Article Text

Abstract
Objectives Previously published studies on parental occupational exposure to extremely low-frequency magnetic fields (ELF-MF) and risk of acute lymphoblastic leukaemia (ALL) and acute myeloid leukaemia (AML) in their offspring were inconsistent. We therefore evaluated this question within the Childhood Leukemia International Consortium.
Methods We pooled 11 case–control studies including 9723 childhood leukaemia cases and 17 099 controls. Parental occupational ELF-MF exposure was estimated by linking jobs to an ELF-MF job-exposure matrix (JEM). Logistic regression models were used to estimate ORs and 95% CIs in pooled analyses and meta-analyses.
Results ORs from pooled analyses for paternal ELF-MF exposure >0.2 microtesla (µT) at conception were 1.04 (95% CI 0.95 to 1.13) for ALL and 1.06 (95% CI 0.87 to 1.29) for AML, compared with ≤0.2 µT. Corresponding ORs for maternal ELF-MF exposure during pregnancy were 1.00 (95% CI 0.89 to 1.12) for ALL and 0.85 (95% CI 0.61 to 1.16) for AML. No trends of increasing ORs with increasing exposure level were evident. Furthermore, no associations were observed in the meta-analyses.
Conclusions In this large international dataset applying a comprehensive quantitative JEM, we did not find any associations between parental occupational ELF-MF exposure and childhood leukaemia.
- acute lymphoblastic leukemia
- acute myeloid leukemia
- case-control study
- elf-mf
- occupation
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Key messages
What is already known about this subject?
Some previous studies suggested an association between parental occupational exposure to extremely low-frequency magnetic fields (ELF-MF) and leukaemia in their offspring; however, the evidence is inconsistent.
What are the new findings?
We evaluated this research question in the largest case–control study consortium on childhood leukaemia and did not find association with parental occupational ELF-MF exposure.
How might this impact on policy or clinical practice in the foreseeable future?
These findings increase our understanding of childhood leukaemia aetiology.
Background
Leukaemia is the most common cancer in children diagnosed before 15 years of age worldwide, with acute lymphoblastic leukaemia (ALL) as most common (~75%) and acute myeloid leukaemia (AML) as second most common subtype (~15%).1 2
In addition to some well-established risk factors of childhood leukaemia (ie, a few hereditary conditions, exposure to high-dose ionising radiation and prior chemotherapy), many studies worldwide have suggested several possible factors associated with increased (or decreased) risk of the disease such as birth characteristics, immune-related markers and environmental pollutants.3–7
Early age at diagnosis indicates that childhood cancer might originate in utero and that exposures prior to birth including parental occupational exposures and early-life environmental exposures may be important determinants.8 9
Plausible underlying mechanisms for associations between parental exposures and childhood leukaemia are dependent on the time of exposure and which parent is exposed. Preconception exposures of parents are assumed to affect parental germ cells, while maternal exposures during pregnancy may affect the fetal development.10
Associations between residential extremely low-frequency magnetic field (ELF-MF) exposures and childhood leukaemia were observed in a pooled analysis of studies conducted before 200011 12 and confirmed in a pooled analysis of more recent studies.13 Risk assessments by the International Agency for Research on Cancer,14 the WHO15 and the European Commission’s Scientific Committee on Emerging and Newly Identified Health Risks came to similar conclusions16 that ELF-MF are possibly carcinogenic.
Some studies also reported associations with parental occupational ELF-MF exposure.17–20 However, these findings were not consistent with findings from other studies.21–23 Hug et al 22 included a meta-analysis in their report finding a summary relative risk estimate of 1.35 (95% CI 0.95 to 1.91) for paternal occupational exposure and also some evidence of publication bias, endorsing the need of further studies.
The Childhood Leukemia International Consortium (CLIC) is composed of case–control studies providing an opportunity to study even rare risk factors in relation to childhood leukaemia.24 Building on the wealth of data and biospecimens collected in over 20 case–control studies worldwide, CLIC was established in 2007, to overcome the limitations of single epidemiological studies.24
In this study, we aimed to assess the association of parental occupational exposure to ELF-MF with the risk of leukaemia in their offspring. We hypothesise that paternal occupational ELF-MF exposures occurring around conception and maternal ELF-MF exposures during pregnancy may be associated with leukaemia risk in the offspring.
