Article Text

Abstract
Objectives This study aimed to examine whether high emotional demands at work predict long-term sickness absence (LTSA) in the Danish workforce and whether associations differ by perceived and content-related emotional demands.
Methods We included 26 410 individuals from the Work Environment and Health in Denmark Study, a nationwide sample of the Danish workforce. Emotional demands at work were measured with two items: one assessing perceived emotional demands (asking how often respondents were emotionally affected by work) and one assessing content-related emotional demands (frequency of contact with individuals in difficult situations). LTSA was register based and defined as spells of ≥6 weeks. Respondents with LTSA during 2 years before baseline were excluded. Follow-up was 52 weeks. Using Cox regression, we estimated risk of LTSA per one-unit increase in emotional demands rated on a five-point scale.
Results During 22 466 person-years, we identified 1002 LTSA cases. Both perceived (HR 1.20, 95% CI 1.12 to 1.28) and content-related emotional demands (HR 1.07, 95% CI 1.01 to 1.13) predicted risk of LTSA after adjustment for confounders. Further adjustment for baseline depressive symptoms substantially attenuated associations for perceived (HR 1.08, 95% CI 1.01 to 1.16) but not content-related emotional demands (HR 1.05, 95% CI 1.00 to 1.11). Individuals working in occupations with above-average values of both exposures had an increased risk of LTSA (HR 1.32, 95% CI 1.14 to 1.52) compared with individuals in all other job groups.
Conclusions Perceived and content-related emotional demands at work predicted LTSA, also after adjustment for baseline depressive symptoms, supporting the interpretation that high emotional demands may be hazardous to employee’s health.
- emotional demands
- perceived
- content-related
- workplace
- sickness absence
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Key messages
What is already known about this subject?
Whether high emotional demands at work are hazardous to employee’s health is debated.
Some studies found that emotional demands predicted long-term sickness absence (LTSA) and depression. Other studies raised concerns that these associations might have been affected by bias related to the measurement of emotional demands.
What are the new findings?
Both perceived and content-related emotional demands at work predicted a higher risk of LTSA.
Adjusting for the baseline psychological state of the individual attenuated the estimate for perceived emotional demands more than for content-related emotional demands, but estimates for both types of demands remained statistically significant.
How might this impact on policy or clinical practice in the foreseeable future?
The results support the interpretation that high emotional demands contributes to a higher risk of LTSA.
Workplaces may consider reducing emotional demands at work as a mean for ensuring or improving employee’s health.
Further research on work-related resources that may buffer the effect of emotional demands at work would provide insights on prevention possibilities.
Introduction
Emotional demands at work concern aspects of work that require sustained emotional effort of employees.1 Examples of emotionally demanding work tasks are dealing with sick or dying patients, taking care of clients’ emotional needs, responding to clients’ sorrows and worries, and handling aggressive customers and clients.1–5
Whether a high level of emotional demands at work is hazardous to employee’s health is debated. Whereas some studies found that emotional demands are associated with a higher risk of sickness absence, depressive symptoms and psychological distress,6–16 other studies raised concerns that the measurement of emotional demands may have biassed associations.2 17
Previously, emotional demands have primarily been measured as perceived emotional demands, for example, with items like ‘how often do you feel emotionally affected by work?’. This type of item may measure both characteristics of the work environment (ie, that work is emotionally demanding) and factors related to the emotional processing of the individual (ie, a psychological state of the individual). Thus, measuring emotional demands as perceived emotional demands mixes the exposure to emotional demands with the psychological state of the individual, and it remains unclear if subsequent outcomes are due to the exposure, the psychological state of the individual or both.
To address possible bias concerning the measurement of emotional demands, Vammen et al recently compared how perceived and content-related emotional demands were associated with risk of clinical depression.2 Unlike perceived emotional demands, items on content-related emotional demands do not to mix the environmental exposure and the individual’s psychological state but focus on the content of the job task, such as dealing with others’ grieves and worries. The study found that perceived emotional demands but not content-related emotional demands predicted risk of clinical depression, strengthening concerns about bias in studies examining perceived emotional demands. The study by Vammen et al was limited, although, by including only public sector employees, a relatively small study population of about 3000 participants and low statistical power with only 62 cases of depression at follow-up.
