Article Text

Abstract
Objectives To assess if improvement of working conditions related to heat stress was associated with improved kidney health outcomes among sugarcane harvest workers in Chichigalpa, Nicaragua, a region heavily affected by the epidemic of chronic kidney disease of non-traditional origin.
Methods Based on our findings during the 2017–2018 harvest (harvest 1), recommendations that enhanced the rest schedule and improved access to hydration and shade were given before the 2018–2019 harvest (harvest 2). Actual work conditions during harvest 2 were then observed. Serum creatinine (SCr) was measured before and at end-harvest, and cross-harvest changes in estimated glomerular filtration rate (eGFR) and incident kidney injury (IKI, ie, SCr increase by ≥0.30 mg/dL or ≥1.5 times the baseline value) were compared between harvest 1 and harvest 2 for three jobs with different physical workloads using regression modelling. Workers who left during harvest were contacted at home, to address the healthy worker selection effect.
Results In burned cane cutters, mean cross-harvest eGFR decreased 6 mL/min/1.73 m2 (95% CI 2 to 9 mL/min/1.73 m2) less and IKI was 70% (95% CI 90% to 50%) lower in harvest 2 as compared with harvest 1 data. No such improvements were seen among seed cutters groups with less successful intervention implementation.
Conclusion Kidney injury risk was again elevated in workers with strenuous jobs. The results support further efforts to prevent kidney injury among sugarcane workers, and other heat-stressed workers, by improving access to water, rest and shade. The distinction between design and implementation of such interventions should be recognised.
- renal
- international occupational health
- climate
- workload
- intervention studies
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Key messages
What is already known about this subject?
In Mesoamerica, a region struck by an epidemic of chronic kidney disease of non-traditional origin, workers conducting heavy physical labour in the heat, particularly sugarcane harvest workers, are at high risk of experiencing reduced kidney function.
What are the new findings?
In burned cane cutters, the proportion of workers with kidney injury decreased following an enhanced rest schedule and improved intervention implementation.
Effective interventions require both adequate design and implementation.
How might this impact on policy or clinical practice in the foreseeable future?
The findings strengthen the need to increase efforts to prevent kidney injury among heat-stressed workers, while continuing to evaluate the effectiveness of available interventions.
Introduction
Central America, and especially its agricultural workers, suffer from an epidemic of chronic kidney disease of non-traditional origin (CKDnt),1 also known as Mesoamerican nephropathy.2 Similar epidemics occur in other tropical regions.3 Hypothesised aetiologies include heat stress/dehydration from strenuous work in heat with insufficient protections,4 pesticide toxicity5 and infection.6 Important gaps in our understanding of these epidemics exist, for example, their geographical extent and if they represent one single global epidemic, and what the impact of improved working conditions would be.7 This uncertainty, and a recent review of Mesoamerican CKDnt studies concluding occupational heat stress is associated with decreased kidney function and injury,8 an association increasingly recognised in experimental studies,9–11 motivate intervention studies addressing the heat hypothesis.
The Adelante Initiative12 Intervention Study aims to assess the impact of evidence-based recommendations designed to improve work conditions and reduce kidney dysfunction among sugarcane workers. The long-term goal is to adapt findings in this setting to other at-risk occupations and geographies. For harvest 1, November 2017–April 2018, of the Adelante Initiative we have described the existing work conditions and existing preventive measures and found that workers with the physically most demanding job had substantially higher risk of serum creatinine (SCr) increase over the cane harvest than those with less strenuous work but otherwise similar working and living conditions.13
This paper describes harvest 2, November 2018–April 2019, of the ongoing study, during which enhanced measures to prevent heat stress were introduced. The objective was to assess whether work conditions improved and assess if renal health outcomes improved conjunctively.
Methods
Study setting
This study was conducted at the San Antonio sugar mill (ISA) in Chichigalpa, Nicaragua, a known CKDnt hotspot. The climate in northwestern Nicaragua during November–April is hot and humid. Median wet-bulb globe temperature in the sugarcane fields reaches 30°C at about 10 am13 (ambient temperature 34°C) and 31°C at 2 pm (ambient temperature 37°C).