Methods
Study population
A total of 11 case–control studies from eight countries in Europe, the USA and New Zealand contributed to the pooled analysis of ALL, and 10 studies contributed to the analyses of AML (table 1).
Characteristics of studies included in the CLIC pooled analysis of parental exposure to occupational low-frequency magnetic fields (EMF-MF) and risk of childhood leukaemia
In total, our study population included 9723 childhood leukaemia cases and 17 099 controls. Overall leukaemia cases consisted of ALL (B-lineage, T-lineage and other), AML and other types of leukaemia. We excluded 171 (1.8%) cases and 6 (<0.01%) controls with Down syndrome, a condition known to be a risk factor for the development of childhood leukaemia.
Cases were diagnosed between 1989 and 2011 and were identified from national or regional population-based cancer registries, networks of hospitals, selected hospitals or clinical trials.24 Control subjects were recruited from population registries, same hospitals as cases or by using random digit dialling. Cases and controls were less than 15 years of age at date of diagnosis (or equivalent date for controls) (table 1).
Data collection
Information on parental occupation and characteristics of the children was collected using standardised questionnaires, with in-person or telephone interviews of both parents in 10 of the contributing studies. In the register-based study from Finland, occupational data were obtained from census records in 1990, 1995, 2000, 2005 and 2010, and other characteristics from various nationwide population-based registries. Details of data collection in Finland are reported elsewhere.25
Characteristics of interest included the child’s sex, age, birth weight, birth order, ethnicity, as well as parental age at child’s birth, parental education and occupation. We categorised continuous covariates or recoded categorical ones according to standard categorizations previously used across CLIC studies.6 26
Parental occupations were coded using the International Standard Classification of Occupations (ISCO) from 1968, 1988 and 2008 in Finland, 1968 and 1988 in France and Greece and 1968 in Italy. In other countries, national job classifications were used (table 1); see below how those data were harmonised for the present pooling effort.
Exposure assessment
We defined time periods of interest as at conception for the father and during pregnancy for the mother. Parental occupational ELF-MF exposure was estimated by linking job titles to an existing quantitative ELF-MF job-exposure matrix (ELF-MF JEM). We used an ELF-MF JEM developed for the INTEROCC study,27 which is a multinational case–control study of adult brain tumours and occupational risk factors. The INTEROCC JEM originally developed by Bowman et al 28 was substantially enhanced by adding measurement data on jobs included in the INTEROCC study based on summary statistics or primary data from published occupational ELF-MF measurement studies in Canada, England, Finland, Italy, the Netherlands, New Zealand, Sweden and the USA.27 Further details of the ELF-MF JEM can be found elsewhere.27
The INTEROCC JEM was considered applicable to the CLIC dataset for three reasons. First, this JEM is based on data from countries that greatly overlap with the countries from which the CLIC data originates. Second, ELF-MF measurements used for its construction stem from time periods sufficiently relevant for the time periods covering the birth periods of the children in our CLIC dataset. Third, the JEM is based on an international occupational classification system (ISCO-68 and ISCO-88) allowing linkage with the occupational histories which were collected in CLIC.
Occupations in the ELF-MF JEM were coded according to the ISCO-88 unless exposure estimate was available for a more specific job in ISCO-68. Selected occupations with their respective ELF-MF exposure are shown in online supplementary table 1.
Supplemental material
We linked the ELF-MF JEM directly to datasets with occupations coded into ISCO-88 (table 1). In datasets with ISCO-68 codes, we translated ISCO-68 codes to ISCO-88 except for those codes that could be directly linked to the ELF-MF JEM. In the remaining datasets, job codes were translated to ISCO-88 by using correspondence tables (table 1). Some national job codes did not match to a single ISCO-88 code, which resulted in ‘one-to-many’ and ‘many-to-one’ translations and consequently multiple ELF-MF exposure assignments to the same persons. For such persons, we derived median and maximum ELF-MF exposure as a summary exposure estimate. The former was used in the main analyses and the latter in a sensitivity analyses.
