Article Text

Abstract
Objectives Making decisions about disclosing a mental illness in the workplace is complicated. Decision aid tools are designed to help an individual make a specific choice. We developed a web-based decision aid to help inform decisions about disclosure for employees. This study aimed to examine the efficacy of this tool.
Method We conducted a randomised controlled trial with recruitment, randomisation and data collection all online. Participants had access to the intervention for 2 weeks. Assessments occurred at baseline, postintervention and 6 weeks’ follow-up. The primary outcome was decisional conflict. Secondary outcomes were stage and satisfaction of decision-making and mental health symptoms.
Results 107 adult employees were randomised to READY (n=53) or the control (n=54). The sample was predominantly female (83.2%). Participants using READY showed greater reduction in decisional conflict at postintervention (F(1,104)=16.8, p<0.001) (d=0.49, 95% CI 0.1 to 0.9) and follow-up (F(1,104)=23.6, p<0.001) (d=0.61, 95% CI 0.1 to 0.9). At postintervention the READY group were at a later stage of decision-making (F(1,104)=6.9, p=0.010) which was sustained, and showed a greater reduction in depressive symptoms (F(1,104)=6.5, p=0.013). Twenty-eight per cent of READY users disclosed, and reported a greater improvement in mental health than those who did not disclose.
Conclusions READY provides a confidential, flexible and effective tool to enhance employee’s decision-making about disclosure. Its use led to a comparative improvement in depressive symptoms compared with the current information provided by a leading mental health non-governmental organisation, without apparent harm. READY seems worth evaluating in other settings and, if these results are replicated, scaling for wider use.
Trial registration number ACTRN12618000229279.
- decision aid
- employee
- mental health condition
- disclosure
- workplace
Statistics from Altmetric.com
Key messages
What is already known about this subject?
Deciding whether or not to disclose a mental illness in the workplace is often complicated, with different considerations for each individual.
Often individuals need to disclose their mental illness to receive reasonable adjustments.
Decision aid tools are designed to help individuals make a specific and deliberate choice and are widely used to inform decisions about medical treatment options.
What are the new findings?
This trial demonstrated that READY, the first online disclosure decision aid tool for employees, reduced decisional conflict regarding disclosure of a mental illness compared with the provision of standard information about disclosure and its consequence.
Use of the program resulted in people being at a later stage of decision-making, being more satisfied with their decision and less depressed at follow-up, with no indication of psychological harm.
How might this impact on policy or clinical practice in the foreseeable future?
READY provides a confidential, flexible and effective online tool to enable employees to make an informed decision about which disclosure option is best for them.
The decision aid allows individuals to consider an active disclosure before an event occurs, allowing employees to take control of their decision-making.
Introduction
Deciding whether or not to disclose a mental illness in the workplace is often complicated, with individualised considerations.1 Within the workplace context, disclosure is defined as the process in which an employee informs their employer of their disability.2 Under many countries’ equalities legislation, individuals need to disclose to receive reasonable adjustments.3
Interpersonal factors such as discrimination and stigma can affect employee’s disclosure decision-making.4 Employers prefer potential employees make disclosures during recruitment5 despite consistent evidence showing that employees may be seen as less employable.6 As a result, employees fear discrimination,7 worry about being a burden on others, being seen as weak8 or not being hired or promoted.9 A recent Australian survey found that over half of those who had experienced discrimination report not being hired because of their mental illness,10 and a global survey showed that employees were reluctant to disclose out of fear of job loss.11 Employees who had disclosed reported limited knowledge of symptoms, stigma and discrimination, limited managerial support and perceived negative consequences were barriers to their disclosure.12
The literature on disclosing mental health conditions in the workplace has often focused on the outcomes or predictors,13 rather than the process. Whether to disclose at all, how much to disclose (partial or full) and whom to disclose to draw on three identified styles of selective, indiscriminant or broadcasting disclosure.14 The timing is important as concealment itself can be a major stressor,15 and sometimes, a forced decision may be precipitated by symptom severity or impairment.6 A recent study16 indicated that employees generally start from a position of non-disclosure, often only moving to a position of disclosure when symptoms are no longer concealable.
