Article Text

Abstract
Objectives We investigated work-unit exit, total and long-term sickness absence following organisational change among public healthcare employees.
Methods The study population comprised employees from the Capital Region of Denmark (n=14 388). Data on reorganisation at the work-unit level (merger, demerger, relocation, change of management, employee layoff or budget cut) between July and December 2013 were obtained via surveys distributed to the managers of each work unit. Individual-level data on work-unit exit, total and long-term sickness absence (≥29 days) in 2014 were obtained from company registries. For exposure to any, each type or number of reorganisations (1, 2 or ≥3), the HRs and 95% CIs for subsequent work-unit exit were estimated by Cox regression, and the risk for total and long-term sickness absence were estimated by zero-inflated Poisson regression.
Results Reorganisation was associated with subsequent work-unit exit (HR 1.10, 95% CI 1.01 to 1.19) in the year after reorganisation. This association was specifically important for exposure to ≥3 types of changes (HR 1.52, 95% CI 1.30 to 1.79), merger (HR 1.29, 95% CI 1.12 to 1.49), demerger (HR 1.41, 95% CI 1.16 to 1.71) or change of management (HR 1.24, 95% CI 1.11 to 1.38). Among the employees remaining in the work unit, reorganisation was also associated with more events of long-term sickness absence (OR 1.15, 95% CI 1.00 to 1.33), which was particularly important for merger (OR 1.31, 95% CI 1.00 to 1.72) and employee layoff (OR 1.31, 95% CI 1.08 to 1.59).
Conclusions Specific types of reorganisation seem to have a dual impact on subsequent work-unit exit and sickness absence in the year after change.
- sickness absence
- organizational change
- reorganization
- health care workers
- turnover
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Key messages
What is already known about this subject?
Previous studies examining the impact of organisational change mainly focused on downsizing or merger at the company level to find that these types of reorganisation were related to employee exit from the workplace or a higher risk of sickness absence among the remaining employees.
However, the potential dual impact of subsequent workplace exit and sickness absence following various types of organisational change remains to be examined at the work-unit level.
What are the new findings?
This study demonstrates a dual impact of individual-level subsequent employee exit from the work unit and sickness absence in the year after six types of organisational change measured at the work-unit level among 14 388 healthcare employees in the Capital Region of Denmark.
How might this impact on policy or clinical practice in the foreseeable future?
Decision and policy makers should consider the potential adverse effects of organisational change in a work unit.
Introduction
Organisational change at the workplace is common and may be regarded as a feature of modern work life.1 2 Evidence indicates that organisational changes are associated with deleterious health and psychosocial outcomes,3–7 and consequently, subsequent employee exit from the workplace8–11 and higher risk of sickness absence (SA).12–16Reorganisation may become counterproductive since workplace exit and SA are highly costly due to long-term stress-related illness, loss of productivity and costs related to replacement of employees.9 17–19
Studies of the healthcare sector have shown higher exit rates following implementation of new workflows10 and hospital mergers across occupational groups regardless of employee health.11 Also, higher exit rates have been found, especially among senior employees, following merger of computer companies9 in line with other findings of higher rates of voluntary early retirement among senior employees exposed to various types of reorganisation.8
Regarding SA, epidemiological studies found major downsizing (ie, staff reduction) and workplace expansion to be associated with more SA13 and a higher risk of long-term SA.5 A study from Norway demonstrated that merger, demerger, relocation and creation or shut-down of units aggregated at the hospital level was associated with total and long-term SA, but the various types of reorganisation were not examined separately.14 Another study found modest risks of long-term SA during hospital merger and 2, 3 and 4 years after merger.16 Although there is some evidence that reorganisation adversely affects SA,15 other studies found SA rates to be unaffected20 or even decreased in women21 following downsizing or expansion.
A limitation of previous studies of SA is that they mainly focused on employees who remained at the workplace7 without studying the potential accompanied effect of employees subsequently exiting their workplace after reorganisation. Indeed, one study has linked higher rates of workplace exit and long-term SA to self-reported negative consequences of reorganisation,22 whereas another study found no higher risk of long-term SA after privatisation of public-sector work units without major downsizing.23
We examine the impact of various types of organisational change on subsequent employee exit from the work unit, total SA and long-term SA among public healthcare employees in Denmark.
