Article Text

Abstract
Objectives The effect of retirement on mental health is not well understood. We examined the prevalence of hospital treatment for depression and purchase of antidepressant medication before, during and after retirement in a Danish population sample. We hypothesised that retirement was followed by reduced prevalence of hospital treatment for depression and antidepressant purchase.
Methods Participants were 245 082 Danish workers who retired between 2000 and 2006. Information on retirement, hospital treatment and antidepressant purchases were obtained from Danish national registers. The yearly prevalence of hospital treatment for depression and antidepressant purchases was estimated in relation to the year of retirement from 5 years prior to the retirement year to 5 years after retirement. Using logistic regressions with generalised estimating equations we analysed the trends in prevalence before, during and after the retirement.
Results Two of 1000 participants were hospitalised with depression in the year of their retirement and 63 of 1000 purchased antidepressant medication during the retirement year. The prevalence of hospital treatment for depression increased before and around retirement, followed by a slight decline from 2 years after retirement with the prevalence of hospitalisation dropping from 0.21%(retirement +2 years) to 0.16% (retirement +5 years). For antidepressants, we observed a steady increase in purchases before retirement (retirement −2 years). This increase levelled off in the years around retirement, but continued after retirement (retirement +2 years).
Conclusions Overall, this study did not confirm the hypothesis that retirement is beneficial for mental health measured by hospitalisation with depression and treatment with antidepressants. Although the temporary levelling off of the increase in antidepressant treatment around time of retirement might indicate a beneficial effect, this possible effect was only short-term.
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
What this paper adds
-
Previous studies, largely based on self-reported data, suggest that retirement is beneficial for mental health.
-
However, studies using medically certified outcomes are scarce.
-
Using hospital discharge diagnoses of depression and antidepressant purchases as end points we find no strong evidence of improvements in mental health following retirement.
-
With increasing retirement age in the OECD (Organisation for Economic Co-operation and Development) countries, work environment and health among elderly workers should be a priority in future research.
Background
Increasing life expectancy and decreasing fertility rates are reducing the proportion of gainfully employed individuals throughout the OECD (Organisation for Economic Co-operation and Development) countries.1 ,2 A possible means to increase the proportion of active workers is to raise the statutory retirement age. Despite recent high-quality studies on mental health and retirement,3–5 the knowledge regarding the potential mental health consequences of such an increase is still scarce.
Depression is associated with lower quality of life and is one of the leading causes of years lost due to disability, according to WHO.6 Denmark is among the countries with the highest level of prescription of antidepressants in the OECD, only surpassed by Iceland, Australia and Canada.2 The high treatment prevalence in Denmark could indicate a high prevalence of depression in the Danish population, but could also indicate a high awareness of mental problems, good access to health professionals or low costs of prescription drugs in Denmark or a combination of these factors. Elderly residents are particularly frequent users of antidepressants which could be due to more frequent contact with health professionals, frequent use of antidepressants in eldercare homes, increasing morbidity, and more frequent experiences of death of friends and relatives.
Stressful life events and psychosocial factors at work have both been proposed as risk factors for depression.7–9 Thus, removing exposure to adverse conditions at work by retiring might decrease the risk of depression. However, work may provide protective factors, such as time structure and positive social relationships, and, consequently, the risk of depression might increase after retirement. Studies have shown that retirement may influence health behaviours, resulting in weight gain,10 leisure time physical activity11 and increased alcohol consumption around time of retirement,12 which may affect mental health.
Recent prospective studies with self-reported mental health outcomes consistently found improvements in mental health after retirement,13–17 whereas results from earlier studies were less consistent.18–21 Studies on mental health with medically certified outcomes offer a different perspective than self-reported outcomes and give the opportunity for large-scale studies if register data are used. A review study concluded that there is strong evidence for beneficial effects of retirement on mental health.22 However, in two recent Finnish studies using treatment with antidepressants as the outcome, no clear improvements in mental health were found following old-age retirement.4 ,5 However, in another study from Finland, Oksanen et al3 found a decline in use of antidepressants around the retirement point.