Decision aid tools are designed to help individuals make a specific and deliberate choice, and are widely used to facilitate decisions about medical treatment options. A systematic review showed that decision aids for people facing treatment or screening decisions produced less decisional conflict, higher knowledge, a more active role in decision-making and increased risk perception.17 In the mental health context, the Conceal or Reveal (CORAL) randomised controlled trial (RCT)18 showed a paper-based decision aid tool for people with a severe mental illness in secondary care services reduced disclosure decisional conflict when seeking employment and tangible employment benefits.
We developed a web-based decision aid tool (READY) to help facilitate disclosure decisions for individuals in current employment. This study aimed to examine the efficacy of READY in reducing decisional conflict, the primary outcome, compared with the online disclosure information provided by a leading mental health charity, at postintervention and 6 weeks’ follow-up. Secondary outcomes were the effect on the stage and satisfaction of decision-making and mental health.
Methods
Design
A parallel arm RCT was conducted. Participants had open access to READY or online disclosure information for 2 weeks. Assessments occurred at baseline, postintervention and 6 weeks postbaseline.
Recruitment, randomisation and data collection were all internet based.
Participants
The target population was employed adults, any gender, aged 18–65 years, with a self-identified mental health condition and who had not previously disclosed mental ill health to their current employer.
Participants were excluded if they did not have access to reliable internet, a valid email address or if they reported poor English fluency.
This study was registered in the Australian New Zealand Clinical Trials Registry (ANZCTR): ACTRN12618000229279.
Recruitment, informed consent and randomisation
Recruitment occurred between 8 November 2017 and 25 February 2018 through many channels: emails to people on a mental health research register, a pop-up in a mental health treatment app (HeadGear) and via Facebook advertisements. These invited people to visit the study website.
The website provided an online version of the participant information statement and consent form, which was available for download. After completing the informed consent process online, participants completed the baseline questionnaires (sociodemographic, outcome and moderator measures) on the study website before being randomised. Automatic computerised randomisation was triggered within the website when eligible participants completed the baseline assessment. The allocation was set at a 1:1 ratio, and the procedure allowed for full replication.
Intervention
The content of READY was developed in an iterative fashion based on currently available disclosure materials18 and guided by an international expert group. The content of READY was tested in focus groups with employees who had disclosed mental ill health in the workplace and key occupational decision makers12 to identify influencing factors. The wording of the tool scored a Flesch-Kincaid Grade Level of 6.6, which is understandable by the average 11 year-olds.19
The final program (READY) was based around seven self-guided modules which enabled the user to consider potential consequences of (non)-disclosure, weighing advantages and obstacles, their needs and values, timing and process of disclosing while reflecting on past disclosures and providing the user with an interactive summary of their responses. Each module was designed to take approximately 5–10 min to complete. The program was carefully worded to avoid promoting any specific decision as the ‘correct’ one. Users needed to complete each interactive module to be able to move to the next module. Multiple log-ins were available.
Control condition
The control group were given access to a visually similar website with four modules that contained information about disclosure rights and responsibilities, laws, and legislation based on content from the HeadsUp website, an Australian website aimed at workers with mental health conditions, hosted by the country’s largest mental health non-governmental organisation (NGO), Beyond Blue. This website has been publicly available since 2014, and a recent international review of guidelines that manage workplace mental health conditions highly rated the website for quality and comprehension,20 and it was awarded the Best Online Learning and Education Resource at the Digital Industry Association of Australia Awards 2014 with 146 000 unique views within the first year.21 Permission was obtained to use the content from the HeadsUp website. Users again had to complete each module to be able to move to the next.
Both conditions provided links to the relevant legislation: Disability and Discrimination Act 1992, and the Privacy Act 1988.