In this article, we investigate the association between different conceptualisations of emotional demands and risk of long-term sickness absence (LTSA) in a nationwide sample of the Danish workforce with more than 25 000 employees. We chose LTSA as the outcome because LTSA is a valid indicator of ill-health, predicting both disability and mortality.18–20
In addition to measuring perceived and content-related emotional demands by self-report, we also measured these two types of emotional demands by job title, by aggregating self-reported emotional demands to the job group level. Measuring occupational exposures on the job group level instead of the individual level reduces reporting bias, although it might simultaneously increase risk of non-differential misclassification.21
We examined the prospective association between perceived and content-related emotional demands, measured on the individual level and the job group level, and risk of LTSA during a 1-year follow-up. We further examined if adjustment for participants’ psychological state at baseline affected the strengths of the associations.
Methods
Study design and participants
We analysed the prospective association between emotional demands at work with risk of LTSA by linking information on emotional demands, assessed with survey data from the Work Environment and Health in Denmark Study (WEHD), to register information on LTSA and covariates retrieved from nationwide registers. Time of follow-up was 52 weeks.
WEHD is a biennial survey of the work environment and health in Denmark from 2012 to 2020. WEHD is based on a nationwide sample of Danish employees aged 18 to 64 years. For this study, we combined data from the 2014 and 2016 waves as these two waves included identical items for measuring emotional demands, whereas the wording in the 2012 wave was slightly different.
Figure 1 shows the flow chart towards the final study sample. In total, 67 844 individuals were invited in the 2014 and 2016 waves of WEHD. Of these, 33 544 responded to the questionnaire (49.4%). We excluded 2020 respondents who were not working, 3540 with a history of LTSA or due to censoring (early retirement, statutory retirement pension and emigration) during 2 years before baseline, and finally, 1574 with missing information on exposures (n=689) or potential confounders (register-based covariates: n=318; depressive symptoms: n=567), yielding a sample of 26 410 participants. This sample was used for all analyses in this study.

Flow chart towards the final study sample. LTSA, long-term sickness absence; MDI, Major Depression Inventory.
Measurement of emotional demands
We measured emotional demands at work with two items: one item on perceived emotional demands and one item on content-related emotional demands. Perceived emotional demands were measured with the question: ‘How often are you emotionally affected by your work?’. Content-related emotional demands was measured with the question: ‘How often at work are you in contact with individuals in difficult situations (individuals who for example, are affected by serious disease, accident, grief, crisis, or social problems)?’. Both items were rated on a five-point scale (1: Never; 2: Seldom; 3: Sometimes; 4: Often; 5: Always).
We calculated a mean score of the two items (Cronbach’s Alpha=0.56), resulting in a score from 1 to 5, and we also used the two items as single measures. Further, we analysed the two single items as categorical variables. For this analysis, we collapsed the response categories ‘Never’ and ‘Seldom’ because of the low number of respondents in the category ‘Never’.
Measurement of LTSA
We identified LTSA in the Danish Register for Evaluation of Marginalisation (DREAM)22 that includes weekly information on all social transfer payments in Denmark since 1991. Since 2012, sickness absence spells of 31 consecutive days or more are registered in DREAM. Sickness absence spells that lasts for 30 days or less are payed for and managed by the employer. Sickness absence spells≥31 days are partly reimbursed by the municipalities that manage the course of these longer sickness absence spells. Accordingly, we defined LTSA as ≥31 consecutive days, corresponding to ≥6 weeks in the DREAM register. For each participant, we measured the first episode of LTSA after the date of questionnaire completion and followed each individual for up to 52 weeks.
Measurement of covariates
As potential confounders we included age, sex, education, cohabitation, children living at home. We further adjusted for depressive symptoms at baseline as a measure of individuals’ psychological state when responding to the questionnaire. All covariates have been associated with both emotional demands and LTSA in previous Danish studies,7 23 24 and were therefore considered potential confounders. Information on these potential confounders was retrieved from Danish population-based registers,25–28 except for depressive symptoms that were measured in WEHD.