We aim to examine the effect of retirement on depression using national Danish registers of hospital treatment for depression (HTD). To the best of our knowledge, effects of retirement on mental health have never been studied using hospital discharges as end points and never in a full national population. In addition, we studied effects of retirement on registered purchases of antidepressant medication, which gave opportunity for analyses of mental health studies with high statistical power and for direct comparison with recent register studies on retirement with medication as end points.3–5 Danish registers offer high-quality data with regard to completeness and consistency,23–26 and provide the opportunity to study effects of retirement on mental health in a full population study. Thus, bias due to selection into the study sample and to drop-out can be avoided in these register studies.
We hypothesise that retirement is associated with a reduced prevalence of HTD and antidepressant purchase when age is taken into account.
Design and methods
Population
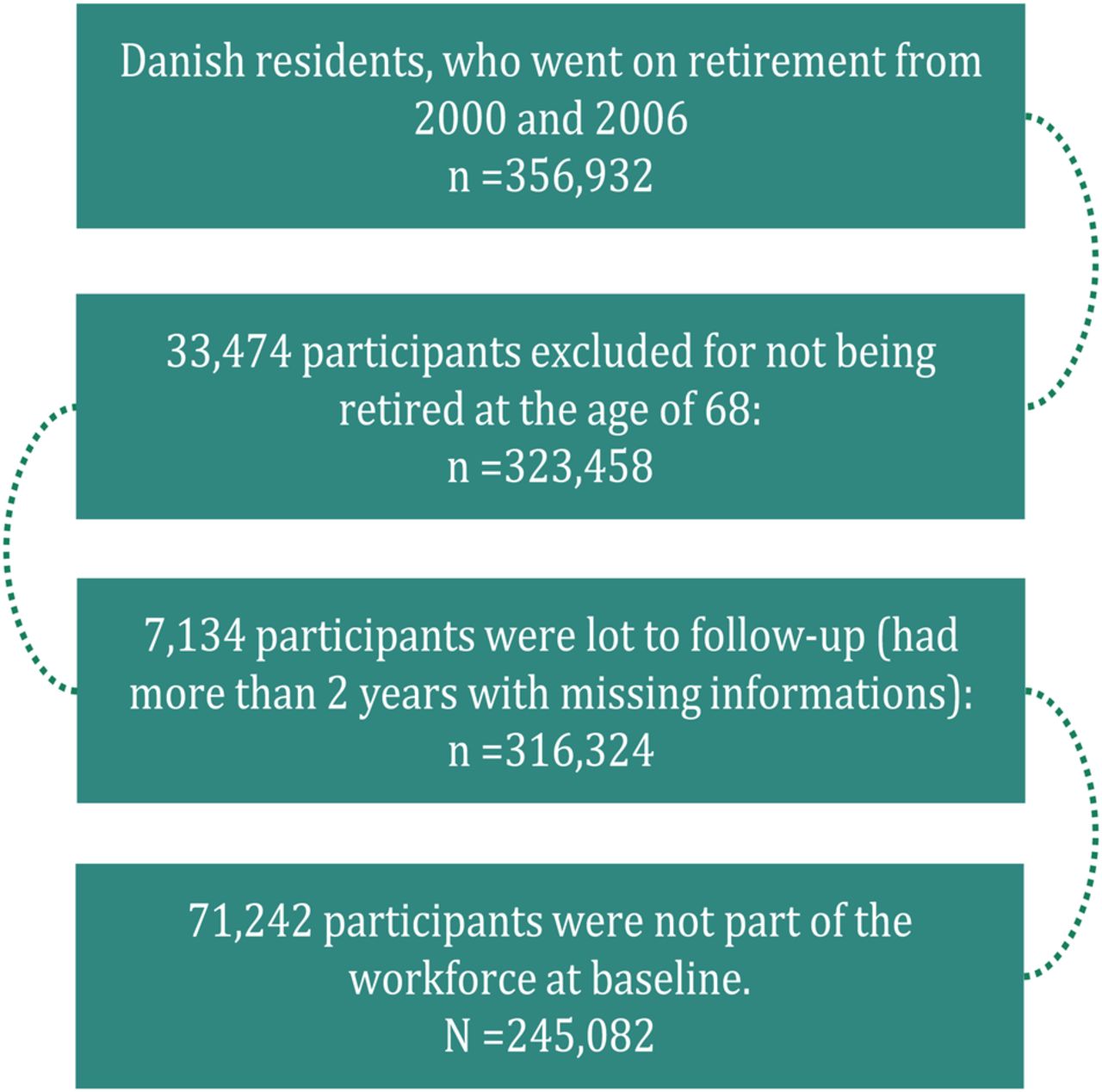
All Danish residents have a unique personal identification number that allows for individual level linkage to administrative and health registers. We utilised this resource to create a registry-based cohort study including all 356 932 Danish residents who went on retirement from 2000 and 2006. We excluded 31 068 participants who took retirement after the age of 68, as we suspected those older retirees to be a select group with work-characteristics no longer representative of the overall population. Further, we excluded 7134 participants who were lost to follow-up because of death or migration resulting in more than 2 years with missing observations. We also excluded 71 242 participants who were not a part of the workforce 1 year before baseline, yielding an analytic sample of 245 082 participants. Figure 1 illustrates the selection process of the study population.

