Article Text

Abstract
Objectives We conducted a large cohort study to investigate the association between work-related wrist movements and carpal tunnel syndrome (CTS).
Methods Electro-goniometric measurements of wrist movements were performed for 30 jobs (eg, office work, child care, laundry work and slaughterhouse work). We measured wrist angular velocity, mean power frequency (MPF) and range of motion (ROM). We established a cohort of Danish citizens born 1940–1979 who held one of these jobs from age 18–80 years, using Danish national registers with annual employment information from 1992 to 2014. We updated the cohort by calendar year with job-specific and sex-specific means of measured exposures. Dates of a first diagnosis or operation because of CTS were retrieved from the Danish National Patient Register. The risk of CTS by quintiles of preceding exposure levels was assessed by adjusted incidence rate ratios (IRRadj) using Poisson regression models.
Results We found a clear exposure–response association between wrist angular velocity and CTS with an IRRadj of 2.31 (95% CI 2.09 to 2.56) when exposed to the highest level compared with the lowest. MPF also showed an exposure–response pattern, although less clear, with an IRRadj of 1.83 (1.68 to 1.98) for the highest compared with the lowest exposure level. ROM showed no clear pattern. Exposure–response patterns were different for men and women.
Conclusions High levels of wrist movement were associated with an increased risk of CTS. Preventive strategies should be aimed at jobs with high levels of wrist movements such as cleaning, laundry work and slaughterhouse work.
- work-related carpal tunnel syndrome
- work-related disorders of the upper limb
- carpal tunnel syndrome
- wrist movement
- electro-goniometry
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
- work-related carpal tunnel syndrome
- work-related disorders of the upper limb
- carpal tunnel syndrome
- wrist movement
- electro-goniometry
Key messages
What is already known about this subject?
Previous studies have found an association between work-related repetitive work and carpal tunnel syndrome, but these studies have often been limited by a cross-sectional study design and self-reported outcome and exposure assessment.
What are the new findings?
This study found a clear exposure–response relationship between wrist angular velocity and the risk of carpal tunnel syndrome, identified through register-based diagnoses, in a large population-based cohort with exposures based on technical measurements within 30 different jobs.
How might this impact on policy or clinical practice in the foreseeable future?
The results of this study suggest that preventive strategies should be aimed at jobs with high levels of wrist movements such as cleaners, laundry workers and slaughterhouse workers.
Introduction
Carpal tunnel syndrome (CTS) has consistently been shown to be associated with work-related biomechanical factors. The specific pathogenesis is not clearly understood, but symptoms relate to compression of the median nerve at the wrist, and several studies have demonstrated an increased pressure in the carpal tunnel when performing hand straining tasks.1 Symptoms include pain and paraesthesia of the three radial fingers and the radial part of the fourth finger and may involve atrophy of the thenar muscles. In severe cases, the ability to perform manual work may be compromised.
CTS is the most common nerve entrapment disorder and a common cause of work absence and private earning losses.2 In a large Swedish general population-based study (25–74 years) based on both clinical and electrophysiological diagnosis of CTS, the overall prevalence was 2.1% (95% CI 1.3% to 3.0%) among men and 3.0% (2.1% to 3.9%) among women.3 Pregnancy, wrist fractures, hypothyroidism, rheumatoid arthritis, diabetes mellitus and obesity are known risk factors.4 5 The best documented work-related risk factors are repetition, force and hand–arm vibration.6 7
Self-reported exposure is widely used in studies on biomechanical risk factors in CTS increasing the risk of reporting bias compared with objectively assessed exposure.8 9 Several studies included job titles or job function to define exposure,10–12 but both are difficult to interpret in terms of specific risk factors. Some studies have used expert ratings and observation, either alone or in combination, and some have used video analyses or technical measurements.6 7 13–15 Cross-sectional designs dominate the studies investigating biomechanical risk factors in CTS, but longitudinal designs have also been used.6 7 16 17 Exposure–response relationships for force and repetition has been determined in studies using observed measures6 7; however, exposure–response relationships for force and repetition in men and women based on technically obtained exposure measures have not yet been determined. To our knowledge, no large prospective cohort studies based on technical measurements within several different jobs have been conducted.
