Article Text

Abstract
Background Individual studies on the relations between ambient air pollution and the risk of stillbirth have provided contradictory results. We conducted a systematic review and meta-analysis to summarise the existing evidence.
Methods We conducted a systematic search of three databases: PubMed, Scopus and Web of Science, from their time of inception to mid-April, 2015. Original studies of any epidemiological design were included. Data from eligible studies were extracted by two investigators. To calculate the summary effect estimates (EE), the random effects model was used with their corresponding 95% CI.
Results 13 studies met the inclusion criteria. Although not reaching statistical significance, all the summary effect estimates for the risk of stillbirth were systematically elevated in relation to mean prenatal exposure to NO2 per 10 ppb (EE=1.066, 95% CI 0.965 to 1.178, n=3), CO per 0.4 ppm (EE=1.025, 95% CI 0.985 to 1.066, n=3), SO2 per 3 ppb (EE=1.022, 95% CI 0.984 to 1.062, n=3,), PM2.5 per 4 μg/m3 (EE=1.021, 95% CI 0.996 to 1.046, n=2) and PM10 per 10 μg/m3 (EE=1.014, 95% CI 0.948 to 1.085, n=2). The effect estimates for SO2, CO, PM10 and O3 were highest for the third trimester exposure. Two time series studies used a lag term of not more than 6 days preceding stillbirth, and both found increased effect estimates for some pollutants.
Conclusions The body of evidence suggests that exposure to ambient air pollution increases the risk of stillbirth. Further studies are needed to strengthen the evidence.
Statistics from Altmetric.com
What this paper adds
Previous reviews on the relations between prenatal exposure to air pollution and the risk of stillbirth were based on only three studies and were inconclusive. Emergence of a substantial number of studies since the last review, called for re-evaluation of the existing evidence.
This systematic review and meta-analysis suggests an elevated risk of stillbirth in relation to air pollution, although further studies are needed to strengthen the evidence.
Policies such as control of vehicular emissions, fuel quality improvement and control of industrial waste emission, should be developed and implemented to reduce the risk of air pollutants.
Introduction
Ambient air pollution is a major environmental health problem in developed and in developing countries,1 and is a major cause of several important diseases including lung cancer,2 acute lower respiratory infections,3 cardiovascular diseases,4 pregnancy outcomes,5 chronic obstructive pulmonary disease COPD6 and asthma.7 The WHO reports that in 20128 around 7 million people died—one in eight of total global deaths was as a result of air pollution exposure, 3.7 million of these were attributed to ambient air pollution due to exposure to particulate matter (PM10).1 This estimate is more than twofold of the previous estimates and suggests that air pollution is now the world's largest single environmental health risk.1
Fetal growth and pregnancy outcome are determined by several factors including maternal nutrition, environmental exposures and heredity. The prenatal stage of life is a very sensitive period such that exposure to harmful substances can have an adverse effect on the developing fetus. The effects of air pollution on fetal growth and pregnancy outcomes have been studied especially in developed countries and the results have been summarised in several reviews.9–12
The WHO reported that 2.6 million stillbirths occurred worldwide in 2009, according to the first comprehensive set of estimates published in a special series of Lancet, 2011. Every day, more than 7200 babies are stillborn.13 Previous studies have identified the important causes of stillbirth as umbilical cord accidents, congenital anomalies, placental abruption, maternal disease (diabetes, HIV, syphilis and hypertension), obesity, primiparity and smoking in pregnancy.14
Two previous reviews have suggested that ambient air pollutant exposure including nitrogen dioxide (NO2), sulfur dioxide (SO2), black carbon, carbon monoxide (CO), polycyclic aromatic hydrocarbons (PAH's) and particulate matter (PM), can also be an important cause of stillbirth, but both concluded that the evidence was weak at the time of conduct. There are also recent reviews indicating that air pollution from secondhand smoke15 and solid fuels16 increases the risk of stillbirth.
The two previous reviews of the effects of ambient air pollution evaluated three studies each, two of which were common to both reviews, with Glinianaia et al17 stating that the evidence available is insufficient to assess a possible association between PM and stillbirth. Lacasana et al18 reported a positive but not consistent association between ambient air pollution and stillbirth; this may be due to an insufficient number of studies available. A recent review by Zhu et al19 evaluated the effect of exposure to PM2.5 on pregnancy outcomes but only included one study on stillbirth. A substantial number of studies have emerged since the conduct of these reviews, and this certainly calls for an evaluation of the evidence to provide insight into causality and identify gaps in knowledge. The objective of the present study was to assess the effect of prenatal ambient air pollution exposure on the risk of stillbirth through systematic review and meta-analysis.