Program procedures
Following allocation, the program (READY or Control) was available to the participant for 2 weeks. If no log-in took place within 4 days of randomisation, an automated reminder email was sent, followed by a phone call 2 days later by the lead researcher. Participants received the postintervention questions when they finished their final module, or at 2 weeks after allocation. They completed the online follow-up questionnaires 4 weeks later. Participants who did not complete online follow-up and had provided contact details were called once by the lead researcher to complete these over the phone.
Measures
Sociodemographic measures
Participants self-reported demographic information: gender, age, relationship status and indigenous background.
Study-specific questions measured the participant’s workplace relationships such as, ‘Do you feel you have a good relationship with your boss’ with dichotomous ‘Yes or No’ answers. Workplace sector was assessed by asking participants to select from 15 options. Participants self-reported diagnosed mental health conditions with multiple options provided and a provision of a free text box. We classified schizophrenia and bipolar as ‘severe mental disorder’ and all others as ‘common mental disorder’.
Primary outcome measure
The primary outcome was change in decisional conflict postintervention. Decisional conflict was measured using the 10-item Decisional Conflict Scale Low Literacy version22 (α=0.86), measuring self-reported uncertainty, the level that they feel informed, clarity of values, whether they feel supported and effective decision-making. Participants responded: Yes=0, Unsure=2 and No=4 on a Likert scale to each question, the scores were summed and transformed into a 0–100 scale as per the user manual (no decisional conflict=0, extremely high decisional conflict=100).
Secondary outcome measures
Stage of decision-making (SDM) is a five-question scale to measure individual readiness to engage in decision-making.23 Participants selected their SDM from ‘I have not yet thought about the options’=0 to ‘I have already told my employer’=5.
Decisional dissatisfaction was measured with two items stating ‘Do you expect to stick with your decision?’ and ‘Are you satisfied with your decision?’ with responses ranging from Yes=0, Unsure=2 and No=4 on a Likert scale.
Stress was measured using the Perceived Stress Scale (PSS-10) (α=0.91).24 Total scores range from 0 to 40, those scoring over 20 were considered ‘highly stressed’.
Depressive symptoms were measured using the Patient Health Questionnaire (PHQ-9)25 (α=0.84) as a continuous variable, and ‘depression’ was defined using the standard cut point (≥11). The presence of suicidal ideation was assessed with question 9 (no vs any).
Potential moderators
Discrimination and stigma over the last 12 months were measured with the Discrimination and Stigma Scale-12,26 comprised 32 questions and rated on a 4-point Likert scale. An overall score was generated using a binary score for each item, with higher values indicating greater experience of stigma and discrimination.27
Bullying was measured with one question from the Negative Acts Questionnaire-Revised (α=0.90)28: ‘Have you been bullied at work?’ along with a definition, then coded into Yes=1, No=0.
Resilience was measured with the 6-item Brief Resilience Scale29 (α=0.86), assessing the ability to bounce back or recover from stress. Those scoring over 15 were considered to have low resilience.
Sample size
The sample size was based on the effect size in the CORAL study18 which had a between-group effect size of Hedge’s g=0.69 (95% CI 0.21 to 1.17, p=0.005) for mean difference in change in decisional conflict. A sample of 34 per arm would give 80% power to detect a smaller 0.4 effect size, allowing for a potential dropout rate of 33%,30 the target sample size was 46 participants per condition.
Statistical analysis
All data were analysed with SPSS V.24.0. Adequacy of randomisation was assessed by comparing the baseline characteristics of the intervention and control groups using t-tests for continuous variables and χ2 test for binary measures. Attrition was assessed comparing the postintervention characteristics of the dropouts and the completers to determine any apparent differences.
Primary analyses were undertaken on an intention-to-treat basis, including all eligible participants randomised. Last observation carried forward (LOCF) was used to handle the missing data, providing a conservative estimate of treatment effect if data are missing at random (MAR).
The main analysis of efficacy compared READY and the control on outcome measures at postintervention and follow-up using between-subjects analysis of covariance (ANCOVA) with baseline scores as covariates. Cohen’s d with 95% CIs was calculated by comparing the change in means of READY and the control at each time point. According to Cohen, d=0.2 can be considered small, d=0.5 a medium effect and d=0.8 a large effect.31
Univariate effects of the intervention and control and their interaction with baseline mental health and workplace factors were examined using between-subjects ANCOVAs adjusting for the relevant baseline variables (ie, discrimination).
