Article Text

Abstract
Objectives Depression can negatively impact work capacity, but treatment effects on sick leave and employment are unclear. This study evaluates if internet-based cognitive behavioural therapy (ICBT) or physical exercise (PE), with already reported positive effects on clinical outcome and short-term work ability, has better effects on employment, sick leave and long-term work ability compared with treatment as usual (TAU) for depressed primary care patients (German clinical trials: DRKS00008745).
Methods After randomisation and exclusion of patients not relevant for work-related analysis, patients were divided into two subgroups: initially unemployed (total n=118) evaluated on employment, and employed (total n=703) evaluated on long-term sick leave. Secondary outcomes were self-rated work ability and average number of sick days per month evaluated for both subgroups. Assessments (self-reports) were made at baseline and follow-up at 3 and 12 months.
Results For the initially unemployed subgroup, 52.6% were employed after 1 year (response rate 82%). Both PE (risk ratio (RR)=0.44; 95% CI 0.23 to 0.87) and ICBT (RR=0.37; 95% CI 0.16 to 0.84) showed lower rates compared with TAU after 3 months, but no difference was found after 1 year (PE: RR=0.97; 95% CI 0.69 to 1.57; ICBT: RR=1.23; 95% CI 0.72 to 2.13). For those with initial employment, long-term sick leave (response rate 75%) decreased from 7.8% to 6.5%, but neither PE (RR=1.4; 95% CI 0.52 to 3.74) nor ICBT (RR=0.99; 95% CI 0.39 to 2.46) decreased more than TAU, although a temporary positive effect for PE was found. All groups increased self-rated work ability with no differences found.
Conclusions No long-term effects were found for the initially unemployed on employment status or for the initially employed on sick leave. New types of interventions need to be explored.
- return to work
- internet therapy
- physical exercise
- cognitive behavioral therapy
- depression
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
What this paper adds
Depression and other common mental health problems can affect work negatively.
Previous studies on interventions regarding sick leave and employment are inconclusive and often based on smaller trials.
Even though internet-based cognitive behavioural therapy and supported physical exercise for depressed patients were superior to regular primary care treatment in reducing symptoms, all three interventions were still equally effective in reducing sick leave and unemployment after 12 months.
The large number of participants evaluated on sick leave (n=759) makes the finding that symptom reduction may not be enough rather strong, and implies that other types of interventions need to be considered in return to work policies and future research.
Introduction
Depression is a major cause of long-term sickness absence.1 Being away from work may offer relief from hard mental and interpersonal tasks, but work also promotes better life quality.2 A recent review found that for patients with common mental disorders, including depression, workplace and clinical interventions did not have an effect on return to work but somewhat reduced the number of sick days.3 A meta-analytic review focused on depression concluded that cognitive behavioural therapy (CBT) had a positive effect on sickness absence that was stronger than usual care alone when three studies were analysed together,4 although none of the studies provided significant effects on their own.5–7 Work-directed interventions (work modifications and coaching at work) added to usual care were also promising.4 In other studies, however, several interventions have had no effect on sickness absence,8–11 and one study indicated a negative effect.12
Many of the studies above examine groups already on sick leave. A handful of studies have shown effects of intervening at an earlier stage, where workers with depressive symptoms received occupational therapy,13 CBT combined with work modifications and coaching,14 or workplace interventions inspired by CBT principles combined with problem-solving.15
Physical exercise (PE) has been shown to have positive effects on depressive symptoms,16 but virtually no research on its effects on return to work exists. One research group showed indications that supervised strength training might have positive effects compared with relaxation, while aerobic exercise did not.17 18 However, the risk of bias in these studies was high and none used a non-exercise control group.
Internet-based cognitive behavioural therapy (ICBT) has empirical support as intervention for depression and other mental health conditions.19 ICBT can be individually tailored to match more clinically complex patient profiles,20 and this strategy might also be suitable for integrating non-medical target areas in the intervention, for example modules on return to work and sick leave.
In theory, reducing an individual’s depressive symptoms should be related to increased functioning and motivation, and increase the possibility to find new employment or return to work after sick leave. However, previous research is usually based on small studies and inconclusive. Thus, this area could benefit from evaluation in a larger trial.
Aims of the study
The study aimed to evaluate if individually tailored ICBT, including optional modules targeting work-related problem areas, or PE, with a pure focus on symptom reduction and a generally increased function, would have superior effects compared with treatment as usual (TAU) on employment status in a subgroup of initially unemployed patients, on sick leave in a subgroup of employed patients and on subjective work ability (both subgroups) for patients in primary care suffering from mild to moderate depression.