Study population and data collection
As in harvest 1,13 we included half the employed drip irrigation repair workers (IRW), all seed cutters (SC) and burned cane cutters (BCC), and the field support staff (FSS) associated with these work groups. All workers were organised into 60-person groups (cuadrillas). In harvest 2, we added four additional jobs (weeders, seeders, reseeders, gravity irrigators). Data on these workers will be presented separately as they do not contribute to evaluation of intervention enhancements.
Harvest work applicants were recruited in October 2018 during the company’s routine pre-employment health screening. Our staff explained the study objectives and procedures to all workers and answered questions before participants signed an informed consent. Non-fasting morning serum samples, and first void urine samples at workplace were collected. One aliquot each of serum and urine samples were analysed directly at the mill hospital laboratory. Samples were also sent to Lund University, Sweden.
All hiring decisions were the purview of the mill. Men with SCr >1.30 mg/dL or uric acid >7.0 mg/dL and women with SCr >1.00 mg/dL or uric acid >5.7 mg/dL were not hired. Tests could be retaken once if above SCr cut-offs. The generally recommended SCr reference interval for men is 0.90–1.30 mg/dL and for women is 0.60–1.10 mg/dL (18–60 years and SCr analysed by the Jaffe method).13 14 Other conditions leading to participants not being hired included haematocrit <35%, proteinuria and haematuria, inadequately controlled diabetes or hypertension, other health reasons and changing workforce demands.
Our interviewers administered a questionnaire covering demographics, medical history, symptoms over last 2 weeks, liquid intake since previous morning, personal habits, occupational history, medication, infectious disease occurrence and pesticide exposure at baseline and end-harvest. The harvest 1 questionnaire was used in harvest 2, adding questions about residential water source, cause of and duration of sick leave and hospitalisation during this and the past harvest, plus questions about fever: frequency during harvest, and duration, time of onset, perceived cause of most recent episode (sun, influenza, other infection or open-ended alternative). Height (just baseline), weight, blood pressure and heart rate were measured at baseline and at end-harvest. End-harvest and baseline examinations were performed early before starting work.
Chartered buses transported workers between residential areas and work sites. These bus routes changed from harvest 1 to harvest 2, a decision unrelated to the study but which eliminated some workers hired in harvest 1 who did not apply for work again (online supplementary table 1). Efforts were made to bring these workers back for testing even though they did not apply for a job for harvest 2.
Supplemental material
In both harvests, ISA monitored worker kidney health and heat stress. At mid-harvest 2, approximately 75% of all hired workers (smaller proportion of FSS, see online supplementary table 2) had SCr measured. Health promoters educate workers about heat stress and dehydration, deal with simpler injuries and symptoms and can refer unwell workers to the mill hospital for SCr testing.6 15 Workers with elevated SCr are sent on sick leave and can return to work if their SCr normalises (below employment cut-offs). Cutters had a health promoter with their cuadrilla daily, IRW every other day. Two mobile health clinics followed the field workers, with one permanently assigned to BCC. SC were prioritised for the other mobile clinic, while IRW had irregular access. Mobile clinic staff monitors hydration among some workers each day by observing liquid intake, urine output, body weight and dipstick urine density. A heat acclimatisation period was standard practice at both harvests.
At end-harvest harvest 2 (April 2019), all participating workers still employed at ISA were invited to a follow-up examination, with a repeated questionnaire plus serum and urine sampling. Samples were sent to ISA’s lab (anonymised for mill staff) to return results to participants immediately, and to the Swedish laboratory. Serum was separated from cells at the ISA laboratory, aliquoted and frozen at −77°C before transportation. Serum analyses of creatinine, cystatin C, albumin, sodium, C reactive protein, urea and uric acid were performed at Skåne University Hospital in Lund, Sweden, on a Cobas 701 instrument (Roche Diagnostics, Basel, Switzerland). Each individual’s baseline and end-harvest sample were analysed during the same session.