Methods and materials
Population and study design
This longitudinal study used data from the Well-being in Hospital Employees (WHALE) cohort.24 The target population was established 13 January 2014 for distribution of a work-environment survey to 37 720 employees nested in 2696 work units during March 2014.
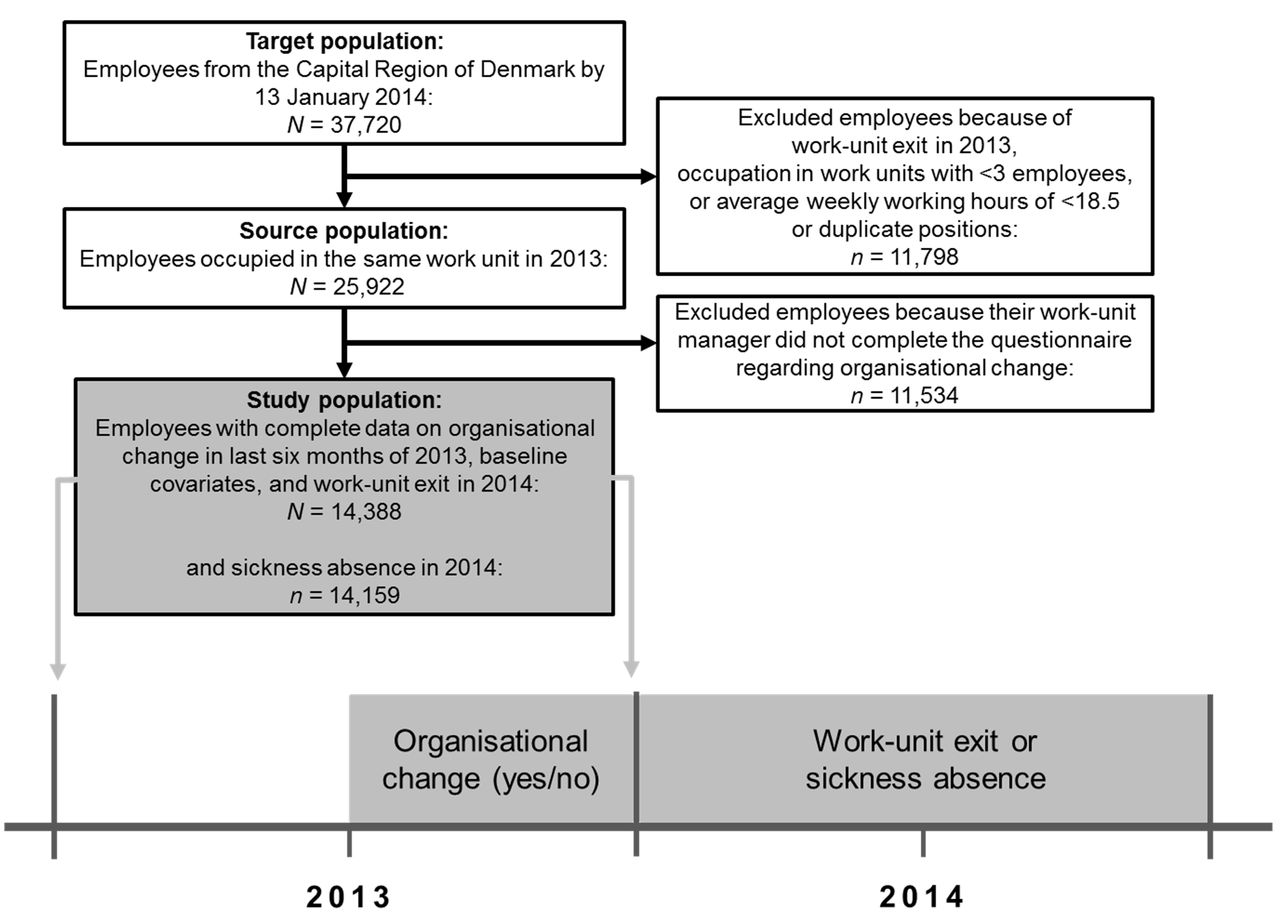
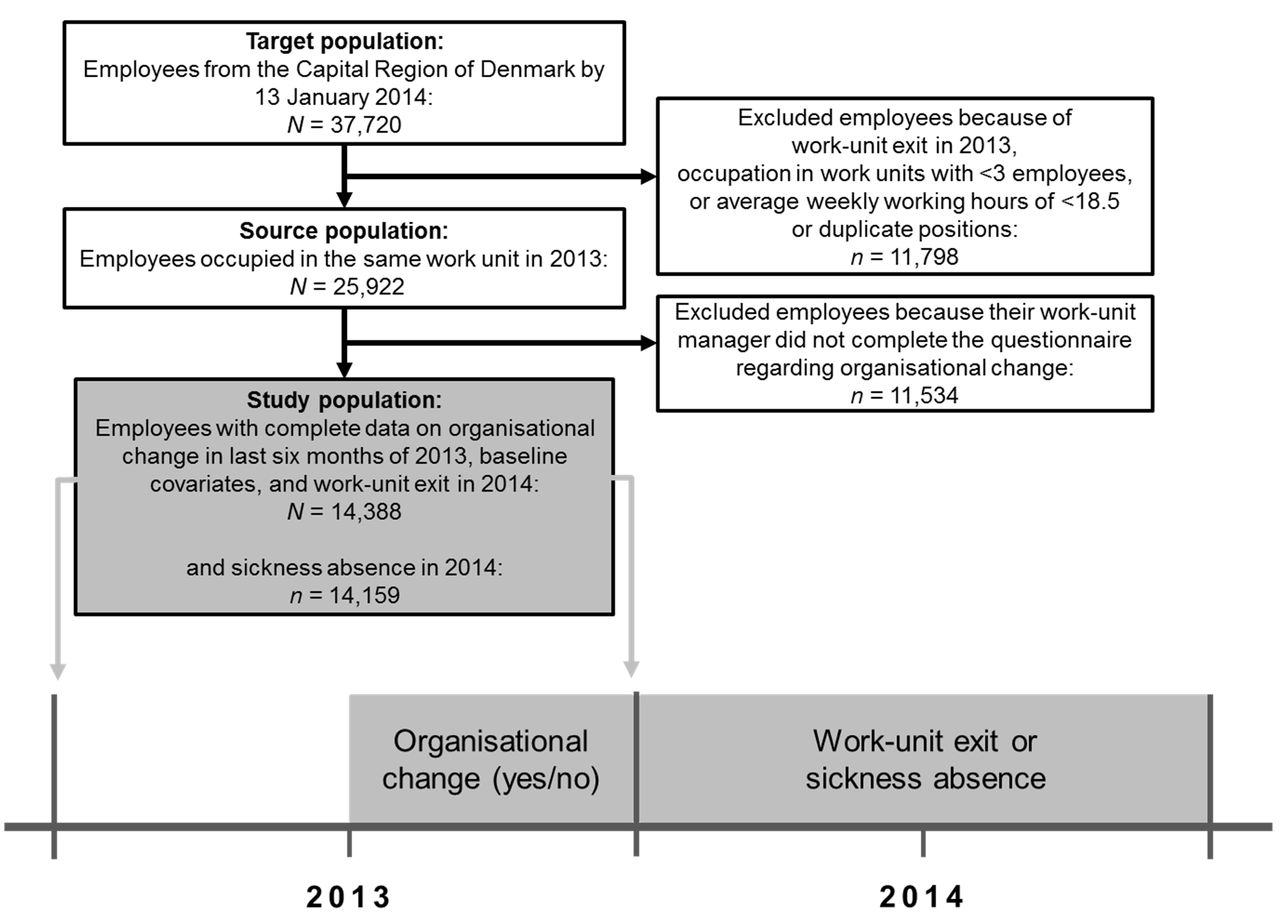
The source population comprised employees each actively occupied in the same work unit of ≥3 employees with an average of ≥18.5 fixed working hours per week through 2013. To ensure that all employees worked in the same work unit through 2013 (although some work units changed their name), we applied the criteria that ≥3 employees and ≥30% of all employees from a given work unit must remain together after a change to be included. In the source population, there were 25 922 employees nested in 2322 work units (figure 1).
