Article Text

Abstract
The burden of disabling musculoskeletal pain and injuries (musculoskeletal disorders, MSDs) arising from work-related causes in many workplaces remains substantial. There is little consensus on the most appropriate interventions for MSDs. Our objective was to update a systematic review of workplace-based interventions for preventing and managing upper extremity MSD (UEMSD). We followed a systematic review process developed by the Institute for Work & Health and an adapted best evidence synthesis. 6 electronic databases were searched (January 2008 until April 2013 inclusive) yielding 9909 non-duplicate references. 26 high-quality and medium-quality studies relevant to our research question were combined with 35 from the original review to synthesise the evidence on 30 different intervention categories. There was strong evidence for one intervention category, resistance training, leading to the recommendation: Implementing a workplace-based resistance training exercise programme can help prevent and manage UEMSD and symptoms. The synthesis also revealed moderate evidence for stretching programmes, mouse use feedback and forearm supports in preventing UEMSD or symptoms. There was also moderate evidence for no benefit for EMG biofeedback, job stress management training, and office workstation adjustment for UEMSD and symptoms. Messages are proposed for both these and other intervention categories.
- Upper Extremity
- Prevention
- Workplace
- Review
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Introduction
Work-related musculoskeletal disorders (MSDs) are a constellation of painful disorders of muscles, tendons, joints and nerves which can affect all body parts, although the neck, upper limb and back are the most common areas.1 ,2 Overall work-related MSDs account for 29% of all US workplace injuries.2 In Canada, MSDs account for between 40% and 60% of lost-time claims since 2000.3–6 In Canada and the USA, upper extremity MSDs (UEMSDs) and low back pain are the leading causes of disabling work-related injuries.2–6 In Europe, UEMSDs and low back pain are considered to be an increasing and significant health problem, making up approximately 39% of occupational diseases.1 Recent attention and studies suggest that MSDs are considered a growing problem in the developing world as well.7–12
It has been estimated that work-related UEMSDs and low back pain costs are between 0.5% and 2% of the EU's gross national product.1 UEMSDs are significant causes of disability claims cost, and lost productivity in many economic sectors worldwide.7 ,13–16 In summary, UEMSDs are prevalent and costly demanding focused prevention campaigns.
The peer-reviewed literature about workplace prevention describes a variety of interventions that have been implemented and evaluated.17–25 However, few studies show sustainable positive effects on symptom, claim and disability outcomes. Overall, the studies and reviews to date reveal that there is no ‘magic bullet’ to deal with the significant burden of UEMSD.18–23 Consequently, systematic reviews, to date, have not been able to provide strong guidance for practice.
Despite the lack of guidance from literature, Occupational Health and Safety (OHS) practitioners have created workplace-based interventions to reduce UEMSD burden based on their training, knowledge and experiences. The challenges of conducting well-designed, rigorous evaluations have been a barrier to building the strong scientific evidence base necessary to guide practice.26–29 Poorly implemented interventions that could not be expected to lead to sustainable change in outcomes studied are another barrier. Kristensen26 has referred to this as programme failure versus theory failure. The implementation aspects of workplace-based interventions have been explored30–33 revealing the importance of intervention intensity, implementation, as well as scientific rigour.
A previous review Kennedy et al23 found moderate evidence for arm supports and limited evidence for ergonomics training plus workstation adjustments, new chair and rest breaks. Levels of evidence for interventions associated with ‘no effect’ were: there was also strong evidence for no effect of workstation adjustment alone; moderate evidence of no effect for biofeedback training and job stress management training; and limited evidence of no effect for cognitive behavioural training. The overall conclusion of the review was that it was not possible to make recommendations to practitioners about how to prevent or manage UEMSDs.
Therefore, the study objective was to systematically review the literature to synthesise the evidence on the effectiveness of workplace-based interventions focused on UEMSDs. This is the first update of the earlier review.23 Stakeholders from Ontario, Canada, were engaged iteratively throughout, particularly in refining evidence synthesis categories and developing practical messages based on the synthesis to support evidence-based practice.
Methods
The systematic review followed the six review steps developed by the Institute for Work & Health (IWH) for OHS prevention reviews:34 (1) question development, (2) literature search, (3) relevance/inclusion screen, (4) quality appraisal, (5) data extraction and (6) synthesis. The review team participated in all review steps. Eleven researchers from Canada, Europe and the USA with expertise/experience in conducting MSD studies or systematic reviews comprised the team.