We attempted home visits for all hired workers absent at end-harvest testing (dropouts) to ask why they left work and administer a shortened end-harvest questionnaire. Information about pesticide use and fever during harvest 2 supplemented questions used after harvest 1. No biospecimens were obtained.
Outcome definitions
Glomerular filtration rate was estimated (eGFR) using SCr and the CKD-EPI formula.16 Incident kidney injury (IKIMeasured) was defined as SCr increase by ≥0.30 mg/dL or ≥1.5 times increase from baseline to end-harvest, a magnitude corresponding to acute kidney injury.17 This outcome has been used in similar studies13 18–20 and shown to predict persistent SCr increase.13 18 Located dropouts who reported leaving due to SCr elevation were considered having IKIReported, which combined with IKIMeasured gave the composite outcome IKIAll. For confirmation, we reviewed the mill hospital records of IKIReported workers where most sought care.
Explanatory variables
Job
Workers were asked at baseline what job they applied for and at end-harvest they were asked to verify that this was the job in which they had worked. Ninety-seven per cent (online supplementary table 2) of those followed-up reported having worked in the job they applied for. The job reported at end-harvest was used for the remaining 3%. Those with missing data on this variable at end-harvest (n=6) were considered to have been working in the job applied for. Those who reported changing to a job other than the four studied were excluded (n=9).
The tasks, personal protective equipment and ranked physical workload of each job have been described previously.13 Preliminary heart rate measurements of job-specific workload supported our qualitatively ranked order of physical workload previously reported (burned cane cutting >seed cutting >irrigation repair and field support work). Details of quantitative workload assessments will be described in a forthcoming publication after further data collection.
Liquid intake
Workers fill their personal 5 L thermos with purified water at the mill’s water station at the start of each workday. On each bus transporting a cuadrilla to the field, there was a 200 L barrel. In the field, there were generally two shade tents (open on two sides) for IRW, and three for cutters per cuadrilla, each tent housing a 40 L water cooler from which the workers could refill their personal thermoses during work. The distance to the bus or shade tent was approximately 200 m for IRW and 50 m for cutters.