Methods
Study design
This study is an analysis of primarily two subgroups of patients in a three-armed, randomised controlled trial (RCT) comparing 12 weeks of ICBT, PE and TAU for primary care patients, with assessments at baseline, 3-month (post-treatment) and 12-month follow-up. Previous publications have established superior effects of ICBT and PE compared with TAU for depression,21 22 as well as sleep, stress and psychological functioning.23 Effects on self-rated work ability after 3 months have been reported21 but no other work-related factors. In the present study, two subgroups were created to increase the interpretability of results. In one group patients without any kind of initial employment were evaluated on employment status, and in the second patients with at least part-time employment were evaluated on sick leave. The study was was preregistered at German clinical trials (DRKS00008745).
Patient recruitment and characteristics
Recruitment was done between February 2011 and March 2013 via primary care facilities in six Swedish county councils varying in size and composition. Inclusion criteria in the original study were 10 or above on the Patient Health Questionnaire-9 at an initial screening for depression, age (≥18 years), no severe somatic illness, no primary alcohol or drug use disorder, and no psychiatric diagnosis requiring specialist treatment. Research nurses administered informed consent, baseline questionnaires and the M.I.N.I. Interntional Neuropsychiatric Interview. After all assessments, included patients were randomised by the Karolinska Trial Alliance, an independent clinical trial research organisation where a computer program generated the group allocation, with the size of the randomisation blocks (36 patients) being unknown to the researchers. When the research nurse had entered all assessment data into the study database and confirmed that all inclusion criteria were met, the allocation for the new patient was revealed via the user interface of the database.
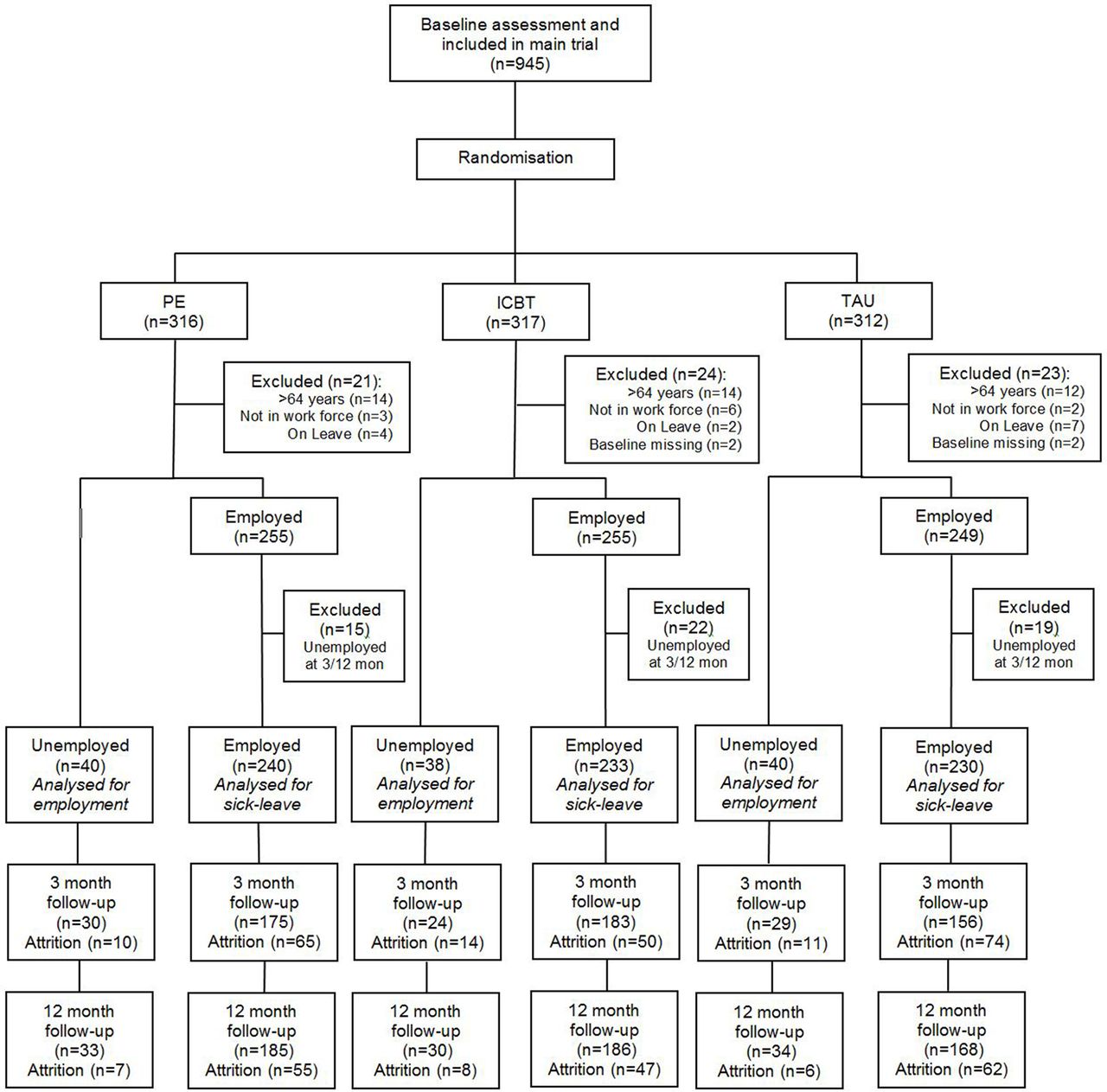
In the current study, with its focus on return to work, some additional exclusion criteria were applied before analysing the data to exclude patients not belonging to the workforce or being voluntarily away from work: being more than 64 years old or being on a disability pension or early pension at baseline, and being on parental leave, leave of absence or on a sabbatical at any time during the trial. Also, patients being analysed on sick leave status who reported being unemployed at either of the follow-ups were excluded from these analyses since their sick leave data were too difficult to interpret in light of their unemployment status. As can be seen in the patient flow chart in figure 1, of the 945 patients included in the original trial, a total of 821 remained for analysis after these additional exclusion criteria were applied; 118 in those initially unemployed subgroup were evaluated on employment status and 703 in those initially employed subgroup were evaluated on sick leave.
{kind=link}