Methods
A systematic search of three databases—PubMed, Scopus and Web of Science—was carried out from their time of inception to mid-April, 2015, using Medical Subject Heading (MeSH) terms without any language restriction. The search terms used are listed in table 1.
Search terms
Two investigators (NS and HAB) independently searched for relevant studies from the databases by first screening the titles of the citations and subsequently reviewing the abstracts of relevant titles. Studies selected after the abstract review were retrieved in full and reviewed with articles selected for inclusion in the study satisfying the following criteria: (1) original articles of any epidemiological design; (2) conducted in a human population; (3) provided effect estimates for the relation between exposure to any outdoor air pollutant and the risk of stillbirth, or reported the occurrence of stillbirth among exposed and unexposed mothers. The reference lists of the included studies were also reviewed to identify additional eligible studies.
Data extraction and study quality appraisal
A data extraction form adapted from our previous review16 was used independently by two investigators (NS and HAB) to extract the relevant information from the studies meeting the inclusion criteria. The information extracted by the two investigators was compared with any differences resolved by repeatedly checking the original articles and through discussion with the third investigator (AKA) adjudicating in situations where there were disagreements. Methodological quality of the included studies was assessed by investigating evidence of selection, information and confounding bias, and evaluation of the case ascertainment protocols. The general quality of the studies was assessed using the Newcastle-Ottawa Scale (NOS).20
Statistical analysis
Owing to differences in study design, geographical settings and different study population, we anticipated the inconsistency in the studies and applied the random effect model in summary effect estimates with their corresponding 95% CI. Heterogeneity of the studies was assessed using the I2 statistic, with a value >50% being deemed to indicate high heterogeneity, 25–50% indicating moderate and <25% indicating low heterogeneity. Individual studies included in the meta-analysis had their effect estimates with different magnitude of air pollutant exposure (except for NO2 and PM10), therefore, before estimating the summary effects the individual effect estimates were converted with a common pollutant concentration such as per 3 ppb increase in SO2, per 0.4 ppm in CO, 4 µg/m3 in PM2.5 and 10 ppb increase in O3 exposure. With regard to the study providing only trimester specific effect estimates, we first combined the three (1st, 2nd and 3rd trimester) estimates using the fixed effects model to get the estimate for the entire pregnancy, and then applied the combined estimate in the overall meta-analysis. Forest plots corresponding to each summary effect estimate were visually assessed. Sensitivity analysis was not conducted due to the small number of studies included in the meta-analysis. Publication bias was assessed by visual inspection of the funnel plots and application of Begg's and Egger's tests. Statistical analyses were performed using Stata V.13.0 (StataCorp LP, College Station, Texas, USA) software.
Results
A total of 13 studies were included in the review. The study selection process is shown in figure 1.

Flowchart of article selection process.
Characteristics of included studies
The characteristics of the included studies are presented in online supplementary table S1.
Supplementary tables
Of the 13 studies, two studies21 ,22 assessed the effects of short-term air pollution exposure with the remaining studies focusing on long-term air pollution exposure. Six studies23–28 assessed maternal exposure to air pollution on a trimester basis.
Of the 11 epidemiological studies with assessment of long-term air pollution exposure, six studies23 ,25–29 employed a cohort design, of which one26 was prospective. Two studies30 ,31 were semiecological, that is, the exposure was assessed at group level and the outcome at individual level, and another two studies were cross-sectional32 ,33 with one study24 applying a case control design. Of the two epidemiological studies with assessment of short-term air pollution exposure, one21 applied a case-crossover design with the hazard period defined as lag day 2 and reference periods selected by matching on the weekday within the same calendar month, and they also used two through 6 days before delivery as lag days. The other short-term air pollution exposure study22 was a time series analysis using Poisson regression and with lag effect of up to 5 days preceding delivery. Regarding the geographical location of the included studies, five studies were conducted in the USA, one in Latin America, three in East Asia, two in Europe, one in Russia and one in the UK. Seven of the included studies were published after the year 2005.