Univariate effects of the program groups and the interaction of severe mental disorders and common mental disorders on primary and secondary outcome measures were examined using between-subjects analyses of variance.
Finally, the number of participants that disclosed (based on the SDM questionnaire) in each arm was reported along with any association with change in depression or stress scores at 6 weeks’ follow-up.
Results
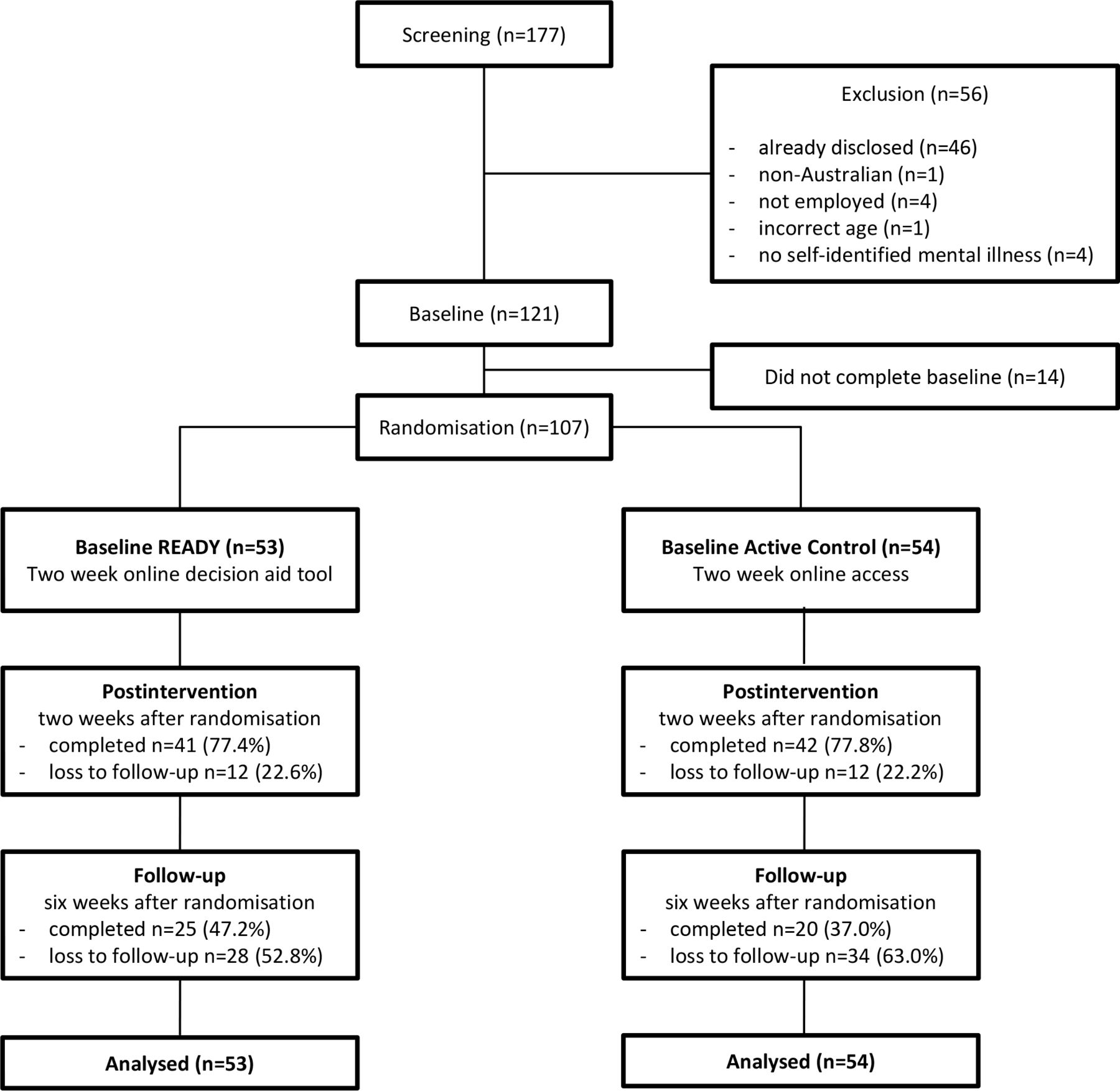
A total of 177 individuals completed online screening for eligibility. Of those, 56 (31.6%) were excluded, primarily because they had already disclosed their mental health condition in their workplace (n=46). A further 14 did not complete the baseline assessment, leaving 107 participants randomised. The study flow is illustrated in figure 1.