Statistical analyses
Two analytical approaches were used. First, we pooled the primary data from CLIC case–control studies and estimated summary ORs and 95% CIs using unconditional logistic regression models. We estimated ORs for parental ELF-MF exposure for ALL and its subtypes (B-lineage and T-lineage ALL) as well as for AML. Specific characteristics of the child and the parents were considered as potential confounders based on the associations between the available characteristics described in the literature. They were retained in the final models if they changed OR estimates for parental ELF-MF exposure by more than 5%. As a result, in the final models, we included the child’s age and sex, highest level of education of either parent, case accrual time and primary study. Because birth weight, birth order and parental age did not change OR estimates by more than 5%, we did not retain them in the final models.
Second, we estimated ORs and 95% CIs for parental ELF-MF exposure in each individual study. In addition to adjustment variables used in the pooled analysis, we also controlled for study-specific adjustment variables (eg, hospital in France ADELE, region in Germany and Italy, maternal race in US California Childhood Leukemia Study (CCLS), and ethnicity in France ADELE, France ESCALE, New Zealand, US Children’s Oncology Group (COG)-E15, US CCLS, and the UK Childhood Cancer Study (UKCCS). OR estimates from individual studies were subsequently summarised to give an overall OR estimate from a meta-analysis. We used a random effects model to account for heterogeneity between studies in terms of study design and time period of exposure assessment. Summary ORs and 95% CIs, I2 statistics (a measure of variation across studies that is not due to chance)29 and forest plots were produced. These analyses were conducted separately for ALL, AML and maternal and paternal exposure. In addition, we identified other studies reporting on parental ELF-MF exposure and childhood leukaemia risk by searching PubMed. We extracted the ORs from those studies and combined them using the meta-analysis approach with the ORs for overall leukaemia from the individual studies included in the current pooled analysis. Funnel plots were produced and Egger’s test was performed to evaluate the effect of publication bias in this analysis.
In the pooled analysis, we categorised paternal occupational ELF-MF exposure at conception and maternal ELF-MF exposure during pregnancy to dichotomous exposure with categories of ≤0.2 microtesla (µT) and >0.2 µT, and polytomous exposure with categories of ≤0.1 µT, >0.1–≤0.2 µT, >0.2–≤1 µT and >1 µT. In meta-analysis, only dichotomous exposure was used.
Finally, we conducted sensitivity analyses to assess the robustness of the main findings from the pooled analyses as follows: (1) analyses stratified by child’s year of birth were conducted to take into account possible change of ELF-MF exposure level over time; (2) analyses by using maximum ELF-MF exposure for parents with multiple exposure assignment due to ‘one-to-many’ and ‘many-to-one’ job code translations were conducted to assess whether the choice of summary exposure estimate (median or maximum ELF-MF) for such persons had an effect on the risk estimates; (3) analyses restricted to datasets with job histories coded into ISCO were carried out in order to reduce ‘one-to-many’ and ‘many-to-one’ job code translations; (4) analyses stratified by child’s sex and age at diagnosis; and (5) finally, we used 0.4 µT as cut-off point for categorisation of dichotomous ELF-MF exposure.
Stata/IC V.14 was used for the meta-analyses, and R V.3.4.3 (R Core Team. 2017. R: A language and environment for statistical computing. R Foundation for Statistical Computing, Vienna, Austria. https://www.R-project.org/) was used for the pooled analyses.
Results
The ALL analysis included 8420 cases (including 5845 B-lineage and 781 T-lineage) and 16 453 controls (including 13 815 B- lineage and T-lineage ALL controls) from 11 studies. The AML analysis included 926 AML cases and 12 246 controls from 10 studies (table 2).
Selected sociodemographic and prenatal characteristics of the study population of the pooled analysis
Because of missing job histories, 578 (6.9%) ALL cases and 1152 (7.0%) controls, and 71 (7.7%) AML cases and 965 (7.9%) controls were excluded from the analysis of paternal ELF-MF exposure (table 2). For the same reason, we excluded 556 (6.6%) ALL cases and 569 (3.5%) controls, and 24 (2.6%) AML cases and 241 (2.0%) controls from the analysis of maternal ELF-MF exposure (table 2).