The aim of this study was to investigate the associations between movements of the wrist and the risk of CTS in a large prospective study, using representative whole day electro-goniometrical measurements of wrist movements in 30 specific jobs to assess exposure in a national register-based cohort of persons who ever held any of these jobs.
Methods
Exposure measurements in specific jobs
Whole day measurements of movements and position of the wrist were performed within 33 different jobs, classified by their occupational title according to the Danish version of the International Standard Classification of Occupations (DISCO).18 The majority of jobs (n=23) was measured in Denmark (Copenhagen and Aarhus) as part of two previous studies of work-related musculoskeletal upper extremity disorders.19 20 Ten jobs were measured in earlier studies in Sweden and Norway and were part of an existing job exposure database at the Department of Occupational and Environmental Medicine, University of Lund, Sweden. The methods were the same for all measurements and were supervised by one of the authors (G-ÅH). For each job, a description of the work tasks performed during the measurements was recorded. Only healthy, right-handed individuals with no musculoskeletal complaints were measured.
The jobs were chosen to represent large exposure contrasts and jobs of both sexes. We aimed to obtain measurements of: 10 men in male-dominated jobs, 10 women in female-dominated jobs and 10 men and 10 women in jobs with a similar proportion of both men and women. House painters, cleaners and office workers had measurements performed as part of other studies and therefore had more measurements performed.15 21
Wrist measurements were performed using biaxial goniometers (SG75, Biometrics, LTD, Newport, UK), placed on the dorsal side of the right and left wrist with the proximal part in the midline between radius and ulna and the distal part over the third metacarpal bone, and data were recorded by person-worn data loggers (Logger Teknologi HB, Åkarp, Sweden) with a sampling frequency of 20 Hz for a full work day, excluding time for instruction, mounting and dismounting the equipment. The mean measuring time was 5.5 hours (3.1–6.9). Analyses were made bilaterally. For each person, the flexion/extension median angular velocity (°/s) and the mean power frequency (MPF) (Hz) was calculated as a measure of wrist movements. Furthermore, the 10th and 90th percentile of the wrist angular deviation from the neutral position was calculated and used the difference between these percentiles as a measure of range of motion (ROM) (°). For each job and sex, the means of these measures were calculated to represent the group and sex average angular velocity, MPF and ROM to create a job exposure matrix for subsequent use in epidemiological studies.
Study population
From the national Danish Civil Registration System,22 we established a cohort of persons born in Denmark between 1 January 1940 and 31 December 1979 including information on sex, date of birth, immigration, emigration and death. Each person was identified by their unique Danish personal identification number allowing linkage to personal information in other national registers in Statistics Denmark. We retrieved individual annual information from 1 January 1992 to 1 January 2015 on their main occupational title by DISCO codes, the industry where the person worked, coded by the Danish Industrial Classification of All Economic Activities,23 and the highest fulfilled educational level coded by the Danish version of the International Standard Classification of Education.24
We used this information on occupational title, industry and education to identify persons who had ever held a job corresponding to the previously established job matrix of 33 jobs with measurements. Since each DISCO code can refer to several job titles, industry and education codes were in some cases used to identify the specific job. The specific codes used for each job are listed in online supplementary appendix 1. We excluded three jobs (assembly worker, packing worker and wood parquet industry worker) that could not be defined with sufficient accuracy in the national registers, thus 30 jobs were finally included.