The IWH Systematic Review programme follows an integrated stakeholder engagement model during reviews.35 This results in stakeholders providing feedback throughout the review process. For this review, the stakeholders were all from Ontario and included ergonomists, policymakers, labour, employers, business and disability management consultants.
Question development
The review team and stakeholders participated in a meeting to discuss the review update research question, and proposed search terms. The review team and stakeholders retained the original review question and search terms for this update.
Literature search
Six electronic databases were searched: MEDLINE, EMBASE, Cumulative Index to Nursing & Allied Health Literature (CINAHL), Canadian Centre for OHS's CCINFO web, Cochrane Library, and Ergonomic Abstracts from 2008 to April 2013. The databases were chosen based on those that yielded references in the original review and were still available. Additional databases were added to the search based on feedback from stakeholders. The search strategy was guided by the original review search and designed to be inclusive, using terms from three broad areas: work setting terms, intervention terms and health/claim outcome terms. The terms within the work setting and intervention categories were combined using a Boolean OR operator and the three main categories were then combined using a Boolean AND operator.
The search terms and database languages differ significantly; therefore, the search terms were customised. For the most part, the titles, abstracts or subject headings were searched for keywords.
In addition to the database searches, the reference lists of all papers selected for review were manually searched. The team also contacted experts in the field and sought out references that were prepublication to ensure a comprehensive search.
References were loaded into commercially available review software (DistillerSR),36 which was also used for all remaining review steps. DistillerSR is an online application designed specifically for the screening, quality appraisal and data extraction phases of a systematic review.
Relevance screen
The review team devised five screening criteria to exclude articles not relevant to our review question: (1) non-English or commentary/editorial; (2) study was not in a work setting; (3) no OHS intervention was evaluated; (4) no comparison group was used; and (5) study outcomes did not include upper extremity musculoskeletal symptoms, signs, disorders, injuries, claims or lost time. The review team decided to exclude non-English references based on low yields in the previous review and other preventions reviews. We note that the non-English articles were excluded due to other criteria in this review.
First, titles and abstracts of references were screened by a single reviewer. To limit the possibility of bias, a quality control (QC) step was implemented. A QC reviewer independently assessed a randomly chosen set of 446 titles and abstracts (approximately 5% of references from the search). Comparing the QC reviewer responses directly to review team responses, 92 conflicts (20%) were found. However, only 6 (1.3%) were conflicts where the review team excluded references and the QC reviewer included them. Consequently, the review team is confident that the titles and abstracts were screened reflecting inclusion and exclusion requirements. The small (1.3%) number of discrepancies suggests that reviewers had a similar understanding and application of the screening criteria.
Second, the remaining full-text articles were screened using the same criteria, with two reviewers independently reviewing and coming to consensus. When consensus could not be reached, a third reviewer was consulted. Third, relevance criteria were revisited in each subsequent review step and articles were excluded if the two reviewers were in consensus.
Quality appraisal
Relevant articles were appraised for methodological quality. Since this is a review update,23 the same criteria and scoring algorithm were used. Quality was assessed using 16 methodological criteria within the following broad headings: Design and Objectives, Level of Recruitment, Intervention Characteristics, Intervention Intensity, Outcomes, and Analysis.
Methodological quality scores for each article were based on a weighted sum score of 16 quality criteria (with a maximum score of 41). The weighting values assigned to the 16 criteria ranged from ‘somewhat important’ (1) to ‘very important’ (3). Each article received a quality ranking score by dividing the weighted score by 41 and then multiplying by 100. The quality ranking was used to group articles into three categories: high (>85%), medium (50–85%) and low (<50%) quality.23
Each article was independently assessed by two reviewers, who were required to reach consensus on all criteria. Where consensus could not be achieved, a third reviewer was consulted. Team members did not review articles they had consulted on, authored or co-authored.
The quality appraisal represents an assessment on: internal validity, external validity and statistical validity.37 A higher quality score increases the team's confidence that an effect was an intervention consequence versus the effect(s) of other workplace or external environment factors. Therefore, data extraction and evidence synthesis were only completed on high-quality and medium-quality studies.