As expected, ALL was most common in children aged 1–4 years, while AML was more evenly distributed in children aged 2 years or more. Slightly over 50% of cases with ALL or AML were boys (table 2).
Minimum estimated exposure for both parents was 0.02 µT, and the maximum estimated exposure for fathers was 17.88 µT (railway engine driver), and for mothers, it was 5.48 µT (locomotive engine driver). The most frequent occupations in this pooled case–control dataset are shown in online supplementary table 1.
Pooled analysis
The OR for ALL related to paternal ELF-MF exposure (>0.2 µT vs ≤0.2 µT) was 1.04 (95% CI 0.95 to 1.13) and for maternal exposure it was 1.00 (95% CI 0.89 to 1.12). Similarly, no association was observed when using more categories of exposure, in particular, not in the highest exposure category >1 µT for paternal exposure (table 3).
Estimated risk of acute lymphoblastic leukaemia (ALL) and acute myeloid leukaemia (AML) in the offspring following parental occupational exposure to extremely low-frequency magnetic fields (ELF-MF) in a pooled analysis of Childhood Leukaemia International Consortium (CLIC) studies
Similarly, no evidence of an effect was found for AML. The OR for paternal exposure (>0.2 µT vs ≤0.2 µT) was 1.06 (95% CI 0.87 to 1.29) and for maternal exposure 0.85 (95% CI 0.61 to 1.16) (table 3).
The OR for all leukaemia related to paternal ELF-MF exposure (>0.2 µT vs ≤0.2 µT) was 1.04 (95% CI 0.96 to 1.13) and for maternal exposure 0.99 (95% CI 0.89 to 1.11) (table not shown).
These results did not change when maximum ELF-MF exposure was used instead of median ELF-MF exposure (data not shown). No large differences in risk estimates were observed for children born before or after 1990 (online supplementary table 2). Main results did not change also in other sensitivity analyses (online supplementary tables 3–6).
Meta-analysis
Summary OR in the meta-analysis of paternal ELF-MF exposure and ALL was 1.05 (95% CI 0.96 to 1.14) (figure 1) and in the analysis of maternal ELF-MF exposure and ALL was 0.99 (95% CI 0.88 to 1.12) (figure 1).