{kind=link}
Diagram representing the flow of participants and the study design. The study population of employees occupied in the same work unit in 2013 were potentially exposed to organisational change in the last six months of 2013 with follow-up on subsequent work-unit exit, total sickness absence or long-term sickness absence in 2014. Data on organisational change were collected between April and June 2016.
Organisational change
Between April and June 2016, semi-annual binary data on organisational change at the work-unit level (ie, merger, demerger, relocation, change of management, employee layoff(s), budget cuts) from 2011 to 2013 were obtained via a survey (see online supplementary material 1) emailed to the work-unit managers (response rate: 59%). The measures of organisational change included exposure to no change (reference group), any type of change, each of the six types of change (not mutually exclusive) or the number of simultaneous changes (only 1, 2 or ≥3 types of changes) in the last six months of 2013.
Supplementary file 1
Work-unit exit and sickness absence
Monthly work-unit affiliation and absence data for each individual employee occupied in the period from 1 January 2012 to 31 December 2014 were recorded from registries in the Capital Region of Denmark. Data on absence included total SA (ie, all types), long-term SA (ie, ≥29 consecutive days) and absence related to child’s first or second sick day. Data on background information included age, sex, occupational group, number of employees in the work units and fixed working hours. Based on the work-unit criteria stated above, we calculated subsequent monthly work-unit exit at the individual level between January and December 2014.
The two measures of SA were computed as percentages of the working hours missed in 2014 until work-unit exit due to total and long-term SA. The SA measures were calculated relative to the working hours to account for sickness periods overlapping with days off work and work-unit exit in 2014. For example, if an employee was sick on Monday (one working day), but was free from work the following Tuesday through Thursday and returned to work on Friday, it would otherwise appear in the records as the employee had 4 days of SA (ie, Monday through Thursday). Moreover, if an employee exited the work unit by 28 February 2014 during follow-up, the percentages of missed working hours due to SA were calculated relative to the fixed working hours between baseline at 1 January 2014 and work-unit exit by 28 February 2014. We examined both total and long-term SA because the total measure focuses on all types of SA (eg, short-term sickness, intermittent disorder), whereas the long-term measure focuses only on severe SA.
Covariates
The following variables were a priori considered as potential confounders for the association between organisational change and subsequent work-unit exit or total or long-term SA: age (quartiles), sex, number of employees in the work units (quartiles), occupation (six groups), days of SA in the year prior to reorganisation in 2012 (divided into five groups), child-related absence between 2012 and 2013 and personal gross income (quartiles) in 2012.
The study population of 14 388 employees was nested in 1245 work units. There were SA data on 14 159 employees, as 229 employees (1.59% of the study population) exited their work unit by 1 January 2014 (figure 1).
Statistical analyses
To assess the a priori impact of missing data on exposure to organisational change, we estimated the differences in subsequent work-unit exit, SA and baseline characteristics between employees with and without data on change. χ2 tests were used for categorical variables and two-way t-tests were used for continuous variables.
The employees were followed from 1 January 2014 to work-unit exit, censoring (ie, death) or end of the study by 31 December 2014, whichever came first. Using Cox proportional hazards regression analyses, we estimated work-unit exit rates in 2014 related to each measure of change compared with no change through 2013.
Since a large proportion of employees had no SA (ie, 0 percentage), we used zero-inflated Poisson regression analyses to assess the risk of total and long-term SA after organisational change. The zero-inflated Poisson regression comprises two components in the same operation: in this study, a zero model that generates the OR and 95% CI for SA eventsi (sick: yes/no) and a Poisson model that account for the excess count of zeros and generates the rate ratio (RR) and 95% CI for a higher percentage of SA relative to the fixed working hours among the sick-listed.25 In sum, this adds up to four absence outcomes: ORs and RRs for the event and percentage, respectively, of total SA, and ORs and RRs for the event and percentage, respectively, of long-term SA.