Supplemental material
We retrieved information on the proportion of time with salaried work in each calendar year, defining the job-specific exposure time for each calendar year in the 30 jobs. The annual proportions of working time were multiplied with the job-specific exposure for angular velocity, MPF and ROM, creating an annual measure of exposure level (duration*intensity) for that calendar year for each of the three exposures. We further calculated total cumulative exposures for each calendar year by adding the exposure of all previous years. We excluded persons without information on annual proportion of working time and persons who immigrated after 1 January 1992, if they were more than 18 years old at immigration (figure 1).

Flow chart illustrating the process of creating the cohort.
Outcome and health-related confounders
The Danish National Patient Register (DNPR) holds information about all patient contacts to all Danish hospitals since 1977.25 Cases were identified in DNPR by primary CTS diagnosis or CTS operation. Diagnoses were coded by the International Classification of Diseases (ICD) 8th (ICD-8) (1971–1993) and 10th (ICD-10)(1994–2014) revisions, respectively, and CTS operations were coded by a specific Danish classification (1977–1995) and the NOMESCO Classification of Surgical Procedures (NCSP) (1996–2014), respectively.26 We used ICD-8 code 357.99 and ICD-10 code G56.0 to identify CTS diagnoses, and the specific Danish classification code 3680 and NCSP codes KACC51 and KACC61 to identify CTS operations. Both diagnosis and operation codes were hospital discharge codes. Similar information was recorded for pregnancies, wrist-near fractures, hypothyroidism, rheumatoid arthritis, diabetes mellitus and obesity (see online supplementary appendix 2). Pregnancy was defined as 7 months prior to and 5 months after giving birth. Date of occurrence of hypothyroidism, rheumatoid arthritis, diabetes and obesity was set to 1 January the year of diagnosis and they were included as risk factors from that year and onwards.
Supplemental material
Analysis
The cohort was followed from the first calendar year the person entered one of the 30 jobs if they were at least ≥18 years of age until the date of first-time CTS, emigration, death or 1 January 2015, whichever came first. We excluded persons with a CTS diagnosis or CTS operation prior to start of follow-up (figure 1). Each person obtained risk time from 1 January the year after they entered the cohort until the end of follow-up time. Risk time was divided into age-specific risk time, based on the proportion of time before and after the date of birth using the Lexis-SAS macro.27 In case that a wrist-near fracture had occurred, the risk time was split into risk time before and after the date of fracture and was then included as a risk factor for the rest of follow-up. In case of pregnancy, risk time was similarly split by dates of start and end of pregnancy. Regarding all other health-related confounders, risk time was split 1 January the year of the diagnosis.
Poisson regression models were used to examine incidence rate ratios (IRRs) of CTS in relation to angular velocity, MPF and ROM separately.28 A logarithmic transformation of the risk time was used as offset value.
Our main analyses included the 1-year exposure from the previous calendar year (1-year lag) because of the potential risk of change in exposure due to symptoms preceding a CTS diagnosis. Exposure variables were examined by their quintile categories. Persons in jobs with unmeasured exposures in the relevant year were treated as a separate category. As sensitivity analyses, we examined the association with the total cumulative exposure with a 1-year lag to assess if the effect was different for recent exposure and longer lasting cumulative exposure. We also examined if the 1-year lag was sufficient to guard against effects of CTS on changes in exposure by using a 2-year lag instead. Furthermore, we examined if the results of the main analyses were different for CTS diagnoses with or without operation.
Results were reported as crude and adjusted IRRs. We adjusted for sex, age (18–29, 30–39, 40–49, 50–59, 60–69 and 70–80 years), calendar year (<2000, 2000–2004, 2005–2009 and 2010–2015), pregnancy, wrist-near fracture, hypothyroidism, rheumatoid arthritis, diabetes and obesity. To assess whether exposure effects were different for men and women, we included a multiplicative interaction term between sex and angular velocity, MPF and ROM in the main analyses and further stratified analyses by sex.
Furthermore, we made Poisson regression models including exposure as a natural cubic spline with four knots and the same confounders as in the main adjusted analyses. Exposure quintiles were used as knots.