Parental occupational ELF-MF exposure and acute lymphoblastic leukaemia (ALL) in the offspring. CCLS, California Childhood Leukemia Study; COG, Children’s Oncology Group; ELF-MF, extremely low-frequency magnetic field; NARECHEM, Nationwide Registry for Childhood Haematological Malignancies; SETIL, Studio sulla Eziologia dei Tumori Infantili Linfoemopoietici.
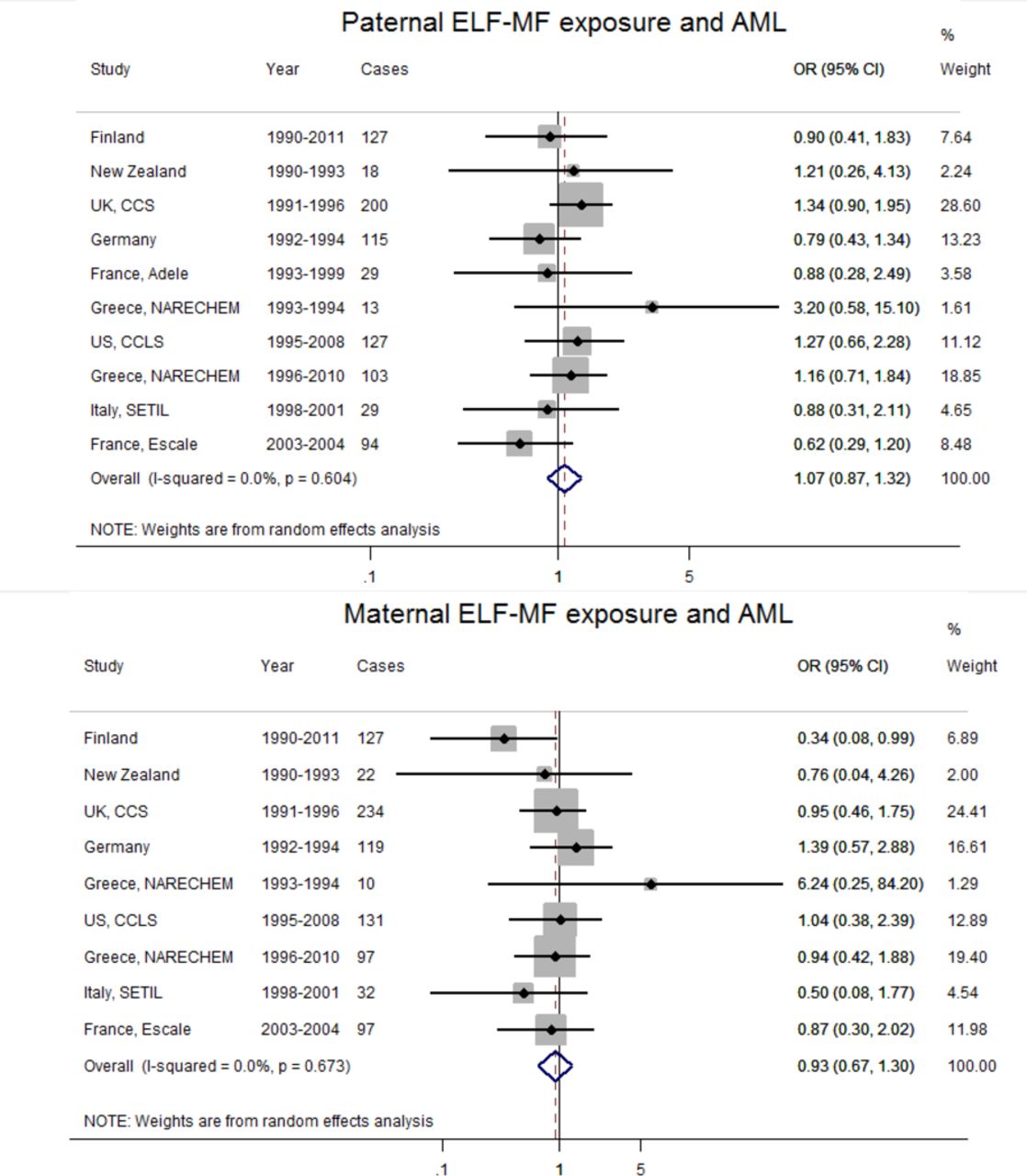
OR for paternal ELF-MF exposure and AML was 1.07 (95% CI 0.87 to 1.32) (figure 2), and for maternal ELF-MF exposure and AML it was 0.93 (95% CI 0.67 to 1.30) (figure 2). France ADELE was not included in the maternal exposure analysis because there were no mothers with exposure level >0.2 µT in this dataset (figure 2).
{kind=link}
{kind=link}
Parental occupational ELF-MF exposure and acute myeloid leukaemia (AML) in the offspring. CCLS, California Childhood Leukemia Study; COG, Children’s Oncology Group; ELF-MF, extremely low-frequency magnetic field; NARECHEM, Nationwide Registry for Childhood Haematological Malignancies; SETIL, Studio sulla Eziologia dei Tumori Infantili Linfoemopoietici.
The meta-analysis of parental ELF-MF exposure and total leukaemia included 15 studies (11 CLIC and 4 additional studies). An increased overall risk of leukaemia with borderline significance was observed for paternal ELF-MF exposure at conception (OR=1.11, 95% CI 1.00 to 1.22) (online supplementary figure 1) but not for maternal ELF-MF exposure during pregnancy (OR=1.04, 95% CI 0.92 to 1.17) (online supplementary figure 3). Funnel plot and Egger’s test (p=0.03) suggested a presence of publication bias in the analysis of parental exposure and leukaemia (online supplementary figures 3 and 4).
Discussion
In this large-scale international pooling effort, we found no clear evidence for an association between parental occupational ELF-MF exposure and ALL or AML in their offspring. This was consistent for the pooling approach and the meta-analytical approach of combining studies and confirmed in various sensitivity analyses.