Bolis are 300 mL electrolyte solution bags containing 7 g of sugar, 50 mg sodium chloride and 20 mg potassium monophosphate per 100 mL. These bolis were kept in coolers in the shade tents and workers were encouraged to drink one boli per break. The water supplied during work and used for boli production is supplied from the mill’s tested purification facility.21 Sugar-sweetened drinks mostly consist of frescos (fresh diluted fruit juice with substantial amounts of added sucrose). Cutters were provided with a fresco and lunch.
Intervention design
Based on observations from harvest 1, we made recommendations ahead of harvest 2:
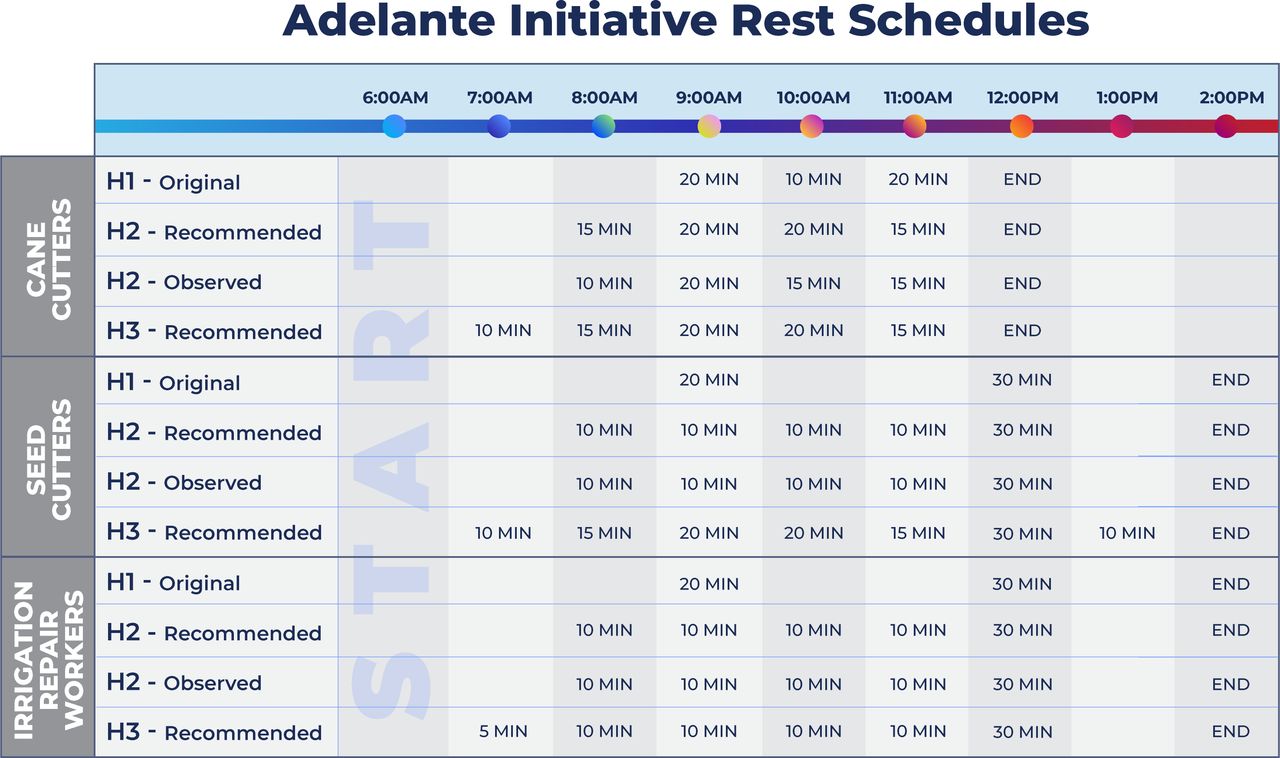
20 min more rest per workday for all jobs (figure 1), more evenly distributed throughout the shift and introducing an earlier break.
Move shade tents and fluid throughout the day to ensure these are ≤50 m from every cutter (<75 m for other workers).
Rotate shade tents so that closed sides face sun.
Increase number of tents to assure fewer than 15–20 workers per 4×4 m tent to improve:
Fluid accessibility.
Heat dissipation.
Improve fluid taste:
Aerate chlorinated water.
Eliminate disliked boli flavours.
Give more attention to boli distribution and consumption.
Change tent material from black to green fabric.
Cutting should start ≥12 hours after a field was burned to reduce radiant heat.
Reduce non-steroidal anti-inflammatory drug (NSAID) use.
{kind=link}
Rest schedule. H1, harvest 1; H2, harvest 2: H3, harvest 3.
Intervention implementation assessment
An occupational hygienist (EAM), experienced in sugarcane industry working conditions, observed working conditions for the different jobs (at least 1 day per job) in March, taking notes on rest schedule enforcement and use of and access to fluid, tents and sun-protective clothing and general working conditions. For a post hoc analysis, the mill OSH manager (blinded to our results) assessed compliance of each cutter cuadrilla with the recommended intervention.
Statistical analysis
Continuous covariates were described by job using means and SD or medians and IQR. All analyses were done using Stata V.15.
Kidney health outcomes
Continuous eGFR
We modelled eGFR in each worker (i) at each time point (t, baseline and end-harvest harvest 1 and 2, that is ≤4 observations per worker) using mixed effects linear regression. An unstructured covariance matrix with random intercept and slope for each worker was used. Separate models were run for each job and included fixed effects for sex and age (10-year bands) and dummy variables for test occasion (Equation 1). Cross-harvest trends (Δ) and the difference in these cross-harvest trends (Δ′) with 95% CI were estimated from the coefficients in these models (Equation 2-4) using the lincom command. Analyses were restricted to workers with serum samples both in beginning and end of ≥1 harvest.
 1
1
 2
2
 3
3
 4
4
Incident kidney injury
Risk ratios with 95% CI for harvest 2 compared with harvest 1 within each job were calculated.