Flow chart of participants (CONSORT). ICBT, internet-based cognitive behavioural therapy; PE, physical exercise; TAU, treatment as usual.
Baseline characteristics of the study sample are shown in table 1. Most of the participants were female (73.4%) and the mean age at inclusion was 41.9 years (SD=11.4; range=18–63). Unemployment rate at baseline was 13.5%. One-third of all participants in the trial were taking antidepressants during the 12-week intervention. Details about the baseline characteristics for the three treatment arms within the two sets of patients are presented in online supplementary appendix B. There were no significant differences between treatment arms except in the employed group, where a larger proportion of patients in PE and fewer in ICBT were studying (χ2 6=13.6; p=0.035) and a higher proportion in the TAU arm were female (χ2=6.8; p=0.033).
Supplementary file 1
Baseline characteristics of the study sample
Primary outcomes
Primary outcomes were based on patients’ self-ratings at baseline and at 3-month and 12-month follow-up. For the subgroup, being at least part-time employed at baseline, long-term full-time or part-time sick leave during at least 1 month was the primary outcome, while at least part-time employment was the primary outcome for patients in the initially unemployed subgroup. Both measures were based on one main question: ‘What is your current employment status?’ One or more of the following answers could be checked: employed, self-employed, leave of absence or parental leave, student, labour-market measure, disability pension, old-age pensioner, unemployed and on long-term sick leave (>1 month). Patients answering ‘Leave of absence or parental leave’, ‘Disability pension’ or ‘Old-age pensioner’ were excluded from all analyses.
To be defined as unemployed, patients should not have any part-time work or study activities. Patients having checked ‘Labor-market measure’ and/or ‘Unemployed’ while not having checked any of the ‘Employed’, ‘Self-employed’ or ‘Student’ options were thus defined as unemployed. All others were defined as employed.
To be defined as being on long-term sick leave, a patient should not be unemployed and should have answered ‘Sick-leave since more than a month’.
Over all three time-points 81 patients (3.1%) did not answer the main question at all. When verifying all answers on the main question by comparing with a range of closely related questions, it was sometimes found that responses contradicted each other, indicating that the patient had misunderstood the main question or missed to check all applicable answers. This indicates that the questions could have been difficult to answer. However, these cases were rather limited. In 13 (0.49%) of all questionnaires, the main question was clearly contradicted by other questions regarding employment status (35, or 2.5%, for sick leave). Internal attrition and contradictory answers were handled in the same way by using the related questions to estimate the value of the primary outcome, as described in online supplementary appendix A.