Consolidated Standards of Reporting Trials (CONSORT) flow of participants.
The average age of the participants was 34.3 (SD=12.1) years. The sample was predominately female (83.2%), not married (61.7%) and not of Aboriginal or Torres Strait Islander descent (97.2%). Many were employed in a social and community services industry (30.8%). The majority reported having a good relationship with their boss (71.0%) and colleagues (81.3%). One-quarter had experienced discrimination when at work (27.1%), and 72% anticipated discrimination at work. Almost half (41.1%) had experienced bullying. Most participants had low resilience (61.7%), were depressed (≥11 on PHQ-9) (71.0%) and highly stressed (>20 on PSS-10) (84.1%), and had a diagnosed common mental health disorder (74.8%) (table 1). There were no baseline differences between the intervention and active control arms (table 1).
Baseline characteristics overall and by intervention type
There were no differences between the intervention and control in decisional conflict, decisional dissatisfaction, SDM or stress scores at baseline although the intervention group had higher levels of depressive symptoms (table 2).
Change in decision, stress and depression measures throughout the trial (ITT sample n=107)
Overall, 24 (22.4%) of participants at postintervention, and 62 (57.9%) at follow-up did not provide outcome data, with no differential attrition between the control group (postintervention n=42, follow-up n=20) and READY (postintervention n=41, follow-up n=25). Twenty-six participants completed the outcome data over the phone, 15 from the intervention group, and 11 from the control group, the remaining participants completing the self-assessment online. There was no association of any of the baseline characteristics with the completeness of data, supporting the MAR assumption for the LOCF analysis.
Of the 53 who started the READY program, 49 (92.5%) attempted at least one module, and 25 (47.2%) completed all seven modules. On average participants in the intervention group completed 3.9 (SD=3.2) modules. Fifty-one (94.4%) of the control arm attempted at least one module, and 48 (88.9%) completed all of the four modules. On average, the control group completed 3.7 (SD=1.1) modules.
Primary outcome: decisional conflict