Data extraction
Standardised forms based on the previous review were used. Extracted data were used to create summary tables sorted by intervention category and used for evidence synthesis. Data were extracted independently by pairs of reviewers. Again, reviewer pairs were rotated to reduce bias. Team members did not review articles they consulted on, authored or co-authored. Any conflicts between reviewers were resolved by discussion. Stakeholders were consulted to determine relevant intervention categories.
Evidence synthesis
The evidence synthesis approach34 ,38 considers the quality, quantity and consistency in the body of evidence (see table 1).
Best evidence synthesis algorithm/algorithm for messages
First, the intervention categories created in the data summary tables were examined by the entire team. Once consensus was reached on the categories, the team moved to summarising the evidence per category. Owing to the heterogeneity across outcome measures, study designs and reported data, we chose not to calculate a pooled effect estimate. To determine individual study intervention effects, the following rules were applied: an intervention with a positive and no negative results was classified as positive effect, an intervention with both positive and no effect was also classified as positive effect, an intervention with only no effects was classified as no effect, an intervention with any negative effect was classified as negative effect. The direction of the intervention effect was considered along with study quality rating and number of studies to determine the level of evidence for each intervention category (see table 1).
To reach a strong level of evidence, there had to be at least three high-quality studies that had that same direction of effect or at least 75% of all studies within the intervention category had to have the same direction of effect.
To generate practical messages, an algorithm developed by IWH along with OHS stakeholders was followed.39 A strong level of evidence leads to ‘recommendations’. A moderate level of evidence leads to ‘practice considerations’. For all evidence levels below moderate, the consistent message is: ‘Not enough evidence from the scientific literature to guide current policies/practices’. This does not mean that the interventions with limited, mixed or insufficient evidence may not be effective; only that there is not enough scientific evidence to draw conclusions.
Results
Literature search
The search (covering 2008–April 2013) identified 9908 references once results from EMBASE, MEDLINE, Ergonomic Abstracts, CINAHL, Cochrane Library, CCInfoWeb were combined and duplicates removed. One additional paper was identified by the research team that was not captured by the search, resulting in a total of 9909 references (figure 1).

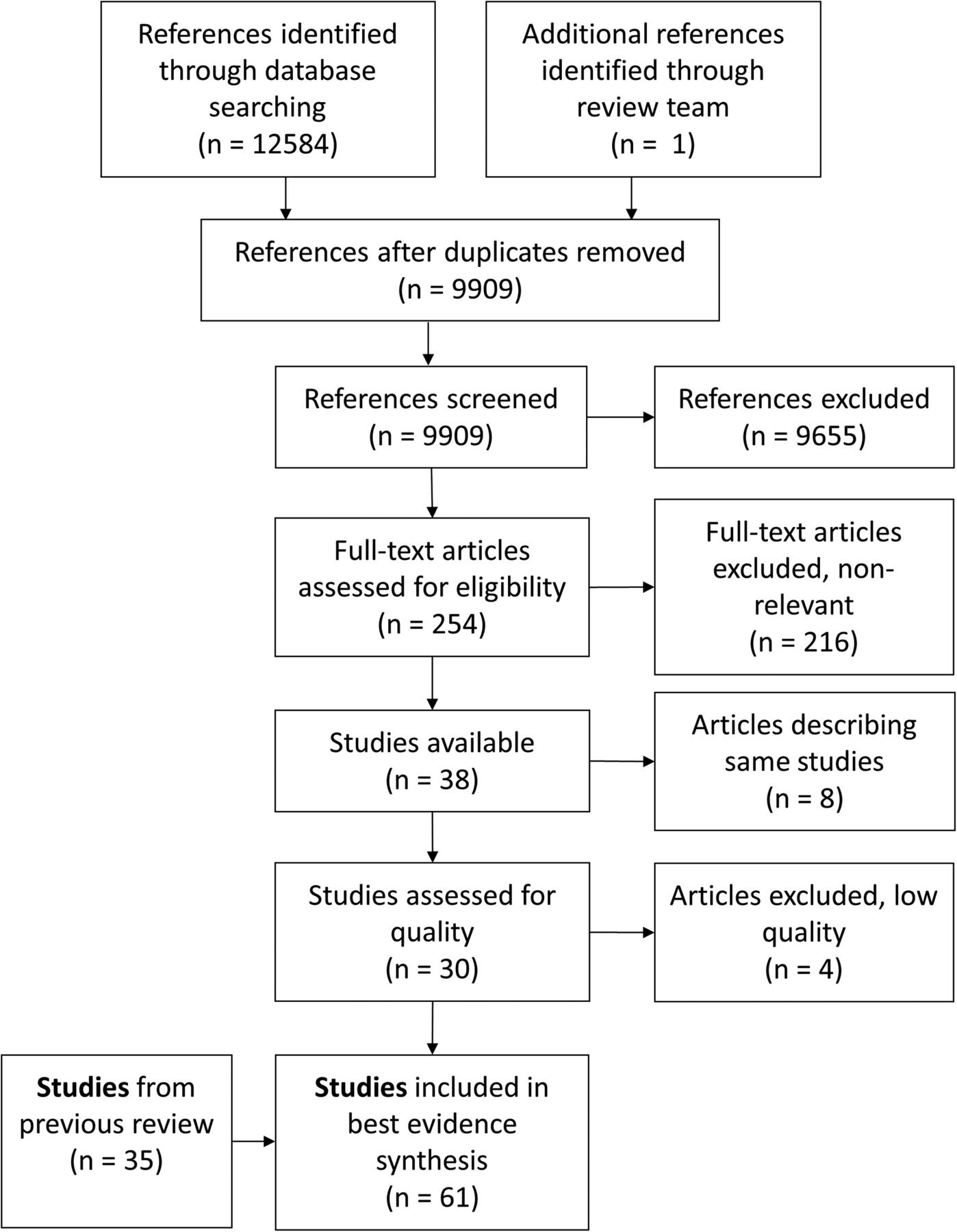{kind=link}
Flow chart of study identification, selection and synthesis.
Relevance screen
Overall, 9655 references and 216 full articles were excluded for not meeting relevance criteria (reference list is available from corresponding author on request). The remaining 38 relevant articles described 30 unique studies (figure 1).
Quality appraisal