Liquid intake
Mixed linear regression models with random effects for worker were used to compare reported 1 day liquid intake between harvests within each job. A zero-inflated Poisson model was chosen to compare the number of bolis reportedly consumed at end-harvest 1 and 2, as certain individuals may completely avoid drinking bolis, while those who drink bolis often drink many. Worker was used as a clustering variable. Models were run separately for each job. The margins command was used to estimate the number of extra bolis drunk in harvest 2.
Results
Participation
A total of 427 and 488 workers participated at baseline and end-harvest for harvest 1 and 2, respectively. Including dropouts not attending end-harvest testing but later interviewed in their homes, data were collected from 525 and 567 participants in harvest 1 and 2, respectively. Of the workers recruited in harvest 2, 8% were completely lost, 12% were contacted in their home for follow-up without providing samples, 78% provided samples at the end-harvest and the remaining 2% changed to another job, refused or had no samples (table 1 and online supplementary table 2).
Participation and outcome in harvest 2, reported by baseline, and by end-harvest job
Of the 427 workers who completed baseline and end-harvest testing in harvest 1, 204 also completed baseline and end-harvest testing in harvest 2. Regarding follow-up that included dropouts contacted after harvest (525 in harvest 1), 243 had such follow-up also in harvest 2. Workers mostly returned to their previous job (online supplementary table 1).
Main findings
BCC were all males, a quarter of the SC were women and field support and IRW had an even sex distribution (table 2). Age and baseline eGFR differences between jobs were small. Few workers reported pesticide use during harvest. Reporting fever during harvest was similarly common among all jobs, but more often attributed to sun exposure among cutters.
Background data by job
IKIMeasured and IKIReported occurred primarily among male cutters (table 1). One IKIMeasured event was in a female seed cutter, and one was in a FSS while two IKIReported events occurred among IRW (one female).
Modelled mean eGFR decrease over harvest 2 was similar for all jobs, at approximately 3 mL/min/1.73 m2 (table 3). Cross-harvest eGFR trends improved comparing harvests 1 and 2 for BCC, along with a strong and statistically significant decrease in IKI rates. For SC, eGFR trends and IKI rates remained similar comparing harvests. Among SC, all 13 IKIMeasured and all but two IKIAll events occurred in two of their four cuadrillas. FSS and IRW had similarly low IKI rates and small cross-harvest eGFR decline across both harvests, although the decline was slightly larger in harvest 2. Descriptive analyses restricted to workers participating in both harvests showed a similar pattern (data not shown).
Outcome comparison between harvests 2 and 1
ISA hospital medical records during harvest 2 could be found for 8/13 workers with IKIReported. All eight workers had SCr elevations corresponding to the IKIMeasured criteria, with a median 2.5-fold SCr increase compared with baseline.
Intervention enhancements
The harvest 2 intervention provided for enhanced and more evenly distributed scheduled rests, although intervention design differed between jobs and actual implementation likely varied between cuadrillas within jobs. All jobs had been recommended an earlier first break (8 am rather than 9 am), BCC expanded hourly breaks, and the other jobs changed to 10 min hourly breaks rather than one single 20 min break (figure 1).
The observations of working conditions during harvest 2 suggest that guidelines concerning water, rest and shade were adhered to relatively well on the days of observation. Self-reported water and boli intake increased from harvest 1 to harvest 2 for all jobs except FSS (table 4), and NSAID consumption decreased (table 2).
Comparison of self-reported hydration indicators per 24 hours between harvests 2 and 1
Discussion
Key findings
Harvest 2 findings confirm those from harvest 1—cutters, who have the highest workload, have the highest IKI rates. The enhanced heat stress prevention intervention, when properly implemented, seems to reduce kidney injury risk.