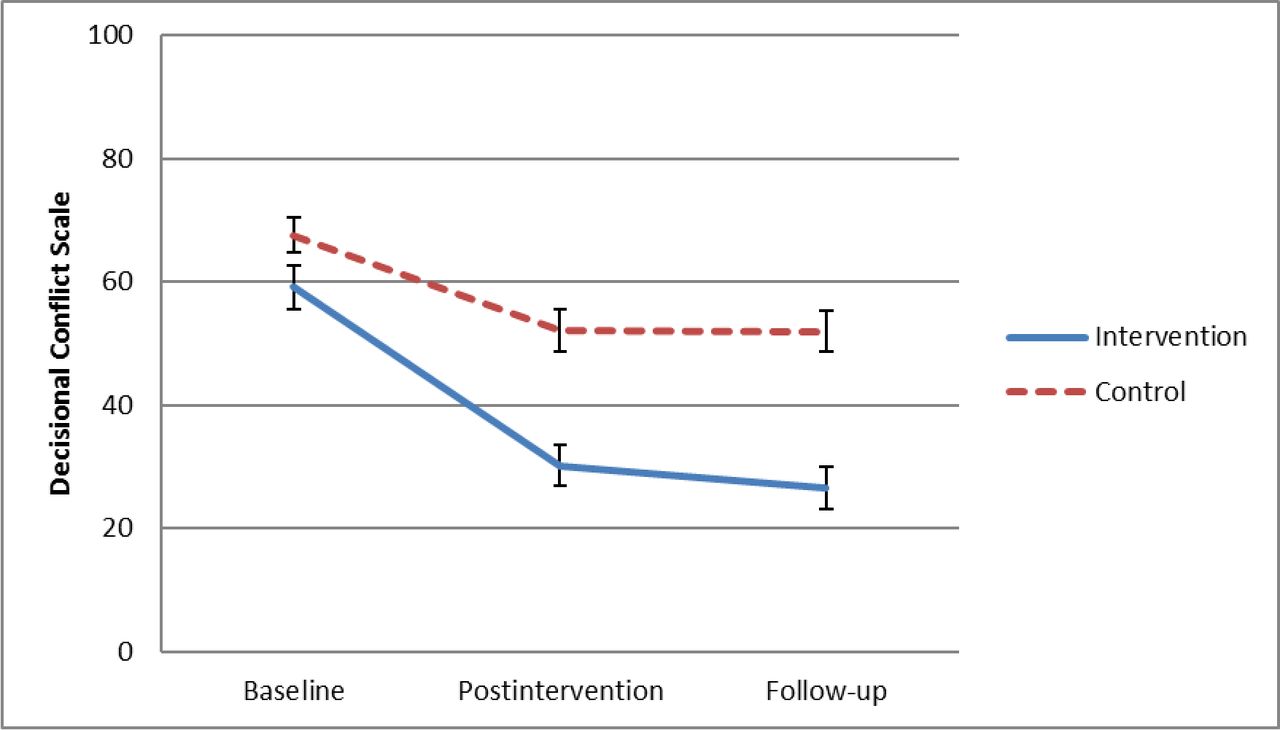
Participants in the READY arm showed greater reduction in decisional conflict at postintervention (F(1,104)=16.8, p<0.001), which was sustained at follow-up (F(1,104)=23.6, p<0.001) compared with the control arm. Moderate between-arm effect sizes were observed at postintervention (d=0.49, 95% CI 0.1 to 0.9) and at follow-up (d=0.61, 95% CI 0.2 to 1.0) (table 2 and figure 2).

{kind=link}
{kind=link}
Mean and SEs in decisional conflict over the course of the trial.
Secondary outcomes
At postintervention, the READY group were at a later SDM than the control group (F(1,104)=6.9, p=0.010) with a moderate effect size (d=0.42, 95% CI 0.3 to 0.8). This effect increased at follow-up (F(1,104)=23.6, p<0.001) with a large effect (d=0.81, 95% CI 0.4 to 1.2). Decisional dissatisfaction was also reduced in the intervention arm (relative to control) at follow-up (F(1,104)=7.5, p=0.008) with a large effect (d=0.78, 95% CI 0.4 to 1.2). Depression (PHQ-9) scores were reduced in the intervention arm compared with the control (F(1,104)=6.5, p=0.013) with a moderate effect (d=0.59, 95% CI 0.2 to 1.0) at follow-up, but not immediately postintervention. There was no effect on stress (table 2 and online online supplementary figure 1).
Supplemental material
There was greater decisional conflict at baseline in those who were highly stressed, those who had experienced bullying, had a bad relationship with their boss or a bad relationship with their colleagues, but this was not associated with depression, low resilience, anticipated or experienced discrimination at baseline. The comparative efficacy of READY was increased in those with low resilience (resilience × arm interaction) (F(3,103)=4.4, p=0.038).
There was no interaction between common or severe mental disorders and program arm efficacy on any outcome measures.
Impact of using READY
Of the completers who provided follow-up data (n=25 in intervention and n=20 in control, figure 1), 7 (28%) of the READY group disclosed their condition and none in the control arm. As disclosure was only seen in those who used READY the results below only consider the intervention group. Disclosure was associated with a greater reduction in both depression and stress than non-disclosure (table 3).