The reference group for all Cox and zero-inflated Poisson analyses employees who did not experience any organisational change in the last six months of 2013. Exposure to any organisational change (yes/no) was entered in the models as one variable. Exposure to each of the six types of change was estimated in separate models with each single change variable (yes/no) entered in turn. To avoid potential overadjustment, we did not include any of the remaining types of changes in the model, because the relationships between each change measure and the others are unclear (eg, they could be mediators or confounders). Exposure to the number of changes performed simultaneously (1, 2, ≥3) was modelled as one variable.
Crude Cox regression analyses were controlled for age only. Adjusted Cox and all zero-inflated Poisson regression analyses were controlled for age, sex, number of employees within work unit, occupation, previous SA, child-related absence and personal income.
All statistical analyses were conducted using SAS V.9.4 (SAS Institute, Cary, North Carolina, USA).
Results
Table 1 shows for the study population, the distribution and prevalence of exposure to any organisational change across covariate levels.
Distribution of the study population with complete data on all relevant variables and the prevalence of organisational change across covariate levels at baseline at 31 December 2013
Table 2 shows for the employees exposed to organisational change, the prevalence and distribution of exposure to each type of change across number of simultaneous changes. This table indicates that employee layoff and budget cuts were often exclusively featured together or alone. Of the 8847 changes experienced by all employees, 5022 (57%) changes were experienced in combination with ≥1 other type of change. A correlation matrix between all types of change showed that no measures were completely overlapping (r=0.07–0.33, p<0.001; online supplementary material 2).
Supplementary file 2
Prevalence and distribution of types of organisational change across number of organisational changes performed simultaneously
In total, seven employees in the study population were censored due to death during follow-up in 2014. Table 3 shows the work-unit exit rates following exposure to any, each type and number of organisational changes relative to no change. Employees exposed to change in the last six months of 2013 were more likely to exit the work unit in 2014 relative to no change in the same period.
Rates of subsequent employee exit from the work unit in the year after organisational change
Table 4 shows the risks of the event and higher percentages of missed working hours in 2014 due to total and long-term SA following organisational change through 2013 relative to no change. Employees exposed to reorganisation had an elevated rate of total SA percentage and were more likely to have SA periods of at least 29 days in 2014 compared with employees who underwent no change.
Risk of sickness absence event and higher percentage of sickness absence relative to working hours in the year after organisational change.
The Χ2 tests revealed that employees with data on change were less likely to subsequently exit their work unit (χ2(1)=22.90, p<0.001); however, they had comparable events of long-term SA (χ2(1)=0.32, p=0.57) in 2014 relative to employees without data on change. The two-way t-test showed that the employees with data on change had a significantly lower percentage of total SA in 2014 (M=4.52, SD=8.30, t(14 161)=65.02, p<0.001) compared with the employees without change data (M=4.65, SD=9.04). This points to underestimation of the effects reported in tables 3–4. There were no noteworthy differences between employees with and without change data regarding the remaining outcomes and selected baseline characteristics (see online supplementary material 3).
Supplementary file 3
In post hoc, we examined potential differential effects for men and women on subsequent work-unit exit or SA by including an interaction term between any organisational change and sex. The results did not support that sex interacted on the multiplicative scale in the relations between exposure to any change and total SA, long-term SA or subsequent work-unit exit (results not shown).