Data were analysed using SAS statistical software V.9.4 (English), except for the splines, which were made using R Studio version 1.1.456.
Results
A total of 1 015 418 persons were included in the cohort, 43% men. Measured values of angular velocity ranged from 3.55°/s to 37.6°/s, MPF from 0.20 Hz to 0.45 Hz and ROM from 29.8° to 65.1° (table 1). Angular velocity and MPF were highly correlated (Spearman correlation coefficient (CC)=0.94). The correlations of ROM and angular velocity and MPF, respectively, were considerably lower (Spearman CC=0.29 and 0.21, respectively). We identified 6834 cases of CTS of which 1546 also had an operation code. Mean age at entry ranged from 18.8 years to 42.8 years between jobs (table 1).
Cohort characteristics on the 30 different jobs (eight with both sexes represented). Jobs are arranged according to angular wrist velocity. Number of persons (N) and age at entry are based on the total cohort. Total risk time and number of carpal tunnel syndrome cases are based on the dataset used in the analyses. Exposure intensities of wrist angular velocity, mean power frequency and range of motion are based on the electro-goniometric measurements
Sex varied considerably across exposure level, while age, wrist-near fractures, hypothyroidism, rheumatoid arthritis, diabetes mellitus and obesity seemed evenly distributed across levels of exposure to angular velocity (table 2).
Distribution of potential confounders by 1-year exposure levels (intensity*duration) shown for wrist angular velocity. Numbers (N) and point prevalences (%) at end of follow-up (2014)*
For angular velocity, the IRR and IRRadj increased monotonously from the second to the fifth exposure quintile with IRRadj 2.31 (2.09 to 2.56) for the highest, compared with the lowest levels (table 3). MPF also showed an increase in IRR with increasing exposure, but after adjustment, this pattern became somewhat irregular with a lower IRRadj in the fourth quintile than in the adjacent quintiles. The highest exposure group had IRRadj 1.83 (1.68 to 1.98). The analyses regarding ROM showed no clear pattern.