Recommendations for increased and more evenly distributed rest (figure 1), and advice on providing improved access to shaded rest, water and electrolyte solution was associated with a dramatic drop in IKI rate and eGFR decline from harvest 1 to harvest 2 among BCC. These results agree with previous results from a pilot study among sugarcane cutters in El Salvador, suggesting eGFR declines halted after improved access to water, rest and shade.22 23
Information from mill officials indicates that conditions were especially harsh for BCC towards the end of harvest 1. Two mechanical harvesters broke down mid-harvest, requiring rushed BCC recruitment. Consequently, existing preventive resources, such as mobile clinics, health promoters, shade tents and liquid coolers were were shared with new hires, therefore reduced among the BCC included in our cohort, possibly contributing to poorer harvest 1 results. If so, then the improvements documented after harvest 2 for BCC could be the result of a combination of substandard adherence to intended preventive measures during harvest 1 and an effect of the recommendations given ahead of harvest 2. Irrespective of why working conditions may have improved, the IKI reduction indicates that kidney injury may be prevented by improving water, rest and shade access.
SC did not improve nor worsen significantly from harvest 1 to harvest 2 as a working group. While there was an overall decrease in eGFR trend, IKIMeasured rates increased slightly. BCC received disproportionate attention to intervention implementation due to the problematic harvest 1 findings which may have contributed to less focus on SC. The blinded assessment of cuadrilla intervention compliance by the mill OSH manager indicated that the seed cutter cuadrilla with the worst compliance had the most cases of IKIAll whereas the cuadrilla with the best compliance had only one case (online supplementary table 3).
Workers reported larger water and boli intake in harvest 2 than in harvest 1 (table 4). Self-reports were compared with data routinely collected by the mobile clinic staff on how much workers drank during work shifts; the overall water and boli intake reported by this staff was only slightly lower than workers’ self-report. Volumes are substantially smaller than the median intake of 15 L of water and 3 L of hydration solution reported from a Guatemalan sugarcane worker cohort which did not fully prevent loss of kidney function.24 Dehydration is just one aspect of heat strain.25 The health effects of hyperthermia not prevented by adequate hydration25 may have been partially addressed in our study population by the improved rest/work schedule and easier access to shade. The importance of break frequency and duration is being further studied. Ten-minute breaks, as instituted for SC, may not be enough to limit hyperthermia, and the remaining 90 min non-interrupted work during the hottest hours after the lunch break may be detrimental.
None of the eight workers reporting pesticide use had IKI. Smoking was common among male sugarcane workers, but, unlike a previous report,26 not associated with kidney injury: the unadjusted incidence ratio for current smokers in all workers combining harvests 1 and 2 data was 1.1 (95% CI 0.6 to 2.0). Among SC over both harvests, there has been only 1 IKIMeasured event in 88 woman-harvests, compared with 17 in 223 man-harvests (Fischer’s exact p value=0.03). While this difference could be due to physical workload differences or women having a stricter SCr pre-employment cut-off, it should be further investigated.
Limitations
As in all longitudinal studies, loss to follow-up can reduce power if non-differential or introduce bias if differential. Having the same workers in harvest 2 as in harvest 1 would have increased power but it is unlikely that the change in bus routes differentially influenced comparisons between harvests. Some workers were also lost due to developing creatinine elevation between baseline examinations, and for other reasons that are not known to us, illustrating the difficulties of conducting a longitudinal study in this setting.
In contrast, loss of follow-up for workers leaving during the harvest is differential as many dropouts leave due to SCr elevation, leading to healthy worker selection bias unless dropouts are tracked. Larger proportions of dropouts occurred in some jobs (notably IRW) in harvest 2 than harvest 1, but complete loss-to-follow-up was still low.
Individuals prone to kidney injury would less likely be hired as pre-employment screening may have eliminated from harvest 2 workers experiencing kidney injury in harvest 1, thus contributing to less kidney injury in harvest 2. However, the pre-employment SCr cut-off was used also ahead of harvest 1. Hence, such bias is unlikely to explain the improvement seen among BCC and compliant SC cuadrillas in harvest 2. After harvest 3, we will attempt to measure SCr levels in cohort members with any prior biological measurements.
Conclusions
This study describes the second harvest of the ongoing Adelante Initiative Intervention Study, laying the basis for further effectiveness evaluation, pathophysiological studies on heat stress and kidney injury and understanding long-term prognosis for individual workers.