Eleven21–31 of the included studies relied on routine air monitoring data in their respective study areas in estimating maternal air pollution exposure. Landgren33 categorised each exposure in two ways, (1) above and below the mean exposure value (SO2: 8.0 µg/g, CH: 6.6 µg/g and NO: 14.7 µg/g) of all the included municipalities and (2) the municipality with the highest exposure level was compared with all other municipalities. Vassilev et al32 used statewide combined modelled average concentrations for each census tract and categorised exposures into low (0.040–0.268 mg/m3), medium (0.269–0.610 mg/m3) and high exposure (0.611–2.830 mg/m3) level with low exposure serving as the reference in the analysis. The included studies measured 13 pollutants including SO2, NO2, CO, particles (PM2.5, PM10, SPM), O3, NO, POM, NOx, hydrocarbon (CH), black smoke, which was taken as equivalent to PM4 in the study that measured this pollutant,25 and suspended solids.
Of the 11 studies relying on air monitoring station data, seven studies21 ,23–28 and that by Vassilev et al32 assigned exposures to mothers based on their residential addresses at the time of delivery. Regarding the studies conducted by Faiz et al21 ,23 and DeFranco et al,27 mothers had to live within a 10 km radius of the closest monitoring station; and Green et al28 used 20 km radius for PM2.5, O3, SO2 and 5 km radius for CO and NO2 to be included in the studies. Whereas Hwang et al24 applied a 25 km radius. The exposure assignments in the studies by Kim et al,26 Pearce et al25 and Vassilev et al32 were not based on any fixed radius. The two ecological studies30 ,31 used annual mean concentrations of the pollutants studied to assign exposures. Dimitriev29 used monthly concentration of air pollutants in the study areas.
Six studies21 ,23 ,24 ,27 ,28 ,32 used a stillbirth cut-off point of >20 weeks of gestation, with three studies22 ,25 ,30 using a cut-off of >28 weeks of gestation. Landgren33 and Sakai31 did not provide a case definition in their reports. DeFranco et al27 ascertained stillbirth by using both, last menstrual period (LMP) and ultrasound examination methods, whereas two other studies25 ,26 mostly used the LMP method but also used fetal ultrasound examination if there was either uncertainty about the LMP date or discordance between the two estimates. Two studies23 ,28 used the LMP method only, with Hwang et al24 applying ultrasound examination. The type of stillbirth studied was not mentioned in any of the included studies except the study by Pereira et al,22 which identified the stillbirths as intrauterine mortality, which we assume to be antepartum stillbirth. The source of data on stillbirth was obtained from fetal death certificates in five studies,21–23 ,32 ,33 birth registry or vital statistics in five studies24 ,27 ,28 ,30 ,31 and hospital records in two studies.25 ,26 Dimitriev29 did not provide any information on how the stillbirths were ascertained.
Methodological quality of the included studies
Selection bias
Selection bias was very minimal in the included studies as most of the studies collected data from fetal death certificates or birth registries and are likely to have represented their source populations with high response rate also reported. The prospective cohort study,26 however, only included pregnant women who visited the hospital for prenatal care, excluding mothers with missing values for residential address and sociodemographic risk factors. Few studies25 ,28 ,32 excluded mothers without gestational age information and census tract coding (8%) from the analysis.