Flowchart of the study population.
Assessment of retirement
During the follow-up period (2000–2006), three main types of retirement were available in Denmark: (A) old-age pension, available for all workers at the age of 67 and above. From 1 July 2004, workers born after 1 July 1939 could retire on old-age pension at the age of 65; (B) postemployment wage programme (PEW), available for qualifying workers from the age of 60 and until the statutory retirement age, although working beyond the age of 60 would progressively improve the pension. The eligibility criteria were based on age and seniority in an unemployment fund but there were no health criteria. PEW became one of the major means by which Danes took retirement during the follow-up period. PEW was particularly popular among workers with low wages who could retain the highest percentage of their pre-retirement income during retirement; (C) disability pension, available for workers at any age who were unable to work for either medical or psychological reasons. We obtained data on old-age pension from the Register-based Labour Force Statistics23 on PEW, and disability pension from the Danish Register for Evaluation of Marginalization (DREAM).24 When a participant was, for the first time, awarded old-age pension or PEW in these registers, the date was considered the time of retirement. For the purpose of this study, participants on disability pension were not considered retired until they were awarded either PEW or old-age retirement. Participants awarded disability pension more than 1 year before baseline were not included in the study.
Assessment of HTD and antidepressant purchase
We used two different indicators of mental disorders, which we analysed separately: HTD as primary diagnosis and purchase of prescriptive antidepressant drugs. Information on hospital discharges was drawn from The Danish Central Psychiatric Research Register, which includes all discharge codes for inpatient and outpatient psychiatric treatment and diagnoses in Danish hospitals since 1969.25 Relevant diagnosis included hospital treatment due to depression (International Classification of Diseases 10 codes of F32 to F33). Hospitalisation for depression is a relatively rare event compared with treatment with antidepressants, and only happens in cases of severe depression. Information on purchase of antidepressants was drawn from the Danish National Prescription Registry, a national Danish registry containing data on all purchases of prescription medication at Danish pharmacies since 1 January 1995.26 Antidepressants were defined as medications coded N06A by the Anatomical Therapeutic Chemical classification.27
Individuals having redeemed at least one purchase of antidepressants during a calendar year were categorised as prevalent antidepressant purchasers. Likewise, HTD during a calendar year resulted in categorisation as having depression that year. Unlike HTD, antidepressants are used in treatment for a range of mental disorders besides depression; they are more frequently used, and also used in cases of milder disorders. Thus we consider antidepressant purchase a measure of mental disorder rather than depression. It has to be noted that many individuals with depression are never hospitalised or treated with antidepressants and that therefore our outcome measures have low sensitivity.
Assessment of covariates
Information on sex, cohabitation, disposable income, level of education and area of residence were derived from national registers. Income and area of residence are likely to change during the follow-up, most likely as a direct consequence of retirement. To avoid adjusting for mediating factors, all covariates were measured before baseline, that is, 5 years before the year of retirement.
Statistical analysis
The analyses were based on 11 years of observation, which cover 5 years of observation time before and 5 years after the year of retirement, defined as time 0. Using logistic regressions with generalised estimating equations we calculated the annual prevalence of depression and its 95% CIs to visualise the trajectories in relation to the year of retirement. To analyse the trends in likelihood of depression and mental disorders, we divided the entire time-window into three periods, pre-retirement (5–2 years before retirement), retirement (a 3-year period centred around the time of retirement) and postretirement (2–5 years after retirement). A previous study reported beneficial effects of retirement on self-reported health when dividing time in relation to retirement in a similar way.14 We estimated the trend of mental health within each defined period by adding an interaction term between time period and time. We chose an autoregressive correlation structure to take the intraindividual correlations between the yearly observations into account. The analyses were adjusted for baseline sex, cohabitation, disposable income, educational level, age at retirement and calendar year. By adjusting for calendar year, the analyses were also adjusted for secular trends in medical treatment of mental disorders. We interpreted a change in the trend around or after retirement as an effect of retirement on mental health. All models were estimated separately for HTD and antidepressant drug purchase.