Number of persons with carpal tunnel syndrome (CTS) (diagnosis or surgery), incidence rate (IR), crude and adjusted incidence rate ratio (IRR) of CTS cases by 1-year exposure levels (intensity*duration) shown for wrist angular velocity, mean power frequency and range of motion
Sex differences
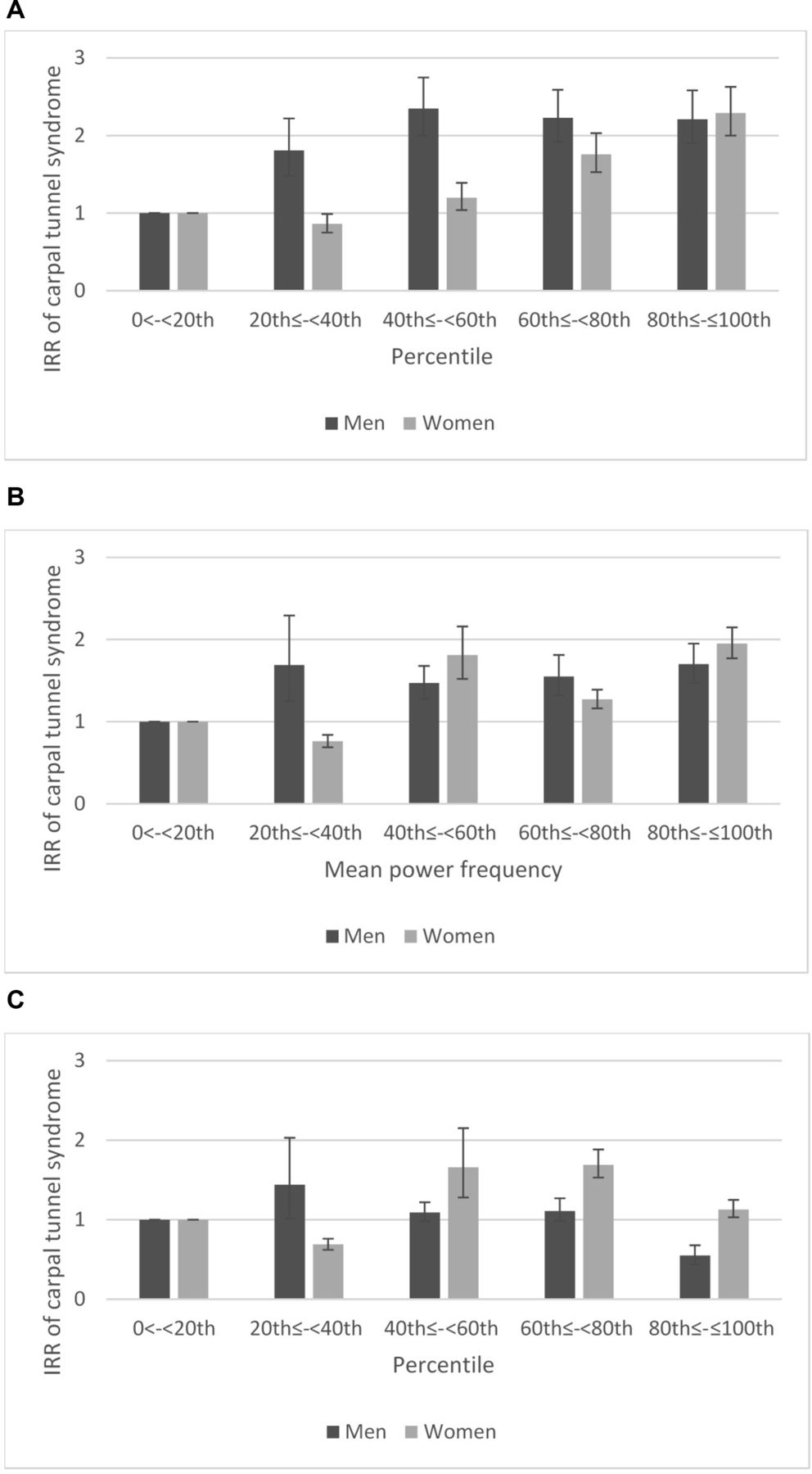
The incidence rate of CTS was 10.69 cases/10 000 person-years for men and 14.03 cases/10 000 person-years for women. For women, the risk of CTS increased with increasing angular velocity from the third to the fifth quintile (figure 2). For men, the risk of CTS increased more steeply than for women from the first to the third quintile and then became slightly smaller in the fourth and the fifth quintiles for both angular velocity and MPF. For women, the results for MPF were somewhat similar to the main analyses. For women, stratified analyses of ROM showed a steep increase from the second to the third quintile, levelling off in the fourth and decreasing a bit in the fifth quintile. We found no clear exposure–response pattern for men. The differences between men and women were significant for all three exposures (p<0.0001).

{kind=link}
{kind=link}
The association between angular velocity (A), mean power frequency (B) and range of motion (C) and carpal tunnel syndrome stratified by sex. Exposure ranges in percentiles as in table 3. Estimates are adjusted incidence rate ratios (IRRs), including marks reflecting the CIs. Adjustments are similar to adjustments described in table 3.
Sensitivity analyses
One-year exposure 2 years prior to outcome showed a pattern like the main analyses but with stronger IRRs reflecting an even clearer exposure–response pattern. Analyses of total cumulative exposure showed a pattern like the main analyses for angular velocity but with lower IRRs. The results showed no effect of MPF and ROM on CTS. The analyses including natural cubic splines also showed a similar pattern of the association between wrist velocity and CTS as the main analyses, as did analyses based on CTS operation alone (data not shown).