Education was measured as the highest achieved education and categorised into four groups using the International Standard Classification of Education (ISCED)29: primary and lower secondary (ISCED level 0–2); upper and post secondary (ISCED level 3–4); first stage tertiary (ISCED level 5); and second stage tertiary education (ISCED level 6). Cohabitation was measured as married/cohabiting yes versus no. Children living at home were categorised into three groups: no children; at least one child aged 0–7 years; at least one child aged 8–17 years (and no children younger than 8 years). Depressive symptoms were measured with the Major Depression Inventory (MDI)30 in the 2014 and 2016 waves of WEHD. The MDI consists of 10 items assessing the level of depressive symptoms during the last 2 weeks. Each item was measured on a scale ranging from 0 (the symptom has not been present at all) to 5 (the symptom has been present all of the time). The items were summed to an MDI score (0–50), with higher scores indicating higher levels of depressive symptoms and included in the analyses as a continuous measure.
Statistical analysis
We analysed the association between emotional demands and subsequent LTSA by calculating HR and 95% CI using Cox proportional hazards regression models. We followed each individual for up to 52 weeks from the date of completing the questionnaire until first episode of LTSA or censoring due to early retirement, disability retirement, statutory retirement pension, maternity leave, emigration, death or end of study, whichever came first. Information on reasons of censoring was retrieved from DREAM.22