Further, we tested for possible modifying effects by sex, cohabitation and education by stratification of the sample.
Results
Table 1 shows the baseline characteristics of the study population with mutually adjusted ORs for prevalence of HTD and antidepressant purchase 2 years before retirement. Pre-retirement, women had a notably higher prevalence of antidepressant purchase compared with men, whereas the prevalence of HTD was more evenly distributed. Living alone, low income and high education were associated with a higher prevalence of HTD and of antidepressant purchases. Antidepressant drug purchases were evenly distributed across geographical regions, whereas HTD was more common among residents in Copenhagen than in other Danish regions.
Population characteristics
The mean age of retirement was 62.1 years, with a median of 61.8 years and a range of 60–68 years. A total of 202 356 persons (82.6%) retired with PEW, whereas 42 726 persons (17.4%) retired with old-age pensioning. There were 5195 cases of disability pensioning that were not regarded as retirement for the purpose of this study.
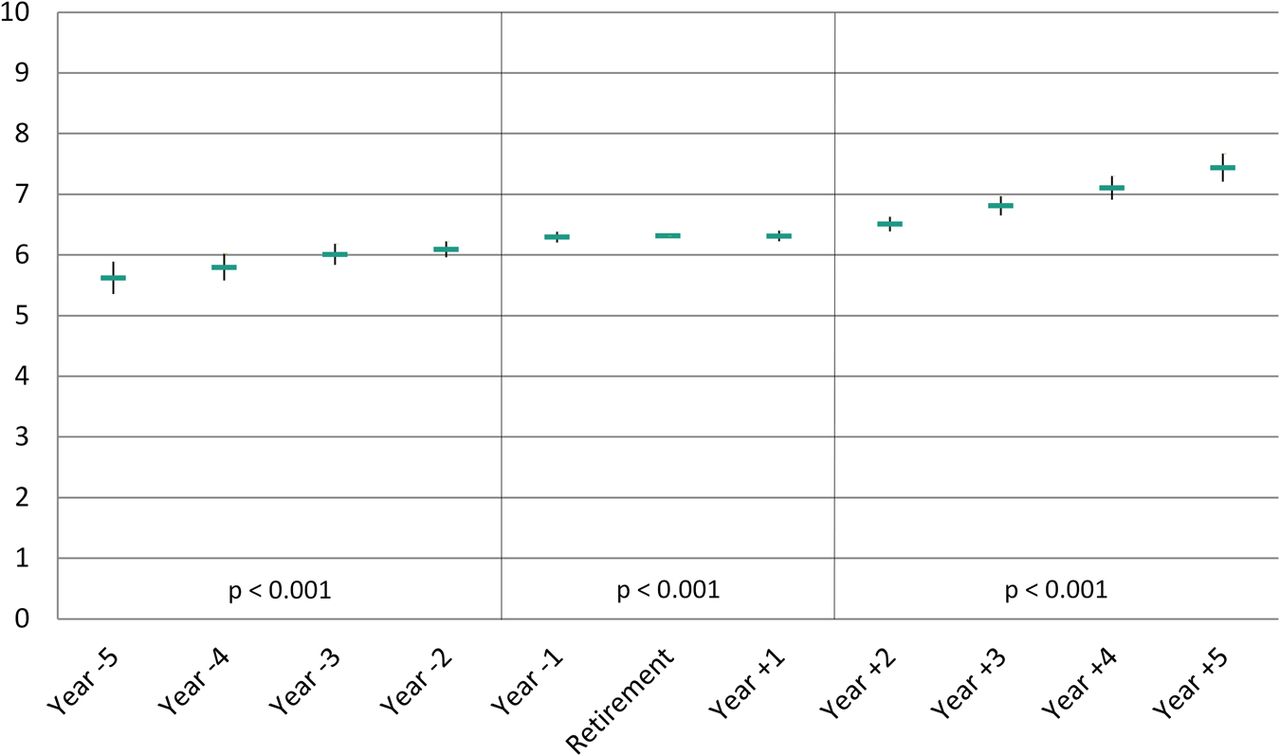
Figure 2 shows the trend in HTD in relation to retirement. There was an increase in prevalence in the pre-retirement period, a further increasing trend during the transition phase followed by a stagnating higher prevalence postretirement. The postretirement trend was statistically significantly different from the trend during the transition phase.