Discussion
We found a clear exposure–response association between angular velocity and CTS. The association between MPF and CTS was similar but with smaller risk estimates and a less consistent pattern, whereas ROM showed no clear association with CTS. Separate analyses for men and women showed different patterns for angular velocity and MPF. The increase in risk of CTS for women followed the same pattern as the main analyses, while for men, the increase in risk of CTS was initially steeper followed by a plateau. For ROM, analyses for men and women showed no clear pattern. The sensitivity analyses testing different time frames for exposure showed similar results for angular velocity, supporting that our main findings did not depend on the specific analysis. The results for MPF and ROM were more vulnerable to the choice of analysis. For all three exposures, analyses with 1-year exposure and 2-year lag resulted in higher IRRs.
Our findings correspond well with findings in other longitudinal studies. Dale et al 13 recently found a positive exposure–response association between repetition and force defined by both an expert-based job exposure matrix and by observation of hand activity level (HAL) and CTS. Gell et al investigated clerical workers and found an increased risk of CTS when peak force in combination with HAL was above a predefined limit which, however, was not statistically significant.29 Werner et al found video-observed radio/ulnar wrist deviation and elbow posture to be an ergonomic risk factor in CTS among auto assembly workers.30 The study did not find any association between flexion/extension, force, repetition or HAL on CTS risk.
Few have studied exposure assessed by technical measurements on the risk of CTS. Nordander et al 14 and Heilskov-Hansen et al 15 studied movements of the wrist using electro-goniometric measurements as risk factors of developing CTS. Nordander et al investigated a range of different work places and jobs in a cross-sectional design, whereas Heilskov-Hansen et al investigated house painters with a task-based approach in a longitudinal design. Both studies showed a positive association between wrist angular velocity and CTS. One study also found a positive association with MPF, but none of the studies found an association between position and CTS.15 No prior study has, to our knowledge, applied objective technical measurements to a large nationwide cohort with the use of a job exposure matrix. Cross-sectional studies using objective assessment of wrist exposures have also found positive associations between repetition and CTS and, contrary to our results, between position and CTS.31 The evidence is however still limited regarding position because of divergent results and large heterogeneity in the definition of position.16 32
We constructed the ROM variable based on the 90th and 10th interpercentile for flexion/extension. A true effect of ROM, if any, might be detected more easily using a larger inter-percentile range. The interpercentile range holds, however, no information about whether the position is primarily flexion, extension or both. If the potential association between position and CTS is correlated to either flexion or extension, it would be difficult to demonstrate in our setting. A study of Heilskov-Hansen et al 15 defined position as percentage of time with angles exceeding 45° flexion/extension or 20° radial/ulnar deviation and found no association between position and CTS. A study by Nordander et al 14 likewise found no association between wrist position and CTS. Unfortunately, we could not use absolute measures of flexion or extension because the reference value changed from functional zero in the older measurements to anatomical zero in the newer. We believe, however, that the ROMs used in this study, compared with, for instance, the absolute measures of time spent in flexed/extended positions used in the study by Heilskov-Hansen et al, are essentially expressing the same risk factor, non-neutral position.
Force is generally accepted as a risk factor in CTS, both alone and in combination with repetition and position.16 Force might explain some of the association between angular velocity and MPF and CTS, as some of the measured jobs are also traditionally seen as forceful. Unfortunately, we had no measure of force in this study; thus, it is unclear if this correlation can explain some of the observed association of CTS with velocity and MPF.
Women generally have a higher risk of CTS than men.3 33 Our analyses showed a multiplicative interaction between sex and exposure. The differences in exposure–response patterns may, however, partly reflect sex differences in the proportion of high-force jobs in the cohort. A large part of male jobs included forceful work tasks (eg, constructions workers and scaffolders), while most female jobs did not. In a recent study of house painters by Heilskov-Hansen et al,34 evidence of a multiplicative interaction between exposure and sex was not found.