First, we analysed the emotional demands mean score as a predictor for LTSA. Second, we analysed the separate scores for perceived and content-related emotional demands. Third, we analysed perceived and content-related emotional demands as categorical predictor variables.
We calculated unadjusted estimates and estimates adjusted for age, sex, education, cohabitation and children living at home (model 1), and further adjusted for baseline depressive symptoms (model 2).
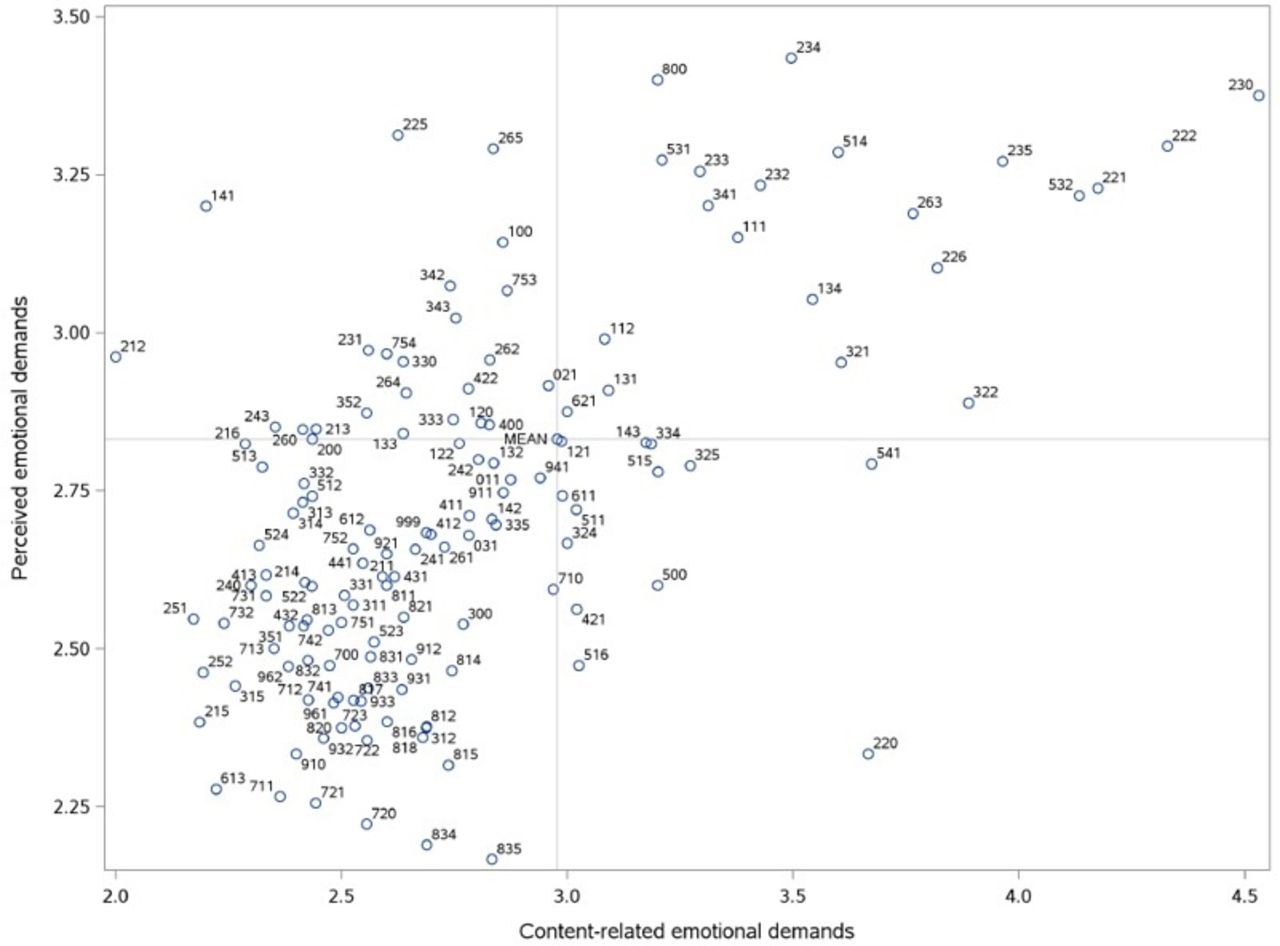
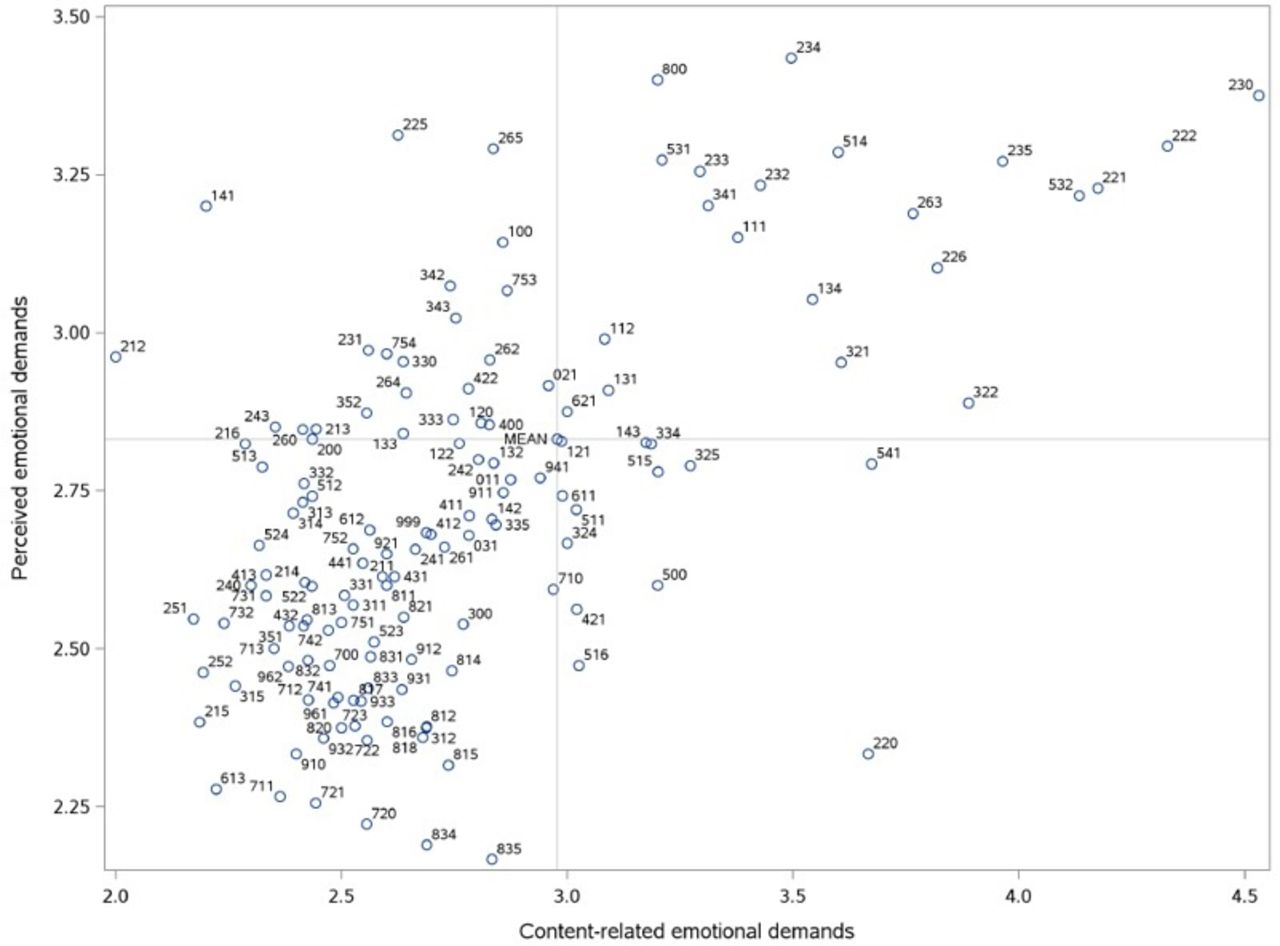
Finally, we aggregated perceived and content-related emotional demands to the job group level by calculating the mean scores for each of the two items by job group defined by the three-digit level of DISCO-08, the Danish version of the International Standard Classification of Occupations’ (ISCO)-08 system. Next, we assigned these mean scores to all individuals of the same job group. We plotted the job group mean scores of perceived and content-related emotional demands against each other to visually display where each job group was located with regard to perceived and content-related emotional demands. Using the scatter plot, we identified job groups scoring above the mean on both perceived and content-related emotional demands and calculated the risk of LTSA among individuals in these job groups compared with individuals in all other job groups in the study population.
All analyses were conducted using SAS statistical software V.9.4.