Estimated prevalence of hospital treatment for depression and its 95% CI in relation to year of retirement. Hospital treatment for depression per 10 000.
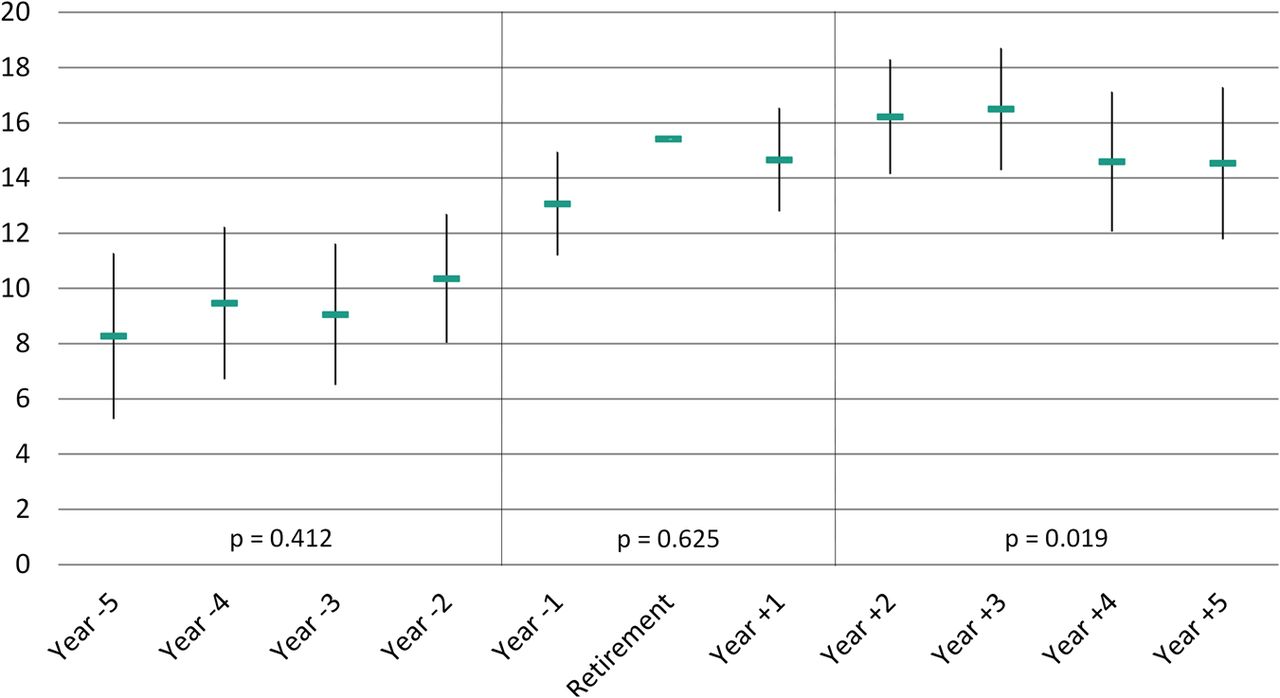
Figure 3 shows the trend in antidepressant purchases in relation to retirement. There was an increase in prevalence in the pre-retirement period. This increase levelled off in the years around retirement, but continued post retirement (retirement +2 years). All three periods differed statistically significantly from each other.
{kind=link}
{kind=link}
{kind=link}
Estimated prevalence of antidepressant purchasers and their 95% CI in relation to year of retirement. Antidepressant purchasers per 100.
Table 2 shows estimates for changes during each time-period (pre-retirement, transition, postretirement), stratified by selected covariates. The only statistically significant interaction effect we found was a modest effect for craftsmen who had reduced prevalence of HTD during the postretirement period. The trends in the subgroups were generally increasing and followed the trends from the full population.
Change in treatment for depression and antidepressant purchase during time period stratified by baseline characteristic
Discussion
Summary of findings
Overall, this study did not confirm the hypothesis that retirement is associated with improved mental health. However, the results suggest that retirement and mental health are differently associated depending on the measurement of the outcome.