A small increased risk of leukaemia in relation to paternal ELF-MF exposure in the meta-analysis of 11 CLIC plus four other published studies must have been due to the added studies especially from the UK and Russia, because this association was not observed for the CLIC pooled studies. With the addition of those studies, exposure assessment was no longer harmonised. Moreover, funnel plot and Egger’s test suggested the presence of publication bias. It appears to confirm what was previously suggested by Hug et al,22 namely that publication bias is a concern, confirming the need of studying this exposure in an unbiased dataset with regard to the original hypothesis, as discussed in more detail below.
Two of the studies included in our analyses, the German Childhood Cancer Registry and the UK Childhood Cancer Study (UKCCS) had already published their findings,21 22 and their individual findings were consistent with the current analyses. Two other studies that are part of the CLIC consortium, the Quebec study20 and Aus-ALL from Australia,23 were not included in these analyses since both used expert assessment rather than quantitative JEM. While the earliest of these by Infante-Rivard and Deadman20 in Quebec observed an increased risk of childhood leukaemia (OR=2.5, 95% CI 1.2 to 5.0) for maternal ELF-MF exposure during pregnancy for exposure level ≥0.4 µT, the findings of the later Australian study were consistent with ours, despite the different method of exposure assessment.
Among studies that are not part of CLIC, our findings were inconsistent with the results from Pearce et al 19 and Smulevich et al.18 Pearce et al 19 included cases diagnosed between 1968 and 2000 in the UK, which has some overlap with the UKCCS among cases diagnosed between 1991 and 1996. Pearce et al 19 found an increased leukaemia risk in relation to paternal occupational electromagnetic field exposure (OR=1.31, 95% CI 1.02 to 1.69),19 and Smulevich et al 18 reported increased risk in relation to both parents’ exposure (OR=4.6, 95% CI 1.8 to 11.9 for fathers’ exposure, and OR=5.2, 95% CI 1.6 to 16.8 for mothers’ exposure).18 However, these results should be interpreted with caution. For example, in Pearce et al 19 and Smulevich et al,18 only those occupations categorised as probably exposed and probably unexposed were considered. Moreover, results from Smulevich et al 18 were based on a small number of events: 14 cases in the analysis of paternal exposure and 10 cases in the analysis of maternal exposure. As previously stated, a meta-analysis of studies published at that time showed strong evidence of publication bias.22 This is in line with our finding of no association based on the sample of CLIC studies alone but an increased OR with the addition of the remaining studies with positive associations from the literature.
The strengths of this study include its large size. It is the largest study to assess parental ELF-MF exposure and childhood leukaemia to date. Childhood leukaemia is relatively rare, and high ELF-MF exposure is also rare in the general population, so a large study is required to detect potential risks should they exist. Completeness of parental job history data was another advantage of our study. The vast majority of women included in CLIC datasets had the same job in pregnancy as in the period prior to conception.26 Among the studies that had information about more than one job during pregnancy, we used the information if any of the jobs was associated with exposure. In total, only 6.8% of paternal and 4.3% of data on maternal job histories were missing, while detailed job histories with start and end dates of each job were available in most included studies. We quantified parental occupational ELF-MF exposures by linking parental jobs at the relevant time period to an ELF-MF JEM. Using an ELF-MF JEM for exposure estimation is a more rigorous method compared with merely grouping persons into exposed versus unexposed categories and allows harmonisation across studies. In addition, the ELF-MF JEM used in our study is quantitative and based on real ELF-MF workplace measurement series in the occupational setting.27 As described in the Methods, the ELF-MF JEM was developed independently from our study; however, it was for an international collaboration capturing similar countries and the same time period as our pooled dataset, therefore it was well applicable for our setting.
The major limitation of this study was potential exposure misclassification, which can arise in any study with retrospective exposure assessment. Exposure misclassification could occur because the ELF-MF JEM, like most JEMs, assigns the mean exposure level to all persons in the same occupation, while exposure heterogeneity within the occupation may be substantial. It does not specify jobs by industrial groups, and exposure intensity might vary in the same occupation by industrial group. Finally, when national codes were translated to ISCO, this resulted in ‘one-to-many’ and ‘many-to-one’ job code translations, which introduced further exposure uncertainty for some persons. We assessed the effect of the latter by restricting analyses to studies using the ISCO classification, and the main results did not change, suggesting that ‘one-to-many’ and ‘many-to-one’ job code translations had no effect on the risk estimates. Exposure misclassification was likely to be non-differential in our study because the JEM was applied in the same way to all parents and independently of case–control status of the child. Bias from non-differential exposure misclassification is generally towards the null for dichotomous exposures.30 For polytomous exposures, non-differential misclassification can bias ORs away from the null only for intermediate exposure categories, but ORs for the highest category will be towards the null.31 Therefore, ORs for dichotomous ELF-MF exposures and for high categories of polytomous exposures would be underestimated if non-differential exposure misclassification was present in this study.