Information bias
There was evidence of potential information bias in all the included studies due to the reliance on proximity of maternal homes to the nearest air pollution monitoring station,21–31 and use of emission measurement and meteorological data32 ,33 in assessing exposure. Factors such as mother's mobility, change of residence during pregnancy, occupation of mother and air exchange were not considered, and this may lead to a decrease in the accuracy of the exposure assessment and introduce a non-differential misclassification that might lead to an underestimation of the effects of air pollution. Also, the exposure source was not reported by the studies other than those by Hwang et al,24 Pearce et al,25 Vassilev et al32 and Sakai.31 For the outcome measurement, the true dates of fetal death were unknown, hence an estimated time using date of delivery was recorded on the fetal death certificate and this may introduce bias. This was observed in the study by Faiz et al,21 ,23 Hwang et al,24 Kim et al,26 Green et al,28 Bobak and Leon,30 and Vassilev et al.32
Control of confounding
Any determinant of the risk of stillbirth could be considered as a potential confounder in cohort, case–control and cross-sectional studies. The case-crossover study and time-series analyses eliminate any confounding related to individual characteristics and environmental exposures that are linked to the studied air pollutant. Most studies adjusted for the characteristics of the mother, such as age and family characteristics, at an individual level. Some of the studies applied control of confounding at group levels.30 When estimating the effect of an individual air pollutant, exposure to other air pollutants is a potential confounder. Only five studies fitted more than one air pollutant into the multivariate model, that is, applied multipollutant rather than single pollutant models.21 ,22 ,24 ,28 ,30
Regarding the ecological studies, Bobak and Leon30 adjusted for several socioeconomic characteristics, which were obtained from the Czech Statistical office, at the district level; whereas Sakai31 did not control for confounding. In the time series analysis, Pereira et al22 adjusted for season and weather. Faiz et al21 conducted a case-crossover study where they controlled for mean temperature of the corresponding lag days. Of the nine long-term air pollution exposure studies, Dimitriev29 did not control for any confounding and the confounding control was considered inadequate in one study,33 as the author only adjusted for year of birth, maternal age and parity. Confounding control was considered adequate in the remaining studies.23–28 ,32 These studies adjusted for a range of confounders including maternal age, race, education, socioeconomic status, season or month of conception, parity, infant sex, prenatal care and lifestyle characteristics. Hwang et al24 and Kim et al26 further controlled for gestational age and maternal anthropometry, respectively. Vassilev et al32 used separate Mantel-Haenzel OR analysis for potential confounding factors and few factors were controlled in the final logistic regression model, this approach can also be deemed as adequate control of confounding factors.