Regarding HTD, we observed an increasing prevalence, except for the last years of observation. The trend was most pronounced in the transition period, possibly due to reverse causality, that is, individuals with depressive disorders being more likely to retire due to their illness. Although this increasing prevalence in HTD was broken postretirement, the prevalence remained high and we did not observe a notable decline in prevalence following the retirement.
Regarding antidepressant purchases, we found a steady increase before and after retirement that temporarily stopped during the transition phase. Thus, retirement did not result in a reduced prevalence but rather temporarily stopped the increasing trend in antidepressant purchases over time. The postretirement increase in prevalent antidepressant purchase indicates that possible short-term benefits of retirement around the retirement-point were lost during the subsequent years.
Interpretation of the results
The postretirement stagnation in prevalence of HTD may indicate that the effect of age on depressive disorder among participants in the workforce was stronger than the effect of age on participants who had retired. Such interpretation is, however, speculative, as it relies on the assumption that the pre-retirement increase in HTD is explained by age and not by the upcoming retirement. If the increase in prevalence before retirement is unrelated to retirement, that is, an effect of age, the postretirement trend may be interpreted as a beneficial effect of retirement, as the prevalence would have been even higher without the retirement. Contrarily, if the increased prevalence around the point of retirement was a consequence of the retirement, an overall interpretation would be that retirement is deleterious for mental health as the prevalence of HTD remains at a relatively high level after retirement without returning to the levels we observed 3–5 years before retirement.
The stagnated increase in prevalence of antidepressant purchases during the transition phase might indicate a beneficial effect of retirement. Many purchases are repeated events and we see an accumulation of treated persons during the observation window. Thus a stagnated trend in the prevalence might indicate a reduction in incident cases of treatment camouflaged by accumulation. However, the increase in treatment postretirement might then be an indication of deleterious effects of retirement. Thus, the possible beneficial effect of retirement during the transition phase is temporary and could possibly be a delay in treatment around the point of retirement rather than a lasting improvement in health.
We did not find convincing evidence of beneficial effects of retirement in any subpopulation. However, due to the register design, we did not have information on reasons for retirement nor expectations to retirement, which could be important for potential beneficial effects.
The prevalence patterns of the two examined indicators of depression differed. For HTD, the increase before and during transition to retirement was followed by stagnation during the postretirement period, whereas for antidepressant purchases the steepest increase was observed postretirement. This difference could have at least two explanations: first, HTD is relatively rare and likely indicates severe depression, whereas antidepressant purchase might be an indication of a wider range of mental disorders. Thus, antidepressant purchases may not only be a different measure of depression but might also measure different mental disorders. Consequently, our results may indicate that retirement is differently associated with different mental disorders. Second, a gradual reduction in a person's antidepressant purchases would not be captured in our study before the participant was free of any purchases during an entire calendar year. Thus, the increasing prevalence in antidepressant purchase during the whole study period may partly be explained by continued antidepressant treatment to prevent recurrence of the depressive disorder.
Comparison to other studies
There have been conflicting findings regarding ageing and mental health.16 ,28 In this study, we observed an increasing prevalence of antidepressant purchases as participants grew older. Thus, increasing age appears to be an important contributing factor for the observed increase in antidepressant purchase over the observation period.
In contrast to our results, findings from studies on retirement and self-reported mental health outcomes generally seem to favour the conclusion that retirement is beneficial for mental health.22 In a study on a British Whitehall cohort, statutory and voluntary retirement was associated with improved mental health.16 Studies on the French GAZEL cohort found beneficial effects of retirement with respect to sleep disturbances,15 self-reported depressive symptoms and mental fatigue13 and self-rated health.14 Another French study on effects of retirement on sleep disturbances confirmed the results from the GAZEL cohort.29
An exception to the abovementioned findings are studies on medication in relation to old-age retirement, which generally find little or no effect of retirement.3–5 Our findings on antidepressant purchases are consistent with these other longitudinal studies examining trajectories over time in relation to old-age retirement, which found no effect of retirement or suggested only minor benefits with respect to reduced medication. A Finnish study found a decrease in antidepressant use around the statutory retirement point,3 whereas another Finnish study found no change in use of psychotropic drugs following retirement.4 A third Finnish study on antidepressant use on a representative sample of the full population found no effect of old-age retirement on antidepressant medication.5 Our findings are in line with the results from the Finnish studies, suggesting that these findings are not dependent on specific national labour markets and retirement laws. To the best of our knowledge, medically diagnosed depression has not previously been studied and, therefore, our study adds to the current literature by showing no beneficial effect of retirement on HTD.