Four studies were classified as low quality (<50% of criteria met), 14 studies were medium quality (50–85% of criteria met), and 12 studies were high quality (>85% of criteria met; see online supplementary table S2). Low-quality studies had high loss to follow-up, found differences in baseline characteristics between intervention and control groups, participants’ outcomes were not analysed by the groups they were originally allocated to, and the statistical analyses were not optimised for best results (eg, not accounting for baseline differences). The quality criteria that differentiated medium-quality and high-quality studies were also loss to follow-up and whether statistical methods were optimised for best results.
Four low-quality studies40–43 did not move on to data extraction leaving 26 studies (34 articles) for data extraction.
Data extraction
Study characteristics
The study designs included randomised controlled trials (n=9), cluster-randomised controlled trials (n=12) and non-randomised trials with a control group (n=5).
The studies came from the Netherlands (n=7), Denmark (n=6), Finland (n=3), Italy (n=2), the USA (n=2), India (n=1), Canada (n=1), Brazil (n=1), Malaysia (n=1), Sweden (n=1) and Israel (n=1).
The sectors included public administration (n=5), professional, scientific or technical services (n=5), manufacturing (n=3), retail (n=1), healthcare and social assistance (n=5), educational services (n=4), hospitality (n=1), armed services (n=1), municipality (n=1), other (n=9), and unknown (n=1). Some studies included populations from multiple sectors. Out of the 26 studies, 16 were considered office based. Overall, positive effects were reported for at least one outcome in 19 of the 26 studies.
Combining studies from original and update
To present an up-to-date synthesis of the evidence, we combined 35 studies46 ,79–112 from the original review23 with the 26 studies from the update for a total of 61 studies.
Intervention effects
There were no negative effects reported in the 61 studies (see online supplementary table S3). The most common UEMSD outcome reported was symptoms. Additional outcomes included sickness absence, disability, disorders (diagnosed) and physical function.
Evidence synthesis
The interventions across the 61 studies were grouped into 30 different intervention categories (see online supplementary table S3) and evidence synthesis for each category was determined (table 2). The intervention category evidence was paired with practical messages (table 2).
Level of evidence for UEMSD interventions and accompanying messages
The message content was determined through iterative stakeholder consultations to improve practicality. The messages were worded to help clarify the strength of the evidence, limit misinterpretation and increase user uptake.
Seven studies were identified and grouped within the resistance exercise category. Four high-quality44–47 and three medium-quality studies48–50 presented a positive effect of resistance exercise, such as dumbbell or kettlebell exercises, on UEMSD outcomes (see online supplementary table S3 for a more complete description of the resistance training programmes; see table 3 for a description of the work environments and sector). The strong level of evidence resulted in the message: implementing a workplace-based resistance training exercise programme can help prevent and manage UEMSD and symptoms.