By applying the NOS scale, three studies23 ,24 ,28 were rated as very high quality (case–control/cohort—8 or more stars) and one study26 was rated as high quality (cohort study—7 stars). The Newcastle-Ottawa-Scores for all the studies included in the meta-analyses are presented in the online supplementary table S2.
Findings of included studies and summary effect estimates
Summary effect estimates are presented in table 2 and the corresponding forest plot in figure 2.
Summary effect estimates for the relation between ambient air pollution exposure and the risk of stillbirth

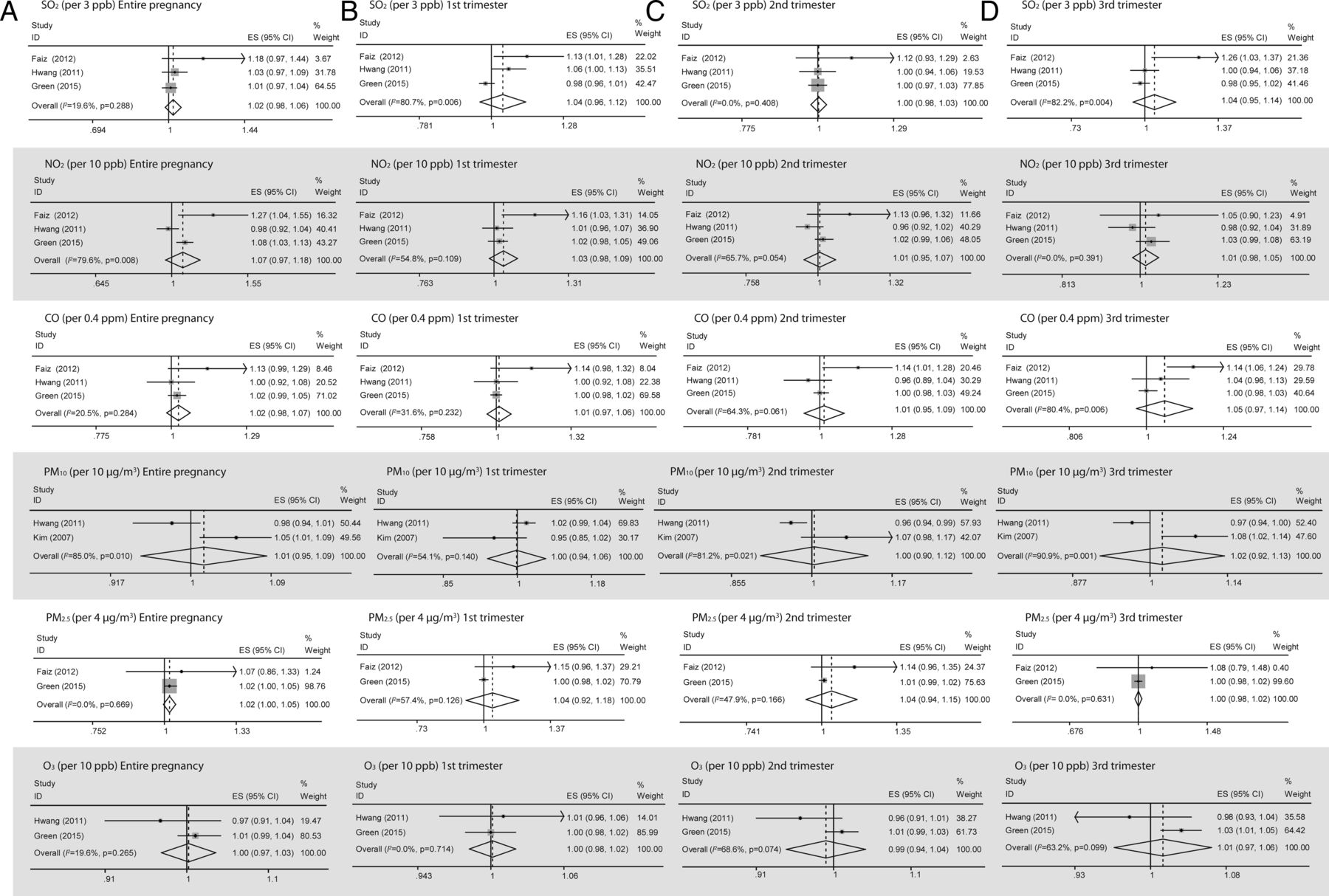
Forest plot showing the effect of ambient air pollutants on stillbirth. ES, effect size; weights are from random effects analysis.
Three studies23 ,24 ,28 provided estimates for the relation of SO2 exposure (per 3 ppb, 1 ppb and 10 ppb increase in mean concentration) to stillbirth for the entire pregnancy period. The summary-effect estimate (EE) per 3 ppb increase in SO2 exposure in the random effects model was 1.022 (95% CI 0.984 to 1.062), with low heterogeneity between the studies observed (I2=19.6%). The case-crossover study21 reported increased risk of stillbirth with IQR (4.7 ppb) increase in mean SO2 exposure 2 days before delivery, and also found similar associations on all the lag days; whereas, another time series study22 reported marginal association between daily counts of intrauterine mortality and SO2 concentration on the same day as delivery. One of the ecological studies31 also found significant positive correlation between spontaneous fetal death rate and SO2 concentration. However, Landgren33 and other ecological study (per 50 µg/m3 increase in annual mean concentration of SO2),30 however, did not find any association, even after adjustment with other pollutants SPM and NOx.
Three studies23 ,24 ,28 provided estimates for the relation of both NO2 and CO exposure for the entire pregnancy period, with the summary EE in the random effects model found to be 1.066 (95% CI 0.965 to 1.178) per 10 ppb increase in mean NO2 concentration and 1.025 (95% CI 0.985 to 1.066) per 0.4 ppm increase in mean CO concentration, respectively. Evidence of high heterogeneity was observed in the NO2 analysis (I2=79.6%). The case-crossover21 studies reported increased risk of stillbirth with IQR increase of NO2 (16.4 ppb) and CO (0.54 ppm) in mean concentration, respectively, 2 days before delivery and also found similar associations on all the lag days. The time-series study22 reported strong significant dose–response relationship between daily counts of intrauterine mortality with NO2 concentration, and marginal association with CO concentration at 5 days and 3 days before delivery, respectively. The findings of CO exposure with stillbirth were, however, less consistent. Sakai31 also found a statistically significant positive correlation between NO2 concentration and spontaneous fetal death rate. Pereira et al22 also developed an overall index of air pollution (combination of NO2, SO2, CO) and found a very robust significant association with dose–response relationship, whereas Faiz et al21 used two pollutant models on lag day 2 but found estimates similar to those of the single pollutant models. Green et al28 adjusted PM2.5 or ozone with NO2 and the associations were unaffected.
