleaning-related respiratory health effects may be caused via irritation rather than immuno-mediated underlying mechanisms. As previously suggested,52 chronic exposure at relatively moderate doses, such as among occupational cleaners, to airborne irritative chemicals could cause inflammation and subsequent bronchoconstriction. Also, our results suggest that if exposure at work to noxious cleaning agents persists a reversible airway obstruction could become irreversible. This is confirmed by studies included in this review that found a positive exposure-response relationship by employment duration and frequency/intensity of exposure to cleaning-tasks.21 25–27
Our systematic review has several strengths. It evaluated a broad range of respiratory health effects and associated phenotypes, and it aimed to be very comprehensive by including also grey literature, as confirmed by the absence of publication bias. Also, we evaluated the evidence quality by applying a standard quality scoring system slightly modified to be suitable to appraise occupational epidemiology evidence. Finally, we managed to quantify a pooled risk estimate for asthma and COPD outcomes that can be used to inform public health interventions and future similar studies on the topic.
Limitations include the exclusion of articles not in English language. Also, misclassification of both exposure and outcome cannot be ruled out, and not all studies adjusted for the same potential confounders. However, both the meta-analysis for asthma and COPD outcomes among the selected studies showed a low heterogeneity that allowed us to use fixed-effect pooling methods.
In conclusion, in our systematic review, we found that occupational exposure to cleaning product is associated with several respiratory health effects, including both reversible and irreversible airway obstruction, and the suggested causal association is supported by evidence of positive exposure-response trends.
These findings have important potential public health implications: preventive measures to avoid, or at least reduce exposure to cleaning agents at workplace should be implemented, and respiratory health surveillance should be strengthened among this category of workers in order to detect early signs of respiratory health effects and so avoid any subsequent morbidity and disability. In addition, according to the precautionary principle, important downstream implications for all end-users of cleaning products during domestic housekeeping could be to suggest reducing exposures to ‘as low as possible’, especially to protect vulnerable subjects such as children from potentially harmful 'bystander' exposure. Our findings are particularly relevant in the current COVID-19 pandemic. Use and exposure to cleaning products in the general population has globally increased for infection control. We recommend adding to pandemic guidance documents information on cleaning-related respiratory health effects and on safe use of cleaning products to prevent the associated public health burden.
Further studies, ideally prospective cohorts using more precise quantitative exposure assessment of individual cleaning agents (eg, exact chemical composition by use of product bar codes), detailed clinical phenotyping (eg, airway inflammatory and immune biomarkers) and modern molecular methods (eg, metabolomics) would help clarify both the underlying causal agents and the relevant biological mechanisms. Filling this knowledge gap would allow implementation of effective focused preventive intervention strategies aimed to eliminate or at least control exposure to hazardous cleaning agents and identify early health effects to prevent the associated occupational respiratory health burden with important personal, medical and societal benefits.
Ethics statements
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Deceased SS since deceased
Contributors SS performed the systematic review as part of his BSc Research project at Imperial College London under the supervision of SDM and OA, and his work was key to write the present work. SS died before this article was prepared in its current form. SS and OA performed the literature review. SDM and DJ designed the project. SDM performed the meta-analyses. DC performed the literature search update and related tables’ amendments. SDM, OA, DC and DJ revised and approved the manuscript.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.