Results
Characteristics of the study population
Table 1 shows baseline characteristics of the study population. About half of the study population was women (52.7%) and the mean age was 45.3 years (SD=11.4). Most participants had upper and post secondary education as their highest completed education (42.6%), were cohabiting (77.7%) and had no children living at home (55.6%). The mean MDI score was 8.1 (SD=7.4). About a quarter responded ‘often’ or ‘always’ to the item on perceived emotional demands (23.9%), and about a third of the study population responded ‘often’ or ‘always’ to the item on content-related emotional demands (34.4%).
Baseline characteristics of the study population
Individual-level emotional demands at work and subsequent risk of LTSA
During 22 466 person-years, we identified 1002 cases of LTSA (45 per 1000 person-years). Among participants experiencing an LTSA event during follow-up, the mean time from baseline to event was 24 weeks.
Table 2 shows the unadjusted and adjusted estimates and 95% CI of the prospective association between emotional demands at work at baseline and risk of LTSA. In the unadjusted model, a one-unit increase in the emotional demands score predicted risk of LTSA with an HR of 1.27 (95% CI 1.19 to 1.36). The estimate attenuated after adjustment for age, sex, education, cohabitation and children living at home (HR 1.18, 95% CI 1.10 to 1.27, model 1) and further adjustment for depressive symptoms (HR 1.10, 95% CI 1.02 to 1.18, model 2) but remained statistically significant.