Taken together, these previous findings indicate that beneficial effects of retirement have mostly been found in studies using self-reported outcomes. Our findings support the tendency in the literature that studies with medically certified endpoints do not show evidence for beneficial effects of retirement.13 ,30
Strengths and limitations
The large sample-size covering an unselected national study population of retirees is a major strength of this study. Furthermore, the use of register-based predictors for mental disorders provided complete population data with a high level of consistency and reliability. Register-based measured HTD and antidepressant purchase are free of the bias due to self-reports, differential attrition and recall bias.
To the best of our knowledge, we are the first to analyse consequences of retirement on mental health in a full national population. Furthermore, hospital admission for depression has never before been studied as an outcome in retirement studies. Antidepressant and psychotropic drug purchase as outcomes are rarely used in the literature, limited to three studies in Finnish populations.
Several limitations of this study have to be noted. There is an inherent risk of reverse causality when studying the effect of retirement on mental health, as poor health may cause early retirement.31 Mental disorder is also a known predictor for early retirement in Denmark,32 thus there could be higher prevalence of mental disorders during transition to retirement if mental disorder is a trigger of the retirement decision. Flexible retirement age during the observation period has increased the risk of selection into retirement based on health criteria. However, the longitudinal design comparing the same individuals before and after retirement secured the fact that individuals were given equal weight at all times across the follow-up regardless of vulnerability to mental disorders. The design also gave opportunity for adjustments for the increasing secular trend in treatment for mental disorders during the follow-up.
We could not distinguish between voluntary and involuntary retirement, that is, retirement related to unemployment or threat of unemployment. The importance of such distinction has been shown previously in studies on health effects of involuntary job loss in an earlier career.33 These studies indicate that the context of the withdrawal from paid work is important for subsequent health, as involuntary job-loss was associated with increased risk of morbidity, including mental disorders.33 ,34 The beneficial effects of retirement, opposed to the deleterious effects of involuntary job loss, may be a result of having fulfilled society's and one's own expectations in retirement.35
Using treatment for mental disorders rather than a direct measure of a specific illness also has some disadvantages. HTD and antidepressant purchase have limitations as proxy measures for mental disorders. Many cases of depression are treated outside of hospitals, which is indicated by the higher proportion of antidepressant purchase compared with HTD. Thus, we suspect many participants without hospitalisation suffer from depression, as only a minor proportion of mental disorder cases seem to result in hospitalisation in Denmark.36 Likewise, many participants may suffer from mental disorder without being treated with antidepressants. Furthermore, despite their name, ‘antidepressants’ are prescribed for a range of disorders besides depression, such as anxiety37 or neuropathic pain.38 ,39 Thus antidepressant purchase is likely an indicator of mental disorder rather than of only depression. We do, however, assume antidepressant purchase to be strongly correlated with depression.
Finally, HTD and antidepressant purchase might be socially patterned. A study on Danish register data has shown inconsistencies between depression measured by a self-rated symptom scale and register-based outcomes, indicating an underestimation of prevalence of depression among individuals with low socioeconomic position when using register data.40
In conclusion, our findings do not confirm the hypothesis that retirement is beneficial for mental health. The prevalence of hospital treated depression and antidepressants were both higher postretirement compared with pre-retirement. We observed an increase in HTD around the retirement point, which was not significantly reduced following the point of retirement. For purchases of antidepressants, there might have been a modest beneficial effect around retirement; this was, however, only temporary.
References
Footnotes
-
Contributors JPB designed the study with assistance from NHR and RR. KO modified the design, conducted the analyses and wrote the first draft of the manuscript. IEHM, JPB, NHR and RR revised the draft and all authors contributed to and approved the final version of the manuscript.
-
Funding This work was supported by the Danish Working Environment Research Fund (grant number 20110013127/1).
-
Competing interests None.
-
Ethics approval The study was approved by the Danish Data Protection Agency.
-
Provenance and peer review Not commissioned; externally peer reviewed.