Two studies24 ,26 provided estimates for the relation of stillbirth per 10 µg/m3increase in average PM10 concentration during the entire pregnancy duration to the summary EE in the random effects model found to be 1.014 (95% CI 0.948 to 1.085). Evidence of high heterogeneity was noted in the analysis (I2=85.0%). The time series study22 did not find any statistically significant associations.
Two studies23 ,28 provided estimates for the relation of stillbirth per 4 µg/m3 increase in average PM2.5 concentration during the entire pregnancy duration to the summary EE in the random effects model found to be 1.021 (95% CI 0.996 to 1.046). No heterogeneity was noted in the analysis (I2=0.0%). DeFranco et al27 found non-significant 21% (OR: 1.21, 95% CI 0.96 to 1.53) increased risk in stillbirth with high PM2.5 (15.67 µg/m3) exposure during the entire pregnancy.
Two studies24 ,28 provided estimates for the relation of stillbirth per 10 ppb increase in average O3 concentration during the entire pregnancy duration to the summary EE in the random effects model found to be 1.002 (95% CI 0.971 to 1.034). Evidence of low heterogeneity was noted in the analysis (I2=19.6%). The time series study22 evaluated the relation between O3 exposure and stillbirth, and found no association.
Four studies23 ,24 ,26 ,28 provided trimester-specific estimates for the relation of stillbirth risk to six pollutants (SO2, NO2, CO, PM10, PM2.5, O3). With the exception of SO2 exposure during the second trimester, NO2 and PM2.5 exposure during the third trimester and O3 exposure during the first trimester, we observed evidence of moderate to substantial heterogeneity in most of the analysis. In the random effect model, almost all these pollutants (per 3 ppb SO2, 10 ppb NO2, 0.4 ppm CO, 10 µg/m3 PM10, 4 µg/m3 PM2.5 and 10 ppb O3 increase in mean concentration) showed increased risk in each trimester except SO2 and NO2 exposure in the second trimester, PM10 and O3 exposure in the first and second trimester and PM2.5 exposure in the third trimester. For SO2, CO, PM10 and O3, third trimester exposure appears to pose the highest risk whereas for NO2 and PM2.5, first trimester exposure posed the highest risk. The summary EE per 10 µg/m3 increase in PM10 exposure showed an increasing trend whereas for PM2.5 per 4 µg/m3 increase in concentration, a decreasing trend was observed. Regarding SO2, NO2, CO and O3, the trend was inconsistent with the second trimester summary estimates, being the lowest for SO2, NO2, O3 and first trimester for the CO exposure. Faiz et al21 found a non-significant small increased risk of stillbirth with IQR increase in the mean PM2.5 concentration in their time series analysis on all the lag days. Whereas DeFranco et al27 found significant 42% (OR 1.42, 95% CI 1.06 to 1.91) increased risk in stillbirth with high PM2.5 (16.22 µg/m3) exposure only in the third trimester. Hwang et al24 evaluated increased risk of stillbirth in association with SO2 per 1 ppb and PM10 per 10 µg/m3 increase during the first and second months of pregnancy, and was stable after adjustment for O3 and either CO or NO2 in multipollutant models. Green et al28 found robust association with third trimester O3 exposure after addition of PM2.5 and NO2.
Dimitriev29 compared the occurrence of stillbirth in good and worse ecological areas assessed on the basis of monthly concentration of selected pollutants (suspended solids, SO2, CO, NO2), and reported risk of stillbirth as 6.63 and 11.03 per 1000 births, respectively. The estimated risk ratio showed a 65% (RR 1.650, 95% CI 1.136 to 2.397) increased risk of stillbirth among mothers resident in polluted ecological areas.
Two studies31 ,33 that investigated the relation of NO exposure to stillbirth also found no association. The association between stillbirth risk and per 10 µg/m3 relating average weekly black smoke (equivalent to PM4) exposure was evaluated by Pearce et al,25 but did not find any significant association during pregnancy. Bobak and Leon30 evaluated the effects of SPM and NOx (per 50 µg/m3 increase in concentration), and found no significant association in the single pollutant model nor after adjustment with all pollutant (SPM, SO2, NOx) models. Vassilev et al32 investigated POM exposure and, using low exposure as the reference category, found statistically significant increased risk of stillbirth with medium and high exposure (ORs of 1.21 (95% CI 1.04 to 1.40) and 1.19 (95% CI 1.02 to 1.39), respectively). The effect of CH was investigated by Landgren,33 but no association was found between stillbirth and levels of CH concentration in Swedish municipalities.