Associations of emotional demands at work at baseline with risk of long-term sickness absence during 52 weeks of follow-up
When we analysed the scores for perceived and content-related emotional demands separately, we found that both scores predicted risk of LTSA after adjustment for age, sex, education, cohabitation and children living at home, with perceived emotional demands showing stronger associations (HR 1.20, 95% CI 1.12 to 1.28) than content-related emotional demands (HR 1.07, 95% CI 1.01 to 1.13). After further adjustment for depressive symptoms, the estimate for perceived emotional demands attenuated substantially (HR 1.08, 95% CI 1.01 to 1.16), whereas the estimate for content-related emotional demands changed only marginally (HR 1.05, 95% CI 1.00 to 1.11).
In supplementary analyses, we repeated models 1 and 2 for the emotional demands score without excluding individuals with LTSA during the 2 years before baseline from the study population, but while adjusting for LTSA during the 2 years before baseline in both models. Results were similar to the results of the main analysis (results not shown).
Content-related and perceived emotional demands by job group and risk of LTSA
Figure 2 shows a scatter plot of the mean scores of the two emotional demands items by job group according to the three-digit level of DISCO-08 occupational classification system. There was a positive correlation (r2=0.35) between perceived emotional demands and content-related emotional demands. Job groups that scored above the mean on both measures of emotional demands were, for example, primary school and early childhood teachers (234), other teaching professionals (235), medical doctors (221), nursing and midwifery professionals (222), and personal care workers in health services (532) (see online supplementary appendix 1 for the scores for each job group).
Supplemental material
{kind=link}
{kind=link}
Job group mean scores of perceived and content-related emotional demands at work items by job group according to the three-digit level of DISCO-08 occupational classification system.
Table 3 shows the results from the analysis of risk of LTSA among individuals working in job groups that scored above the mean on both perceived and content-related emotional demands compared with individuals working in all other job groups. The HR was 1.32 (95% CI 1.14 to 1.52) in the most adjusted model.
Risk of long-term sickness absence among individuals working in job groups characterised by both high perceived and high content-related emotional demands at work compared with individuals working in all other job groups
Discussion
This study of a nationwide sample of 26 410 employees in Denmark showed that emotional demands, measured with a global score, a perceived emotional demands score and a content-related emotional demands score, predicted a higher risk of LTSA during a 1-year follow-up in the most-adjusted model that included adjustment for the psychological state of the individual at baseline. The adjustment for the psychological state attenuated the estimate for perceived emotional demands more than for content-related emotional demands.
Further analyses showed that individuals working in job groups that scored above the mean on both perceived and content-related emotional demands compared with individuals working in all other job groups had a higher risk of LTSA and that the estimate did not change after adjustment for the psychological state of the individual.
This study contributes with new insight into the potential effects of high emotional demands for employees’ risk of LTSA by using separate measures of perceived and content-related emotional demands in a nationwide cohort, by adjusting for the baseline psychological state of the individual and by aggregating data to the job group level to circumvent reporting bias. A previous study by Vammen et al 2 concluded that perceived emotional demands, but not the less reporting bias prone measure content-related emotional demands, were a risk factor for clinical depression. Therefore, the authors suggested that associations found in previous studies and in their own study may be explained by the individuals’ perception and not by the actual content of emotionally demanding work tasks. Consequently, the findings by Vammen et al did not support a causal effect of emotional demands at work and employee’s health. The present study, however, suggests that both perceived and content-related emotional demands are a risk factor for LTSA, a strong predictor of morbidity and mortality. Further, our findings suggest that the association between emotional demands and ill-health can only partly, but not completely, be attributable to the psychological state of the individual at the time when individuals are reporting their emotional demands exposure. This interpretation is further supported by the results from the analyses showing that job group level averaged exposure to the combination of both types of emotional demands predicted individual-level risk of LTSA.
Results from observational studies suggest that good leadership did not substantially buffer the negative effects of emotional demands at work on employee’s health,31 that work-related goal attainment moderated the negative effect of effort in emotion work on employee well-being32 and that experiencing one’s work as emotionally enriching and meaningful reduced the effect of emotional demands on exhaustion.33
Strengths and limitations
The strengths of this study include the large cohort consisting of 26 410 individuals in a nationwide sample of the Danish workforce in the age group 18–64 years and the use of outcome and covariate measurements from Danish population-based registers. As participants were followed-up in registers, attrition during follow-up was minimal. A further strength is that we addressed possible reporting bias by adjusting for baseline depressive symptoms as a proxy measure for participants’ psychological state and by aggregating the individual-level exposures to the job group level in additional analyses.