Supplementary file 2
Secondary outcomes
As a complement to the primary outcome measure of long-term sick leave, the number of average full-time sick days per month was calculated. A range of self-reported questions were used to give an estimation of number of sick days per month, and the measure was then categorised into four ordinal levels: none (0 days/month), low (1–2 days/month), some (3–7 days/month) and high (>8 days/month). Online supplementary appendix A gives a more detailed description of this calculation. Small differences in the questions at different time-points created some systematic differences in how the level of sick days was estimated, which makes this measure inappropriate to use to evaluate main effects over time.
To measure work capacity, the single-item work ability score (WAS) from the Work Ability Index was used. The WAS asks about current self-rated work ability compared with lifetime best and is scored on a Likert scale from 0 (unable to work) to 10 (highest possible work capacity).24
Interventions
Physical exercise
Within the PE arm, patients were randomly allocated to one of three levels of exercise: ‘light’ (yoga or similar), ‘moderate’ (intermediate level aerobics) and ‘vigorous’ (higher intensity aerobics). In this study, all three groups were analysed together. All sessions were 60 min long and the patients were recommended to attend three times per week for 12 weeks. Patients had weekly face-to-face meetings with a qualified personal trainer, and those not attending received a phone call or reminder text messages. In PE, there was no focus on work-related factors, and this intervention is therefore considered as purely symptom-focused. Patients initially unemployed completed on average 9.4 (SD=10.2; median=6.0; range=1–34) out of 36 sessions, and those employed completed 15.2 (SD=10.6; median=13.5; range=1–36) sessions.
Internet-based cognitive behavioural therapy
Patients randomised to ICBT received treatment through a secure website. The treatment was based on self-help text modules, each based on established CBT principles and presenting information on a specific problem area, useful methods to handle it and an online homework report. Patients worked with each module for about a week with brief but active support from a therapist: a clinical psychologist or last-year psychology student under supervision. Risks, specifically suicidal ideation, were monitored continuously. Before treatment, patients received a short phone call from their therapists, who explained the treatment process and helped with technical issues. They also filled in several online questionnaires regarding depression, worry, panic attacks, social anxiety, stress, insomnia, pain and work-related problems. Besides three introductory modules addressing problems related to depressive symptoms, such as inactivity and avoidance behaviours, the subsequent modules were tailored to the patient’s specific clinical profile, mainly based on the areas mentioned above. In total, 34 modules were available and 30 of these were used to individually tailor the treatment.
Of specific importance for the current study, four of the modules aimed at managing problems related to work and sick leave: social insurance agency—participants on sick leave could receive this module, which included information about the sick leave process and homework assignments about initiating better communication with the authority; returning to work—participants on sick leave also could receive this module about the transition of going back to work, including homework assignments about keeping contact with the employer; handling problems at work—participants currently working and reported high levels of stress could receive this module, which included information about a demand-control model of job stress, time management at work and an assignment about handling avoidance behaviours; and finding a new job—participants without employment, or who expressed a wish to find a new job, could receive this module about the job seeking process and homework assignments about scheduling job seeking. In total, patients unemployed at baseline accessed on average 5.8 (SD=4.3; median=5.0; range=1–14) modules out of an expected 13, which was significantly less (t=2.38; p=0.018) than the employed patients accessing 7.9 (SD=4.6; median=9.0; range=1–18) modules. Regarding the four modules related to work and sick leave, 29% of the initially unemployed patients and 18% of the employed accessed at least one.
Treatment as usual
This consisted of primary care standard treatment for depression determined by the patient’s general practitioner. It could for example include antidepressants, counselling with a CBT focus conducted for about 1 hour and group-based interventions. Twenty-five per cent of patients in this group received no recorded treatment.
Statistical analyses
Analyses of return to work after baseline unemployment were made by analysing differences at 3-month and 12-month follow-ups with χ2 tests on observed data, complemented with sensitivity analyses where missing data were assumed to mean ‘still unemployed’. To broaden the evaluation of possible treatment effects on employment status, secondary analyses with χ2 tests were made, including also those who were employed at baseline.