Discussion
We show higher rates of subsequent work-unit exit among employees in the year following reorganisation, especially for exposure to ≥3 types of changes, merger, demerger, relocation or change of management. Interestingly, exposure to employee layoff or budget cut was not associated with subsequent work-unit exit. Reorganisation was also associated with a higher risk of long-term SA and elevated rates of total and long-term SA percentages after exposure to 2 or ≥3 types of changes. All findings should be interpreted in the context of a relatively low unemployment rate of 5.3% through 2014 in the Capital Region of Denmark,26 as unemployment rates are negatively correlated with turnover rates27 and long-term SA.28
Work-unit exit
The present findings of higher exit rates are similar to a study examining voluntary early retirement among senior employees in the Capital Region of Denmark. This study found higher retirement rates following merger, change of management and relocation at the work-unit level8 concurrent with the present findings. Among 54 787 hospital employees in Norway, Ingelsrud11 found a higher exit rate from the hospital sector only in the second year following hospital merger, whereas we found higher exit rates in the first year after the work-unit merger. Exposure to employee layoff and budget cut were not significantly associated with higher rates of subsequent work-unit exit. This may be explained by the observation that this pair of changes was commonly featured together or alone. Building on this, we found that exposure to only 1 or 2 types of changes were not significantly associated with subsequent work-unit exit, whereas exposure to ≥3 types of changes was associated with a 1.52-fold higher exit rate relative to no change.
The reasons of work-unit exit were not examined in the present study. Some employees may voluntarily exit after changes,8 whereas some changes may have the tacit or explicit purpose of ‘pushing out’ employees of the workplace. Demerger may be such latter example as it was related to a particularly large exit effect and no effect of SA. The large exit effect after demerger could also be due to co-occurring changes since about half of the employees exposed to demerger were exposed to ≥3 simultaneous changes.
We added to this literature by distinguishing and comparing the impact of various types of reorganisations, and we found that some, but not all, types of reorganisations are related to higher rates of subsequent work-unit exit.
Sickness absence
In all SA analyses, more Poisson-model estimates were statistically significant than zero-model estimates. This pattern may be explained by the larger statistical power introduced by the Poisson distribution compared with the binary distribution as indicated by the 95% CIs in table 4.
The present results of higher rates of total SA following reorganisation correspond to previous findings after major downsizing only in permanent employees.13 Kjekshus et al 16 found elevated ORs for long-term SA of 1.05 during hospital merger and 1.04 in the second year after merger, which are smaller than the OR for long-term SA of 1.33 in the year following work-unit merger demonstrated in this study. The difference between these findings may be due to the work-unit approach applied presently ensuring that the exposed employees did de facto experience the merger. Our findings of higher risk for long-term SA of ≥29 days among various occupational groups after reorganisation are inconsistent with other findings23 of no higher risk for long-term SA of ≥91 days among hospital laboratorians and radiographers. This inconsistency may be explained by the social gradient in health between the populations studied and the conservative measure of long-term SA applied by Kokkinen et al.23
In general, those types of organisational changes associated with a higher exit rate were also associated with a higher risk of SA. This suggests that organisational change has a dual impact on subsequent work-unit exit and SA. Interestingly, employee layoff was not associated with a higher work-unit exit rate, but it was associated with a large OR for events of long-term SA and a relatively large RR for a higher percentage of SA among the remaining employees. This may be explained by the potentially higher job insecurity and lower job control among the remaining employees after a staff reduction,29 which may manifest as more SA. To the extent of our knowledge, only a single study has investigated potential work-environmental mediators between organisational change and SA, which found that higher job insecurity, physical demands and lower job control mediated the longitudinal association between downsizing and higher risk of long-term SA.30 Recent findings imply that supporting and redeploying employees as a part of downsizing is important for well-being of the workers.31 Thus, it is reasonable that workplace social capital may mediate adverse effects of organisational change since this concept is linked to health status32 33 and comprises aspects of organisational justice, trust and collaboration.8
We did not find differential adverse effects of organisational change between men and women in contrast to another study in the context of downsizing.34 This study showed that female employees with depression had a higher risk of exit out of employment, whereas unemployment in male employees was unaffected by their health status. Therefore, the lack of interaction between organisational change and sex in the present analyses may be ruled out by adjusting for previous SA.
In sum, the present findings of higher exit rates and SA following change seem to be related to specific types of change rather than a dose-response relation of the number of changes performed simultaneously. More studies are needed to examine the dual effects of reorganisation on health among employees exiting and remaining on the workplace, as the literature point to poor health outcomes in both groups.35 A Swedish study found that job loss predicted new events of subsequent major depression in both sexes with a larger effect size in men,34 yet the present study did not demonstrate an interaction between any change and sex. Future research should elucidate potential mediators of the detrimental effects from organisational change as such factors may comprise targets for interventions to buffer these effects.