Selection bias may also be a concern in this study. In most of the included studies, higher response rates of case parents compared with control parents, and mothers compared with fathers were noted.26 Selection bias could occur also in analyses of maternal exposure and ALL, because 6.6% case mothers were excluded from the analysis compared with only 3.5% control mothers due to missing occupational data. Recall bias is, however, unlikely to be an issue in the present study because job title rather than exposure information was collected from study participants. It has been shown that the validity and reliability of self-reported job histories obtained using an interview-administered questionnaire are generally good and not subject to recall bias.32 33
In conclusion, using a large international pool of case–control studies and a detailed quantitative JEM, we did not find any evidence for an association between fathers’ occupational ELF-MF exposures around the time of conception or mothers’ occupational ELF-MF exposures during pregnancy and leukaemia in their offspring. Considering our findings and those of previous smaller less consistent studies together suggests that parental ELF-MF exposure plays no relevant role in the aetiology of childhood leukaemia.
Acknowledgments
The authors would like to thank Veronique Luzon (International Agency for Research on Cancer (IARC)) for her skilful data management for the CLIC Data Coordination Center. The authors would also like to thank Sini Erme, MD (Tampere University Hospital) for contributions to the Finnish study. For the Germany GCCR study, we would like to thank Drs Peter Kaatsch, Rolf Meinert, Uwe Kaletsch and Jörg Michaelis for their work in the original study. For the Greece NARECHEM study, we would like to thank Nick Dessypris. For New Zealand, GP Herbison, DCG Skegg and JM Elwood are thanked for their contributions to the original study. For Italy, SETIL, Alessandra Benvenuti and Patrizia Legittimo (Occupational and Environmental Epidemiology Unit, ISPRO Cancer Prevention and Research Institute, Florence, Italy), Marco Gilardetti and Assunta Rasulo (Cancer Epidemiology Unit, CPO Piedmont and University of Turin, Torino, Italy) and Alessandra Ranucci (Cancer Epidemiology Unit, Department of Translational Medicine, CPO Piedmont and University of Eastern Piedmont, Novara, Italy). The SETIL (Italian Multicentric Epidemiological Study on Risk Factors of Childhood Leukaemia, Non-Hodgkin Lymphoma and Neuroblastoma) Working Group was listed in: Magnani C, Mattioli S, Miligi L et al. SETIL: Italian multicentric epidemiological case-control study on risk factors for childhood leukaemia, non hodgkin lymphoma and neuroblastoma: study population and prevalence of risk factors in Italy. Ital J Pediatr. 2014;40:103. doi: 10.1186/s13052-014-0103-5. The authors would also like to thank research investigator from French studies ADELE and ESCALE, Jacqueline Clavel ,and principal investigators from The Société Française de lutte contre les Cancers de l’Enfant et de l’Adolescent (SFCE): André Baruchel (Hôpital Saint-Louis/Hôpital Robert Debré, Paris), Claire Berger (Centre Hospitalier Universitaire, Saint-Etienne), Christophe Bergeron (Centre Léon Bérard, Lyon), Jean-Louis Bernard (Hôpital La Timone, Marseille), Yves Bertrand (Hôpital Debrousse, Lyon), Pierre Bordigoni (Centre Hospitalier Universitaire, Nancy), Patrick Boutard (Centre Hospitalier Régional Universitaire, Caen), Gérard Couillault (Hôpital d’Enfants, Dijon), Christophe Piguet (Centre Hospitalier Régional Universitaire, Limoges), Anne-Sophie Defachelles (Centre Oscar Lambret, Lille), François Demeocq (Hôpital Hôtel-Dieu, Clermont-Ferrand), Alain Fischer (Hôpital des Enfants Malades, Paris), Virginie