Long-term sick leave and the level of sick days per month were analysed with generalised estimation equations (GEE),25 which like generalised linear modelling adjusts for correlations between repeated measures and handles missing data by estimating a model using all available data from all cases. GEE can be used with both dichotomous (long-term sick leave) and ordinal data (level of sick leave), and handle missing data by including all available data in the estimations. For both measures we built a model with all three time-points and two binary dummy variables to define groups—one for ICBT and one for PE with TAU as the reference group (ie, zero on both dummies)—and evaluated the interaction effects between time and these group-defining dummy variables. Due to small but systematic differences in the estimation of the level of sick leave at different time-points, the main effect of time was not evaluated in that model. Work ability was evaluated with a hierarchical linear mixed model (maximum likelihood), including all three time-points and the two dummy variables above, including their interaction with time. The best model fit was achieved when squared time was added to the models. For sensitivity analyses, aiming to further lower the risk of missing data affecting the results, we added baseline depression, self-rated work ability, gender and age as covariates in the model.
The original power analyses were designed to find a 10% difference in re-employment or returning after long-term sick leave between any two groups, which with a power of 80% at the 5% level would mean 330 patients in each arm. Analyses were performed using SPSS V.22.
Results
Attrition rates
Of the 703 patients included in the analyses of sick leave, 514 (73%) valid measures were obtained at 3-month follow-up and 539 (77%) at 12 months. For the 118 patients included in the employment status analyses, there were 83 (70%) valid measures after 3 months and 97 (82%) after 12 months. Figure 1 presents how the attrition was distributed among the arms. Self-rated work ability was evaluated for the whole sample, and response rates for the WAS for TAU, ICBT and PE were 71%, 81% and 77% at 3 months, and 85%, 87% and 88% at 12 months, respectively. χ2 tests revealed no differences in attrition between arms besides for the sick leave at 3 months, where the groups differed significantly with TAU having an attrition of 33% compared with 27% for PE and 21% for ICBT (χ2(2)=6.77; p=0.033).
Primary outcome for the initially unemployed subgroup: employment status
After 3 months from baseline, 29 (24.6% of all initially unemployed and 34.9% of all those also having a valid measure at 3-month follow-up) of the initially unemployed patients were engaged in at least a part-time employment. After 12 months, the corresponding number had raised to 51 (43.2% of all, and 52.6% of those with valid answers). Table 2 presents the distribution of employed patients among the three arms at the two follow-ups.
Employment status (at least part-time employed), long-term sick leave (full-time or part-time continuously for at least 1 month) and level of average sick days per month
After 3 months, there was a significant difference in the proportion of patients who had gained employment in the three groups (χ2(2)=11.0; p<0.01). Comparing ICBT with TAU revealed a significantly lower proportion of patients in ICBT being employed (χ2(1)=7.7; p<0.01; RR=0.37, 95% CI 0.16 to 0.84), and PE also presented a lower rate of employment compared with TAU (χ2(2)=7.6; p>0.01; RR=0.44, 95% CI 0.23 to 0.87). However, at the 12-month follow-up the three groups did not differ when compared together (χ2(2)=0.98; p=0.61) or when TAU was used as a reference to ICBT (χ2(1)=0.64; p=0.42; RR=1.23, 95% CI 0.72 to 2.13) or to PE (χ2(1)=0.015; p=0.90; RR=0.97, 95% CI 0.69 to 1.57). The sensitivity test, where missing data were interpreted as ‘still unemployed’, presented equivalent results.
To evaluate the interventions’ effect on employment status more broadly, secondary analyses were performed with all patients employed at baseline (n=759). Of those, 21 were unemployed after 3 months and 45 after 1 year, corresponding to 4.1% and 8.3% of the valid observations at each respective time-point, with no significant differences between treatment arms. For all the 877 patients who were within the workforce at baseline, the total number of unemployed patients was 118 at baseline, 75 after 3 months and 91 after 1 year, corresponding to 13.5%, 11.0% and 12.3% of the valid observations at each time-point, with no significant differences between time-points or between the three interventions at each time-point.
Primary outcome for the initially employed group: long-term sick leave
Observed data for long-term sick leave are presented in table 2. Overall, the main effect of time showed an overall decrease of long-term sick leave for all three treatment groups (Wald=29.3; p<0.001). There was no difference in change during the period from baseline to 12-month follow-up, as shown by the lack of time by group interaction between ICBT and TAU (Wald=0.096; p=0.75; RR=0.99, 95% CI 0.39 to 2.46) or between PE and TAU (Wald=0.45; p=0.50; RR=1.4, 95% CI 0.52 to 3.74). The sensitivity test did not change the results.