Evaluation of publication bias
Figure 3 presents the funnel plots for all the study specific effect estimates used to calculate the summary effect estimates. Online supplementary table S3 presents results from the Begg's and Egger's tests. There was no indication of publication bias present, although these results should be interpreted with caution because they were based on two or three study-specific effect estimates only.

{kind=link}
{kind=link}
{kind=link}
Funnel plot with pseudo 95% confidence limits for the relation between ambient air pollutants and stillbirth.
Discussion
Our systematic review and meta-analysis provided evidence that prenatal exposure to air pollution increases the risk of stillbirth. The summary effect estimates from the random effects models were systematically elevated, although they did not reach statistical significance. Per 10 ppb NO2, 0.4 ppm CO, 3 ppb SO2, 4 µg/m3 PM2.5 and 10 µg/m3 PM10, increase in mean exposure during the entire pregnancy duration, respectively, resulted in a 6.6% (EE=1.066, 95% CI 0.965 to 1.178), 2.5% (EE=1.025, 95% CI 0.985 to 1.066), 2.2% (EE=1.022, 95% CI 0.984 to 1.062), 2.1% (EE=1.021, 95% CI 0.996 to 1.046) and 1.4% (EE=1.014, 95% CI 0.948 to 1.085) increased risk of stillbirth. The point estimates for the third trimester were slightly elevated for SO2, CO, PM10 and O3 consistently, with a hypothesis of a susceptible time window for the adverse effects, although the differences were not statistically significant. Two time series studies used lag day not more than 6 days preceding stillbirth and both found increased risk with certain pollutants.
Validity of results
We included all the studies identified in an extensive systematic search, so missing of important epidemiological studies is less likely to have happened. A significant number of studies have emerged since the last reviews; hence the critical assessment of the evidence is timely. Even though our review contains eight more studies and much more information than the previous reviews, we found a very limited number of estimates for each of the pollutants, and only five studies made attempts to adjust for other air pollutants when presenting effect estimates of each air pollutant. Therefore, we could not include all of the studies in the meta-analyses, and the reliability on the summary effect estimates is further compromised. However, the existing evidence is suggestive of causality for air pollution and stillbirth without precise identification of the timing of exposure. With the limited studies on the relevant topic, our review suggests strong priorities for future research. The visual inspection of the funnel plots and the statistical assessment did not indicate publication bias.
Biological plausibility
Fetuses are more affected by a variety of environmental toxicants because of differential exposure and physiological immaturity.34 The biological mechanisms by which exposure to ambient air pollutants leads to fetal death is not very clear. Faiz et al21 suggested the direct crossing of air pollutants across the placenta, causing irreversible damage to the dividing cells of the growing fetus and triggering hypoxic damage or immune-mediated injury during critical periods of development, as a possible mechanism.
Of all the pollutants, only the mechanism of the toxic effects of CO on the fetus is well established.17 CO reduces oxygen-carrying capacity of maternal haemoglobin that could seriously affect oxygen delivery to fetal circulation.35 Sangalli et al36 revealed that CO crosses the placental barrier and haemoglobin on fetal blood has greater affinity for binding CO than that in an adult; O2 delivery to fetal tissues is further compromised.37 Moreover, fetal elimination of carbon monoxide is slower than in the mother.38 There is also a significant dose-dependent relationship between CO and COHb, and a developing fetus can be deprived of adequate oxygenation due to high levels of COHb, which may even lead to fetal death.22
Maternal exposures to particulate (PM) air pollutants during pregnancy can result in increased concentration of DNA adducts or may lower the efficiency of the transplacental function, resulting in decreased fetal health leading to stillbirth.39 ,40
There is evidence that the presence of air pollution increases blood viscosity and plasma fibrinogen relates to coagulation; these haematological factors might have an influence on blood perfusion of the placenta, which could also lead to impair fetal health.41–43
Synthesis with previous knowledge
In the meta-analysis, we observed a 1.4% (EE 1.014, 95% CI 0.948 to 1.085) increased risk of stillbirth with 10 µg/m3 increase in PM10 exposure during the entire duration of pregnancy, albeit statistically but not significantly. Pereira et al22 also did not find any statistically significant association in their time series study. Glinianaia et al17 reported little evidence of association between exposure to PM and stillbirth risk, and thus describes it as insufficient to assess a possible association between PM and stillbirth.