Gandemer (Centre Hospitalier Universitaire – Hôpital Sud, Rennes), Dominique Valteau-Couanet (Institut Gustave Roussy, Villejuif), Jean-Pierre Lamagnere (Centre Gatien de Clocheville, Tours), Françoise Lapierre (Centre Hospitalier Universitaire Jean Bernard, Poitiers), Guy Leverger (Hôpital Armand-Trousseau, Paris), Patrick Lutz (Hôpital de Hautepierre, Strasbourg), Geneviève Margueritte (Hôpital Arnaud de Villeneuve, Montpellier), Françoise Mechinaud (Hôpital Mère et Enfants, Nantes), Gérard Michel (Hôpital La Timone, Marseille), Frédéric Millot (Centre Hospitalier Universitaire Jean Bernard, Poitiers), Martine Münzer (American Memorial Hospital, Reims), Brigitte Nelken (Hôpital Jeanne de Flandre, Lille), Hélène Pacquement (Institut Curie, Paris), Brigitte Pautard (Centre Hospitalier Universitaire, Amiens), Stéphane Ducassou (Hôpital Pellegrin Tripode, Bordeaux), Alain Pierre-Kahn (Hôpital Enfants Malades, Paris), Emmanuel Plouvier (Centre Hospitalier Régional, Besançon), Xavier Rialland (Centre Hospitalier Universitaire, Angers), Alain Robert (Hôpital des Enfants, Toulouse), Hervé Rubie (Hôpital des Enfants, Toulouse), Stéphanie Haouy (Hôpital Arnaud de Villeneuve, Montpellier), Christine Soler (Fondation Lenval, Nice) and Jean-Pierre Vannier (Hôpital Charles Nicolle, Rouen).
References
Footnotes
Contributors MT, JS, AO, FE and HB designed the study. MT conducted data analyses and wrote the manuscript. The results were interpreted and manuscript was revised by all authors.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Ethics approval Individual studies were approved by their respective ethical committees (COG-E15 study: Minnesota Human Subjects Research Protection Program, study approval number 1403E49261; ADELE study: CNIL (339392) – RBM (CCPPRB 1995/9443); ESCALE study: CNIL (902162) – RBM (DGS 2003/0259); CCLS study: Committee for Protection of Human Subjects (CPHS), University of California, Berkeley, CPHS Protocol Number 2010-10-2438; NZCCS study: Ethical Committees of Waikato Area Health Board RDL:JD, Auckland Area Health Board 90/20 Committee B, Otago Area Health Board 216 00001207, Southland Area Health Board 13-3-1-7, West Coast Area Health Board, Nelson Marlborough Area Health Board, Hawkes Bay Area Health Board 1991/5, Manawatu-Manganui Area Health Board 2/91, Taranaki Area Health Board, Tairawhiti Area Health Board, Bay of Plenty Area Health Board, Canterbury Area Health Board WJP/AQ, Wellington Area Health Board Te Waiora a Tara 90/82; GCCR study: ethical and data protection approval granted by University of Mainz, 1990 (IMSD-1990); SETIL study: Ethical Review Board for the Piedmont Region, authorisation n. 2886, on 15/2/1999, letter n. 1852/28.3 on 17/2/1999; UKCCS study: Yorkshire and the Humber – Leeds West Research Ethics Committee 18/YHO/0135; Integrated Research Application System 203822; Confidential Advisory Group (CAG) 18/CAG/0066; Greece NARECHEM 1993-1994 study: no ethics committee had been established at that time; the dataset was used in doctoral thesis supervised by the principal investigator E Petridou; Greece NARECHEM 1996-2011 study: Ethics Committee of the National and Kapodistrian University of Athens, letter on 20 March 2000, authorization n. 5097 on 17 February 2012 and authorisation n. 1516003877 on 9 October 2015 as the study expanded; written informed consents obtained from family members who provided data in the presence of the child). In interview-based studies, written informed consent was obtained from family members who provided data.
Provenance and peer review Not commissioned; externally peer reviewed.
Correction notice This article has been corrected since it published Online First.
Patient consent for publication Not required.