As seen in table 2, patients in the TAU group had a marked increase in long-term sick leave at 3-month follow-up, but not after 1 year. ICBT and PE showed a similar but less pronounced pattern over time. To explore this, two post-hoc GEE models with only two time-points each were conducted, using the same settings and parameters as the full model with three time-points. As the squared time parameter became redundant it was removed. The first model included only baseline and the 3-month follow-up, and showed a time × group interaction between PE and TAU (Wald=4.84; p=0.028), thus supporting a less steep increase for PE. From 3-month to 12-month follow-up, an opposite pattern was found, showing that the reduction in sick leave for TAU was significantly larger than the reduction for PE (Wald=5.00; p=0.025). No significant time × group interactions were found between ICBT and TAU.
Secondary outcomes (both subgroups)
The average number of sick days per month was estimated and divided in four ordinal levels of sick leave and measured at each time-point, as shown for observed data in table 2. The GEE analyses did not present any significant time by group interactions between ICBT and TAU (Wald=1.41; p=0.23) or between PE and TAU (Wald=0.005; p=0.95). The sensitivity analyses, controlling for missing by adding initial depression, work ability, gender and age as covariates in the model, presented equivalent results.
Table 3 shows that self-rated work ability measured with WAS increased for all three groups. The overall increase over time was significant (t(2185)=5.33; p<0.001), but not the time by group interactions between ICBT and TAU (t(2185)=−0.89; p=0.38) or PE and TAU (t(2185)=−0.85; p=0.40). The sensitivity analysis did not differ from main analyses.
Self-rated work ability (work ability score from the Work Ability Index)
Discussion
All three interventions in this large clinical trial were associated with reductions in long-term (more than a month) sick leave after 1 year, but no differences were found between ICBT, PE and TAU. For those initially unemployed, about half were employed again after 1 year but with no differences between treatments. Self-rated work ability improved during the 1-year period, but no differences between interventions were found. Previously published results from this trial demonstrated that ICBT and PE were superior to TAU in reducing depressive symptoms and problems with psychological functioning and sleep.21–23 However these improvements were not associated with corresponding work-related gains. These findings are in line with some previous intervention studies,8–12 although other studies with corresponding reductions in depression have shown reduced work absenteeism.5–7 A notable strength of the current trial is that it includes a large number of participants, enabling the detection of smaller effects on sick leave and employment. Together, this is a strong indication that symptom reduction of the magnitude seen in this study is not sufficient to affect work-related factors.
Long-term sick leave showed an inverted U-shape trajectory over time, increasing for all groups at the 3-month follow-up and then decreasing again at the 1-year assessment. The group receiving TAU had a significantly sharper initial increase and then a sharper decrease compared with PE, indicating a temporary protecting effect of PE. However, the small number of patients on long-term sick leave, a rather large (borderline significant) baseline difference, and the fact that the secondary outcome measuring level of sick leave did not show the same effect, warrant caution when interpreting these results.
One unexpected finding was that TAU was associated with a larger decrease in unemployment after 3 months. One possible explanation is that patients in ICBT and PE received a clearly defined and time-limited clinical intervention, which might have affected the administration and decisions about their unemployment benefits. For example, the general practitioner responsible for work ability assessments and the employment agency might have wanted to await the effects of ICBT and PE before increasing the claims of finding a new job or making a decision to reduce the unemployment benefits. Regardless of cause, this effect was temporary and the analyses including all patients did not show any differentiating effects on employment status.
Previous research is not conclusive regarding the importance of using interventions with a specific focus on work-related problems and return to work.10–14 26 Our ICBT programme included modules aimed at work-related factors, but this did not lead to the desired outcome. The utilisation of these parts was rather low; roughly one-quarter of all patients accessed at least one work-related module. Even for those who accessed them, they might have been too lightweight, not actively involving the general practitioner, workplace, the social security office or the employment agency. In future studies, internet-based interventions might serve as a platform for stakeholder collaboration. A promising example of this was a recent online intervention teaching problem-solving and targeting work-related negative cognitions (while giving support and feedback to the responsible physician), which reduced return to work time compared with usual care.27
This is the largest RCT to date examining return to work in depressed adults. Additional strengths include the primary care level recruitment and the broad inclusion criteria, making it more representative. The setting and context of this study also constitute a strength since it was conducted in Sweden, while many previous high-quality RCTs have been conducted in the Netherlands, where CBT and occupational health service–workplace cooperation is already a part of TAU.