Characteristics of studies
Three intervention categories had a moderate level of evidence showing a positive effect on UEMSD outcomes (see tables 2, 3 and see online supplementary table S3 for details). The forearm supports category had evidence from two high-quality studies79 ,91 and one medium-quality study.80 The vibration feedback about static mouse use category includes evidence from two high quality studies62 ,67 and one medium quality study.53 The stretching exercise programmes category includes evidence from one high-quality study68–70 and five medium-quality studies.60 ,61 ,63 ,81 ,82 The moderate level of evidence of a positive effect resulted in the message: consider implementing these interventions if applicable to the work context.
Three additional studies showed a moderate level of evidence for no effect on UEMSD outcomes. These intervention categories include: EMG biofeedback with two high-quality studies83 ,84 and three medium-quality studies;64 ,65 ,85 ,86 job stress management training category with two high-quality studies;87 ,88 and office workstation adjustment category with one high-quality study89 and three medium-quality studies.73 ,74 ,90 Since there was a moderate level of evidence that these three intervention categories have no effect on UEMSD outcomes, the resulting message is: seek alternatives if possible based on your OHS experience/knowledge.
The remaining 23 intervention categories had too few high-quality studies or had conflicting evidence across studies, resulting in the message: there is not enough evidence from the scientific literature to guide current policies or practices. For a message to be provided for these interventions, more high-quality evidence is needed (table 2).
Discussion
Preventing UEMSD injury and disability is challenging. OHS practitioners are charged with designing and implementing solutions. Evidence-based approaches should help identify and implement more effective solutions. Optimal evidence-based practice employs the knowledge and experience of practitioners along with the most up-to-date evidence from the scientific literature in the context of the client (patient, worker, etc) to determine prevention solutions.113
It can be challenging for busy OHS practitioners to find and read the latest research on any given topic. This challenge is compounded by the increase in the number of OHS publications year to year. Using the same literature search strategy as the earlier review,23 we found over 9900 references in a 5-year period (2008–2013) as compared with approximately 15 400 in a much longer period (mid-1960s–2008). We did find a higher proportion of relevant high-quality studies (50% vs 39%) in the past 5 years as compared with the original review.23
The current review and evidence update gathers and synthesises the scientific literature and presents practical messages for OHS practitioners. The review team consulted with OHS stakeholders to help ensure the messages were useful and applicable in practice.
Combining newer studies with those from the original review resulted in the potential for stronger levels of evidence according to our synthesis approach. However, the new studies also resulted in a greater number of intervention categories as compared with the original review. While we found a strong level of evidence for the positive effect of resistance training, the remaining findings were quite consistent with the original review. Our finding of moderate levels of evidence for positive effects of arm supports is consistent with the original review as is the moderate evidence for no effect of EMG biofeedback and of job stress management training. Kennedy et al23 found a strong level of evidence for no effect of workstation adjustments alone, while in the current update, a moderate level of evidence was found. In this case, one of the newer medium-quality studies had a positive outcome; we note that worker engagement was higher in the recent studies than it was in the original studies, which also contributed to the change in level of evidence.
The diversity of workplace-based interventions for UEMSD likely reflects the variety of potential relevant hazards, the number and types of UEMSD, the distinctness of workplaces, and the practical challenges of trying to design, implement and evaluate policies, programmes and practices. We note that there are many studies (approximately 60%) conducted in office-based workplaces. There are a number of potential reasons for this: the prevalence of UEMSD in office-workers,1 the nature of the work and workplace with similar equipment designs and work patterns, or possibly because it is easier to conduct an evaluation in an office setting. Office settings may have more consistent work schedules (less shift work), typically there are individual (non-shared) workstations, and the workstation can be relatively easily modified (through adjustment or alternative products). While it may be more challenging to implement and study interventions in non-office settings, our findings suggest it is possible.
Our findings are consistent with other recent reviews that included workplace-based interventions.17 ,18 ,114 ,115 Reviews that focused on RCTs only and attempted a meta-analysis also did not find strong levels of evidence for workplace interventions.19–22 While the findings are consistent, our synthesis of workplace-based interventions to prevent and manage UEMSD includes practical messages for, and developed with, practitioners.