This study did not include measures of acceleration. Previous studies using the same technical method have found a constant ratio between acceleration and velocity of around 10, but due to methodological challenges, velocity measures have been the preferred goniometric measure, although acceleration, as well as force, is clinically relevant risk factors in work-related MSDs.35 36
Our cohort consisted of persons born 1940–1979. Persons who turned 18 years before we could register their jobs in 1992 were included, which means that their work-related exposure before 1992 remains unknown. Analyses assessing total cumulative exposures therefore are at risk of truncation bias as persons without a full job history would be the oldest and therefore potentially a group exposed differently, most likely more, than the rest. However, mechanistic studies have shown that regarding CTS, the relevant exposures are the more recent,37 and since we identified the first outcomes in 1993 and only used updated exposure 1 year prior (with 1-year lag) in the main analysis, the influence of truncation bias is minimal in the main analyses.
Sensitivity analyses with 1-year exposure and 2-year lag generally resulted in higher IRRs and showed an even clearer exposure–response association between angular velocity and CTS. This could reflect a selection out of the most exposed jobs among symptomatic persons before being diagnosed. The sensitivity analyses including cumulated exposures have limitations, since risk time spent in one of the unmeasured jobs did not contribute to the exposure. This misclassification was independent of the outcome, and it therefore seems most likely that it will bias results of sensitivity analyses towards the null. This is in accordance with the less pronounced exposure–response relation for total cumulated exposure in comparison with the main results. The main analyses included only 1-year exposures and consequently misclassification was not a problem for these results.
The CTS diagnosis registered in DNPR is considered to be valid as the majority of patients admitted for assessment of CTS at the hospital have electroneuronography performed routinely to confirm the diagnosis.38 A certain part of CTS cases is diagnosed and conservatively treated by general practitioners, especially CTS during pregnancy. These CTS cases were not included in our data because of lack of valid coding in primary care, which explains the relatively low prevalences found in this study compared with other studies based on screening in general/working populations.6 39 40 CTS cases diagnosed in the healthcare system are most likely more severe than undiagnosed CTS cases in the population. Our results, therefore, may not be generalisable to all CTS cases. Furthermore, CTS cases with hand demanding work may experience more trouble than CTS cases with less hand demanding work and therefore become diagnosed earlier than CTS cases with less hand demanding work. If so, exposure–response associations could be inflated or spurious. The register-based design was further limited by a lack of information on handedness.
Conclusion
With the use of technical measurements and register-based outcome measures, this study found an increasing risk of CTS with increasing levels of wrist angular velocity. A similar association, although less clear, was found between repetition assessed by MPF and CTS. Exposure–response patterns differed for men and women perhaps reflecting different force exposure. No clear association was found for wrist position assessed by ROM, defined as the 90th and 10th interpercentile for flexion/extension, and CTS. Our results indicate that a reduction of repetitive and rapid movements may prevent the development of new CTS cases.
Acknowledgments
The authors would like to thank Thomas Heilskov-Hansen and coworkers at the Department of Occupational Medicine in Herning, especially Annett Dalbøge, who took part in performance of the measurements. Furthermore, we would like to thank coworkers at The University Hospital in Lund, especially research and associate professor engineer Henrik Enquist for assistance during management of data from the electro-goniometric measurements.
References
Footnotes
Contributors CBL, SM, LCT, G-ÅH and JFT planned the study. CBL, SM, LCT and JFT made the analyses. CBL drafted the manuscript. All authors critically reviewed and approved the manuscript.
Funding This study was supported by grants from the Danish Working Environment Research Fund (grant #43-2010-03).
Competing interests None declared.
Ethics approval The study protocol was accepted by the Danish Data Protection Agency (j.nr. 2013-41-2555). Approval from the Ethics Committee of the Capital Region of Denmark was not necessary according to Danish law.
Provenance and peer review Not commissioned; externally peer reviewed.
Patient consent for publication Not required.