Some limitations need to be mentioned. First, we only had two single item measures available for emotional demands. By measuring our two exposure variables with only one item each, we likely have measured limited aspects of perceived and content-related emotional demands. The content-related item focused on frequency of contact with individuals in difficult situations, where difficult situations were elaborated with examples like being in contact with individuals who, for example, are affected by serious disease, accident, grief, crisis or social problems. These are rather serious situations and it is possible that we did not capture less serious forms of content-related emotional demands, such as having to care for emotional needs of others (eg, nursing home residents), helping others solving conflicts (eg, younger pupils in primary school) or handling rude customers (eg, in supermarkets). Our study would have benefitted from including more items to study different aspects of the concept of content-related emotional demands. Second, while attrition during follow-up was minimal due to register-based follow-up with full coverage, the baseline response rate of about 50% raises concerns about selective responding. Analyses of Danish national work environment surveys have shown that response rates tend to be lower among men, individuals of younger age and individuals of lower education,34 35 and we adjusted for these key sociodemographic variables in our analyses. Further, it is possible that risk of sickness absence was different for baseline responders and non-responders; however, we could not examine this, as we did not have information on sickness absence rates of non-responders. Third, it is possible that some unmeasured psychological characteristics may have been related to selection into occupations with high emotional demands and higher risk of sickness absence and therefore may have biassed our results.11 Excluding individuals with LTSA during the 2 years before baseline and adjusting for baseline depressive symptoms may partly, but not completely, have accounted for this bias. Fourth, the administrative registers in Denmark that we can use for research purposes do not include information on the cause of LTSA. Therefore, we do not know whether the 1002 LTSA episodes in this study were due to mental disorders, somatic diseases or injuries. Fifth, although long-term sickness absence is closely related to both morbidity and mortality and, thus, can be regarded as an indicator of ill-health,18–20 incident sickness absence is likely not exclusively determined by ill-health, but probably also by other factors, such as sickness absence legislations and practices, financial aspects or general attitudes at workplaces towards sickness absence.36 Future research may investigate whether these factors might confound or moderate the association between emotional demands at work and risk of LTSA. Finally, a sixth limitation is related to generalisability. As we conducted our study in a large sample of employed Danish residents from a wide range of job groups, we consider our results as generalisable to the Danish workforce. However, our results may not be generalisable to workforces in other countries, as national sickness absence legislations could influence the associations between working conditions and LTSA. Further studies on emotional demands at work and LTSA in other countries, particularly other than Nordic countries, are encouraged.
Conclusion
Perceived, content-related and job group aggregated levels of emotional demands at work all predicted risk of LTSA. Adjustment for the baseline psychological state of the individual measured by depressive symptoms affected the estimate for perceived emotional demands more than the estimate for content-related emotional demands but associations remained statistically significant in all analyses. This study therefore supports the notion that high emotional demands at work are a risk factor of LTSA. As LTSA is a valid indicator of ill-health, we conclude that high emotional demands at work may be hazardous to employee’s health.
References
Footnotes
Correction notice This article has been corrected since it published Online First.
Contributors EF, JKS, IEHM and RR contributed to the conception of the study, and all authors contributed to the interpretation of data. JKS and EF conducted the data analysis. EF drafted the manuscript, and all authors critically revised it and approved the final version.
Funding This study was funded by the Danish Work Environment Research Fund (grant numbers 27-2017-03 and 10-2016-02).
Competing interests None declared.
Patient consent for publication Not required.
Ethics approval The National Committee on Health Research Ethics. The study was approved by The Danish Data Protection Agency through the joint notification of the National Research Centre for the Working Environment (no. 2015-57-0074). All data are stored in a protected server environment hosted by Statistics Denmark.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement Data may be obtained from a third party and are not publicly available.