For PM2.5, Zhu et al indicated that there was no evidence of statistically significant effect (OR: 1.18, 95% CI 0.69 to 2.04) on stillbirth with an increase of 10 µg/m3; this result is consistent with our review, which reveals (EE 1.021, 95% CI 0.996 to 1.046) with an increase of 4 µg/m3. However, in our meta-analysis, we also found a 4.2% (EE 1.042, 95% CI 0.920 to 1.180) and 4.0% (EE 1.040, 95% CI 0.940 to 1.152) increase per 4 µg/m3, in the first and second trimester, respectively.
We also observed a small and statistically non-significant increased risk of stillbirth with SO2 2.2% (EE 1.022, 95% CI 0.984 to 1.062) and CO 2.5% (EE 1.025, 95% CI 0.985 to 1.066) exposure for the entire pregnancy period in the meta-analysis. The short-term air pollution studies on these relationships21 and one of the ecological studies31 also reported an increased risk of stillbirth related to SO2 and CO exposure. The findings of CO exposure with stillbirth was, however, less consistent.
Lacasana et al18 stated that SO2 and CO also showed some, though less consistent, relationship with intrauterine mortality. In our review, we found that there is an increased risk of stillbirth associated with increased ambient concentrations of sulfur dioxide in early pregnancy, with pooled effect estimates of 4.0% (EE 1.040, 95% CI 0.962 to 1.125). Also, we found the highest pooled estimate of 5.2% (EE 1.052, 95% CI 0.973 to 1.138) for carbon monoxide in the last trimester.
For NO2, we observed a higher increase risk of stillbirth of 6.6% (EE 1.066, 95% CI 0.965 to 1.178) for the entire pregnancy. This finding is consistent with the study by Lacasana et al,18 which reported an increased risk of stillbirth with exposure to NO2.
Most of the pollutants in polluted ambient air, such as PM and CO, are also present in indoor air polluted by smoking and solid fuel combustion, although the concentrations are lower. Leonardi-Bee et al15 conducted a meta-analysis of studies on the effects of secondhand smoking on the risk of stillbirth, presenting a 23% risk increase (EE 1.23, 95% CI 1.09 to 1.38). Amegah et al16 synthesised the effect of solid fuels showing an effect estimate of 29% for stillbirth. These findings are consistent with the present pollutant-specific summary effect estimates and thus strengthen the hypothesis that ambient air pollution increases the risk of stillbirth.
Conclusion, recommendations and implications for future research
Our results provide suggestive evidence that ambient air pollution is a risk factor for stillbirth. Pregnant women should be aware of the potential adverse effects of ambient air pollution, although the prevention against exposure to air pollutants generally requires more action by the government than by the individual. The healthcare sector can create awareness and engage other sectors contributing to ambient air pollution (such as the housing sector, transportation sector, industries and the energy sector), to develop and implement policies such as control of vehicular emissions, fuel quality improvement and control of industrial waste emission, to reduce the risk of air pollutants.
Most of the studies reviewed used data from monitoring stations to assess maternal exposure levels. Future studies should integrate the use of personal monitoring methods and also consider the activity of mothers, change in residence, air exchange, mother's occupation and outdoor activities of the mothers. The pregnant women should also be monitored if possible from the first month of pregnancy in order to ascertain the exact period of the effect.
Acknowledgments
The authors thank Svetlana Filatova, Medical Research Center Oulu, Oulu University Hospital and University of Oulu, Finland, for helping with the translation of the Russian study included in the review.
References
Supplementary materials
Press release
Files in this Data Supplement:
Footnotes
Contributors JJKJ conceived the study and designed it with AKA. NS and HAB conducted the search and screened the articles, and contributed to the statistical analyses. AKA contributed to the evaluation of the manuscript, writing of the manuscript, statistical analyses and interpretation of the results. All the authors revised the manuscript for important intellectual content, and the final version has been approved by all the authors. JJKJ takes responsibility for the integrity of the article.
Funding The University of Oulu strategic funds.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement Data needed for repeating the meta-analyses are presented in tables. Additional information on the methods or preliminary data can be requested from the corresponding author.