A unique aspect of this review (update) was the integration of messages related to the levels of evidence developed with OHS stakeholders.39 We shared our review findings with multiple groups of OHS stakeholders and received feedback about how to create useful messages. The iterative approach35 led to concise messages that focused on practice as well as context that a varied group of OHS stakeholders agreed on. The messages are in keeping with an evidence-based practice approach. They provide recommendations or practice considerations to be weighed by the practitioner based on their own knowledge and experience along with the context and end-user needs.
Despite the useful messages provided here, more high-quality workplace-based intervention research is required. Current studies show high-quality evaluations that incorporate concurrent comparison groups (in some cases using randomisation) can be designed and performed. Importantly, the interventions must be properly implemented.
Strengths and limitations
A meta-analysis was not conducted due to the substantial intervention heterogeneity, different workplace contexts and study designs. Instead, a best evidence synthesis (BES) approach consistent with the original review23 was used. While this approach has been criticised,27 it provides practitioners with useful information. In addition, the BES is a transparent approach with clearly defined criteria to determine the level of evidence. Beyond the messages that arise from the consistent algorithm employed, practitioners can also consider the evidence from the individual studies. This is especially useful when there are few studies available for a given intervention type. Practitioners must come up with solutions even when there is a lack of scientific evidence available.
The likelihood of publication bias was not addressed; however, we included many relevant peer-reviewed studies that reported no effects for important outcomes. A key aspect of publication bias is that studies reporting positive effects are more likely to be published. While publication bias cannot be ruled out, the number of studies reporting no effects suggests publication bias is not a significant issue in this synthesis.
To determine intervention effects from individual studies, we decided to classify an intervention effect as positive when the study reported any positive result. This followed the method used in the original review.23 Hence, if a single study outcome regarding UEMSD showed positive results while several other UEMSD study outcomes showed no effect, then this study was still classified as positive intervention effect. Since classification of effect is often based on the primary outcome results, it should be noted that we were not conservative in this part of our evidence synthesis approach. However, we feel that any positive effect might benefit workers and should be taken into account in evidence-based practice.
A particular strength of the synthesis is the OHS stakeholder engagement throughout the review process. Stakeholders helped ensure we were asking a relevant question. Stakeholders were also asked for advice regarding possible literature search terms to ensure our search was up-to-date. Stakeholders were consulted about our findings and how to word the messages for OHS practitioners (consultants or in the workplace) to support evidence-based practice approaches.
Conclusions
Our synthesis update of the scientific literature identified 30 different intervention types from 61 evaluation studies. There were many intervention types that did not meet the criteria for high or moderate levels of evidence. However, we note that this does not mean that the interventions are not effective, only that there is insufficient evidence to support recommending these interventions based on the scientific evidence.
No intervention evaluations produced negative effects (eg, increased symptoms or lost time claims). However, job stress management training, EMG biofeedback training and workstation adjustment alone interventions had a moderate level of evidence of no effect for UEMSD outcomes. Practitioners should consider seeking alternative interventions based on OHS experience/knowledge.
Stretching exercise programmes, vibration feedback on mouse use and workstation forearm supports had a moderate level of evidence for a positive effect in preventing UEMSD. Practitioners should consider implementing stretching exercise programmes, vibration feedback on mouse use or workstation forearm supports in practices if applicable to the work context.
Resistance training programmes had a strong level of evidence. We recommend implementing a workplace-based resistance training exercise programme to help prevent and manage UEMSD symptoms and disorders.
Acknowledgments
Quenby Mahood, Joanna Liu and the IWH library for valuable help with search strategy design/execution and article acquisition. Trevor King for knowledge transfer and exchange activities and stakeholder engagement. Our stakeholders for their suggestions about practical messages. The Institute for Work & Health operates with the support of the Province of Ontario. The views expressed in this publication are those of the authors and do not necessarily reflect those of the Province of Ontario.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
- Data supplement 1 - Online table
Footnotes
Contributors DVE and EI conceived the study with input from BA. EI developed the search strategy with library support (acknowledged), all authors reviewed the search terms. All authors contributed to article screening, quality appraisal, data extraction and synthesis. DVE, CM and EI wrote the draft paper. All authors contributed to writing, reviewing or revising the paper and have read and approved the final manuscript.
Funding Ontario Ministry of Labour. KS is funded by the UK Medical Research Council (MCUU12017/8 and MCPC13027).
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.