Change in depression and stress scores at follow-up in disclosed versus non-disclosed in those who used READY
Discussion
This trial demonstrated that READY, the first online decision aid tool for employees, significantly reduced decisional conflict regarding disclosure of a mental health condition compared with a provision of standard information and that this was sustained at follow-up. Use of the program resulted in people being at a later SDM, being more satisfied with their decision and less depressed at follow-up, indicating no psychological harm. These results are consistent with previous research on the effectiveness of providing decision aid tools for health-related decisions.32
The efficacy of READY was unaffected by whether participants had a common or severe mental disorder. This finding is interesting, given that those with severe mental illness often have additional factors to consider such as higher rates of unemployment, underemployment, poorer vocational outcomes and negative societal stereotypes,33 34 suggesting that disclosure decision-making options may be more difficult.
Although the tool was not developed to lead to one particular decision, be it disclosure or not, one-quarter of those using READY who completed follow-up measures decided to disclose, whereas none of those in the control arm did. Of those who disclosed, 86% reported satisfaction with this decision. While READY facilitated the disclosure decision, seemingly low rates of actual disclosure were reported. We have no idea of what the optimum disclosure rate is given all of the known barriers and we observed no disclosure in the control arm. This suggests that a decision aid tool may facilitate the decision, but cannot address all barriers to disclosure, such as workplace support or culture. The low rates may also have been due to the short follow-up period of 6 weeks. We might have seen a higher rate of disclosure if participants had adequate time to meet with their managers to disclose formally.
There was a significant reduction in depression and stress in those who disclosed compared with those who did not. Although only seen in a small sample, this suggests two possible inferences. First, deciding to disclose might reduce depression and stress symptoms in employees, and accords with a recent Australian survey that showed that receiving support when disclosing is more common than expected.35 Second, participants who recovered from their depression then decided to disclose. The latter may be less likely as the disclosure has been reported as more common when individuals are experiencing greater symptoms36 37 or when there is a need,16 and less common when they display fewer symptoms.38
The level of resilience influenced the impact of READY on decisional conflict, suggesting that those who have low resilience may benefit the most from a structured online decision aid tool.
Surprisingly, discrimination was not associated with higher decisional conflict scores at entry, nor did they induce differential decreases in decisional conflict, contradicting previous research from CORAL.18
Strengths and limitations
This study had several strengths. The online decision aid tool was cocreated with experts and end-users and compared with an active control. Being a completely online intervention, READY maximises confidentiality which was previously reported as a barrier to disclosure.12 The literacy requirements of the tool were set at an appropriate level as some disclosure information is legalistic and requires high levels of literacy. For instance, the information provided from the NGO’s website in the control arm had a reading age of 17.7 years, this may have enhanced the comparative efficacy of READY.39
This study had some limitations. Although attrition was low for an internet-delivered intervention,30 we used a conservative analytical method (LOCF) that likely underestimated any effects. Women and those working in social and community services were over-represented, potentially limiting generalisability of the results. However, it is not surprising as higher participation and interest from women is not uncommon when help-seeking for mental health conditions.40 Lastly, the lead researcher conducted reminder phone calls to participants, possibly affected blinding, although randomisation arm was not visible.
Implications and future directions
READY reduced decisional conflict and facilitated decision-making among employees. There was no indication that the tool led to harm. Future studies should evaluate the long-term effectiveness, and potential adaptation for culturally and linguistically diverse workplaces, in younger working adults and male-dominated workplaces.
References
Footnotes
Contributors ES, NG, CH and SBH contributed to the conception and design of the work. ES, IC and NG completed the analyses and interpretation of data and initial draft of this work. All authors revised the work critically, added to the interpretation of data and added important intellectual content and reviewed the final draft.
Funding This study was developed in partnership with Beyond Blue with donations from the Movember Foundation. ES, NG, SBH, RAC and IC all received funding from Beyond Blue and Movember Foundation via a grant to run this study.
Competing interests None declared.
Patient consent for publication Not required.
Ethics approval This study was approved by the University of Sydney Ethics Review Board: 2017/740.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement All data relevant to the study are included in the article or uploaded as supplementary information.