Strengths and limitations
This study has several strengths. First, we examined employee exit and SA simultaneously as these job withdrawal behaviours depend on each other. Second, data on organisational change were obtained from a different source than the outcomes, which hamper common method bias.36 Third, following of the participants and measurement of organisational change were conducted at the work-unit level ensuring that the participants were actually affected by the organisational change in question. Fourth, it was also a strength that we were able to distinguish between six common types of organisational change adding to the detailed nature of the study.
Potential limitations are stated in the following. First, missing data on organisational change may contribute to an underestimation of the outcome effects, since the rate of subsequent work-unit exit and the percentage of total SA were slightly lower during 2014 among employees with data on change than employees without these data. Indeed, there was no significant difference between these employee groups regarding events of long-term SA in 2014. Second, data on reorganisation were retrieved retrospectively, which may have biased these data as organisational change itself could have affected the managers to leave their job and thus not provide reorganisation information in the online survey. However, we were able to contact managers who remained in the organisation, because their email address was not changed. Third, we were unable to examine the potential effects of work-unit exit and SA before or during the actual reorganisation. Indeed, findings from post hoc analyses showed only a minor effect on total SA in the first quarter of 2014 (results not shown), suggesting that the SA effects—if any—were small before or during exposure to organisational change. Fourth, the analyses did not take into account the multilevel organisational structure of the data. For consistency reasons, we choose not to use multilevel modelling as this approach was unable to converge in a zero-inflated Poisson regression model. A post hoc Cox analysis clustering employees within work units revealed an exit rate after any change of 1.12 (vs 1.10 in table 3), which suggests only a small underestimation by using a single-level approach. Fifth, a zero-inflated negative binomial Poisson model showed a superior fit with long-term SA as outcome compared with the present approach, suggesting potential overdispersion in the Poisson distribution of the long-term sickness data. Indeed, the zero-inflated negative binomial Poisson model was unable to converge with total SA as outcome. Finally, the present results cannot be attributed exclusively to each type of change as some changes are likely to be performed simultaneously and each type of change were modelled separately. Entering all six types of change variables into the same model would likely result in overadjustment because some changes may mediate other changes. Tentatively, we explored the relationships between changes by mutually adjusting for the four most correlated pair of changes in the correlation matrix (see online supplementary material 2), which generally showed similar findings, although merger/demerger adjustment seemed to have a marked role in exit rates towards null (merger: HRs from 1.29 to 1.14; demerger: HRs from 1.41 to 1.00). This could be due to the observation that 92% of the 232 employees exposed to both merger and demerger were exposed to a total of ≥3 changes. Hence, overadjustment is introduced due to impurity of the change variables, which is supported by the finding that simultaneous changes was strongly related to subsequent exit, whereas 1 or 2 changes were not.
These findings indicate that specific types of organisational change frequently occurring in the public healthcare sector have a dual impact on subsequent employee exit from the work unit and total and long-term SA among remaining employees in the year following reorganisation. Generalisations to other public sectors should be made cautiously due to various contextual factors, including sex composition.
Acknowledgments
The authors thank human-resource consultant Charlotte Hyldtoft and data consultant Jesper Strøyer Andersen from the Capital Region of Denmark for their great help and contribution to this study by providing the applied data from regional registries.
References
Footnotes
↵i For interpretation reasons, we inverted the output values to predict the OR of having sickness absence (one divided by output values).
Contributors JHJ had full access to all data provided in the present study and takes responsibility for the integrity and the accuracy of the data analyses. All authors were responsible for the current study design. JHJ wrote the initial draft of the manuscript. All authors contributed to the present study and approved the final draft of the manuscript.
Funding The study was funded by The Danish Working Environment Research Fund (project number: 13-2015-03).
Competing interests None declared.
Patient consent Not required.
Ethics approval The Regional Ethics Committees of the Capital Region stated that ethical approval was not required for this study.
Provenance and peer review Not commissioned; externally peer reviewed.