One main limitation was that measures of sick leave and employment were based on self-report, which may be less accurate than registry data. However, self-reports of sick leave and unemployment have been shown to be highly reliable.28–30 We found that only a small proportion provided indications that the questions were difficult to answer (contradictory answers), that is, 0.49% of employment status and 2.5% for long-term sick leave.
Another limitation is that the subgroups were created after the randomisation process, rather than first creating subgroups and then randomising within these. Freemantle31 note that subgroup analyses might lead to unreliable results. However, this risk is applicable only when an original test of a primary outcome is found non-significant, and later analyses of secondary measures or post-hoc defined subgroups reveal significant differences that are highlighted more than the original test. In our study, subgroups have not been created post-hoc, but out of a necessity to define baseline groups where each outcome measure would make most sense. With employment status, the results were also replicated for the whole group, and overall the number of participants in each intervention group was well balanced within subgroups. One clear limitation was however that the subgroup analysed with employment as primary outcome was rather small and likely underpowered to detect long-term effects. But again secondary analyses comparing changes in employment status for all 877 patients in the workforce at baseline were not suffering from the same problem and did not find any significant differences. Also, the unemployment rate at baseline was 13.5%, which is markedly higher than the 7.5% Swedish average for 2011,32 indicating that the null findings were not due to a low number of cases limiting room for improvement. Another aspect that makes the results more difficult to interpret is the low adherence in the exercise arm and the low usage of the work-related modules in ICBT. Since it has been shown previously that both PE and ICBT in this trial had a superior effect on clinical symptomatology,21–23 the logical conclusion is that even modest adherence to PE was sufficient to improve these outcomes. It is however possible that better adherence would have led to even larger effects on symptoms and everyday function, which in turn could result in work-related benefits. Clinical observations make it likely that the low adherence to work-related modules in ICBT was caused by both the patient and the therapist drifting towards a traditional therapeutic perspective with a primary focus on symptom reduction, resulting in low prioritisation of working life issues. Stressing even more that the work modules were a mandatory part of the individual treatment plan might have increased adherence and thus increased the effects on work-related outcomes.
Other limitations are that the results might be specific to the Swedish context, and that the number of individuals who were invited but declined to participate is unknown. Also, the follow-up period of 12 months might have been too short to find differences in work-related outcomes.
In conclusion, PE and ICBT in primary care are not more effective in reducing sick leave and unemployment compared with TAU. The fact that this large trial, with previously established beneficial, stable effects on clinical symptomatology, did not find any effects on work-related outcomes indicates that symptom reduction is not enough to increase return to work and employment.
Acknowledgments
The authors would like to thank the staff in all six county councils for their tremendous efforts, especially Elisabeth Erwall. We also thank Magnus Backheden and Dr Ingvar Rosendahl for guidance on the statistical analyses.
References
Footnotes
Contributors VK was coinvestigator and took part in the design of the study, implemented the ICBT arm together with NL, coded, analysed and interpreted the data, and wrote the first draft of the majority of the paper. AL helped in interpreting data, wrote the first draft of the introduction, provided critical comments and contributed to writing the paper. MK designed the ICBT programme together with VK, aided in coding and analyses of data, and provided critical comments on the paper. MH aided in coding and analyses of data, and provided critical comments on the paper. CS coordinated the study in one of the regions, aided in data collection and provided critical comments on the paper. ÖE designed the physical exercise intervention, coordinated and monitored it, and provided critical comments on the paper. CL took part in the design of the study and provided critical comments on the paper. NL took part in the design of the study and provided critical comments on the paper. AÖ took part in the design and implementation of the study, interpreted the data and contributed to writing the paper. YF, the principal investigator, designed, implemented and led the entire study, interpreted the data, and contributed to writing the paper.
Funding The Regassa project is funded by Stockholm, Skåne, Kronoberg, Västra Götaland, Blekinge and Västmanlands county councils, REHSAM through the Vårdal Foundation and the Brain Foundation. The funding source had no role in study design, data collection, data analysis, data interpretation or writing of the report. The corresponding author had full access to all data in the study and had final responsibility for the decision to submit for publication.
Competing interests None declared.
Patient consent Obtained.
Ethics approval The regional ethical review board at Karolinska Institutet, Stockholm (Dnr 2010/1779-31/4).
Provenance and peer review Not commissioned; externally peer reviewed.