The drops in IKI rates and attenuated eGFR decrease among BCC and compliant SC cuadrillas are compatible with a beneficial effect of improved working conditions addressing heat stress, potentially attributable to more and longer rest periods to manage hyperthermia and increased liquid intake to manage dehydration. Better implementation of already existing preventive efforts that were not applied as intended during harvest 1 is another possible contributor. However, adequate monitoring of intervention implementation in harvest 2 was impeded by the violence and civil unrest in the study area.27 28 Regardless, recognising potential discrepancies between intervention design and implementation is essential for adequate interpretation of intervention study results and for employers who wish to protect their workers.
Progressively improving work conditions (figure 1) and close monitoring for longer periods is key to evaluating the full impact of reduced heat stress on kidney health. Considering rising global temperatures and increasing evidence linking heat stress with kidney injury,8–11 more intervention studies are urgently needed among vulnerable heat-stressed workers in different settings. The logistical and methodological challenges facing such pragmatic intervention studies should not be a deterrence to undertaking such studies, especially considering these initial promising results.
Acknowledgments
The authors would like to thank Scarlette Poveda and Fatima Cerda for local coordination, data entering and management, William Martinez for local coordination and locating and interviewing dropouts, and all other staff involved in data collection, as well as Ernesto Ariza for help in designing the graph and Aurora Aragon for reviewing the mill hospital records. The authors would also like to thank the sugarcane workers participating in this research.
References
Footnotes
JG and EH contributed equally.
Contributors JG, IW, DHW and CW conceived the study and CW prepared the first protocol draft. The final protocol was produced with essential input from DHW, JG, IW and KJ. IW was responsible for all field work logistics and participated in data collection together with CW, SP, EAM and JG. UE and JA were responsible for laboratory analyses. CW and EH were responsible for data management and EH performed the statistical analyses. DHW was the principal investigator and supervised the project.
Funding This research was funded via the Adelante Initiative, a multistakeholder programme working to improve labour conditions in the sugarcane industry and beyond. Funding was provided by the German Investment Corporation (DEG) and German Ministry for Economic Development and Cooperation (BMZ) and the Ingenio San Antonio (ISA) sugar mill via the DEG and BMZ’s DeveloPPP.de Programme. Under the programme, the DEG and BMZ fund half of the programme and the loan recipient, ISA in this case, the other half. The half funded by DEG and BMZ is dedicated to the Adelante programme, the half funded by ISA is dedicated to a programme of direct aid for those already sick. The only exception is US$150 000 per year the mill puts towards the logistical costs associated with Adelante. They do not pay for the research, or researchers, and do not have any input on lines of inquiry or their reporting. Laboratory analyses were paid directly to Department of Clinical Chemistry, Skåne University Hospital in Lund, Sweden by ISA from the matching funds designated by the DeveloPPP.de programme. Due to the structure of the DeveloPPP.de programme, funds do have to pass through the sugar mill briefly (for about 24 hours) and are then passed to the non-governmental organisation, La Isla Network, to pay for the management and execution of the research. Gothenburg and Lund Universities also supported the work by inkind funding. Stavros Niarchos Foundation provided funds directly to La Isla Network for management and execution of the research ahead of and during harvest 1.
Competing interests UE and JA declare that their institution was paid directly by ISA for laboratory analyses from the matching funds designated by the DeveloPPP.de programme.
Patient consent for publication Not required.
Ethics approval This study was approved by the Comité de Ética para Investigaciones Biomédicas (CEIB), Facultad de Ciencias Médicas, Universidad Nacional Autónoma de Nicaragua (UNAN- León), FWA000045231/IRB00003342. The biochemical investigation carried out at the Division of Clinical Chemistry and Pharmacology at Lund University in Sweden was approved by the Regional Ethical Review Board in Lund (reg. no. 2018–256). Our trained staff apprised all workers of the study objectives and procedures and answered any questions before participants signed an informed consent after which they were interviewed by our staff and provided serum samples taken by ISA phlebotomists.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement No data are available.