Article Text

Abstract
The aim of this study was to estimate the prevalence of viral hepatitis C (HCV) infection among healthcare workers (HCWs) compared to the general population. A systematic search for the years 1989–2014 was conducted in the Medline, Embase and Cochrane databases. Studies on hepatitis C in HCWs were included if they incorporated either a control group or reference data for the general population. The study quality was classified as high, moderate or low. Pooled effect estimates were calculated to determine the odds of occupational infection. Heterogeneity between studies was analysed using the χ2 test (p<0.10) and quantified using the I2 test. 57 studies met our criteria for inclusion and 44 were included in the meta-analysis. Analysis of high and moderate quality studies showed a significantly increased OR for HCV infection in HCWs relative to control populations, with a value of 1.6 (95% CI 1.03 to 2.42). Stratification by study region gave an OR of 2.1 in low prevalence countries; while stratification by occupational groups gave an increased prevalence for medical (OR 2.2) and for laboratory staff (OR 2.2). The OR for professionals at high risk of blood contact was 2.7. The pooled analysis indicates that the prevalence of infection is significantly higher in HCWs than in the general population. The highest prevalence was observed among medical and laboratory staff. Prospective studies that focus on HCW-specific activity and personal risk factors for HCV infection are needed.
- Healthcare workers < Materials
- exposures and occupational groups
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Introduction
Viral hepatitis C (HCV) infection is caused by blood contact and is a public health problem throughout the world. Its clinical course may be severe and can lead to work disability or to death. Considerable costs are incurred for prophylactic and treatment measures and result from the chronic clinical progress of the disease, loss of working hours and premature death. According to the WHO, approximately 150 million people in the world are chronically infected with HCV, and hepatitis C is the cause of 350 000 deaths annually.1 HCV is mainly transmitted by contact with infected blood due to injuries to the skin or mucous membranes.2 Acute infection is often asymptomatic and therefore frequently overlooked. In up to 80% of patients, the clinical course is chronic, leading to an increased risk of developing hepatic cirrhosis or hepatic cell carcinoma.3 Risk factors for HCV infection include intravenous drug consumption, injury-prone sex (men with men) and blood transfusions before the introduction of diagnostic testing. There is no vaccine or postexposure prophylaxis for HCV infection.
Healthcare workers (HCWs) have contact with infected patients and their body fluids. A particularly important factor is repeated performance of exposure prone procedures (EPPs) that may cause injuries to employees.4 Injuries to medical and health staff from sharp or pointed objects are among the most frequently reported occupational accidents in healthcare.5 The results of epidemiological studies indicate that approximately 80% of HCWs have been affected by needlestick injuries (NSI).6 Many such injuries go unreported.6–8 The risk of seroconversion after an injury depends on factors including the type of injury (deep cuts or pricks), the quantity of infectious material transferred, the virus load in the index patient and possibly genetic factors in the injured person.8–10
The probability of HCV seroconversion after a NSI in Europe has been estimated as 0.42%.6 ,8 Although HCV infection as an occupational disease is statistically rare, the consequences for the HCW and the health system are considerable.7 ,11 ,12 In 2012, 79 HCV infections were reported to the German Institution for Statutory Accident Insurance and Prevention in Health and Welfare Services, and 47 infections were recognised as occupational diseases.13 Numerous studies have investigated the prevalence of HCV in HCWs, but the results have been inconsistent. The objective of the present study is to estimate the prevalence of HCV infection among HCWs compared to the general population. Which professionals are particularly affected by infection?
Methods
This study is reported in line with the Proposal for Reporting of Meta-analyses of Observational Studies (MOOSE).14
Search strategy and screening
A systematic literature search was performed in the Medline, Embase and Cochrane databases for the period from 1989 to 2014. This included all prevalence and incidence studies on hepatitis C in HCWs with either a control group or reference data on the general population. The Embase search was performed using the following search terms: (((((‘hepatitis C’) AND ‘occupational exposure’) AND ‘healthcare worker’) AND prevalence) OR incidence)—with and without truncation (see online supplementary file). The search strategy was adapted for the other databases. Additionally, we searched reference lists of the chosen studies and prior reviews. Where it was not possible to make a decision on a study's inclusion or exclusion based on the abstract, the full text of the study was examined. The studies were screened and their quality was assessed by two reviewers working independently and using predefined checklists. Disagreements were resolved by consensus.
Studies meeting the following criteria were considered for inclusion:
Population: HCWs in direct contact with patients or blood
Exposure: Study examines occupational exposure
Control: Control group/reference data for general population from other publications
Outcome: Serological test for HCV
Design: Prevalence and incidence studies
Languages: German, English, French, Spanish, Portuguese, Italian.
The following criteria led to exclusion from this study:
Population: HCWs without direct contact with patients or blood
Exposure: No occupational exposure
Control: No control group; reference data for the general population not taken from other publications
Outcome: No serological test for HCV
Design: Case reports, surveillance data.
In studies with several control groups, the ones selected were those that best reflected the general population. Studies that examined HCWs without a control group were only included when the results were compared with a population-based study performed within a period of 2 years before or after the actual investigation and in a comparable study region.
In this report, ‘healthcare worker’ (HCW) is defined as any person (eg, an employee or student) whose activities involve contact with patients or with blood or other body fluids from patients in a healthcare setting.15
Study quality
In accordance with the literature, we developed an instrument to assess the methodological quality of the observational studies included.16–20 Scores were awarded on the basis of the criteria below. A total of nine scores was possible (table 1).
Checklist for quality assessment
Quality of the laboratory test: Anti-HCV detection depends on the type of test used, and tests differ in quality (product and procedure). In order to standardise the quality assessment, we evaluated the presence of a confirmatory test, but not its quality or procedure. It was not possible to evaluate this in the primary studies, due to missing data.
Statistical analysis
For the meta-analysis, data were extracted from the studies using a standardised documentation form. The parameters were the number of employees examined and the proportion of employees tested as serologically positive. Prevalence ratios (ORs) were calculated as effect estimates using the Mantel-Haenszel method for dichotomous outcomes. The 95% CIs were generated. Additional analyses were performed after stratification by type of controls, study region, publication period, gender and professional group. Meta-analyses were carried out using Review Manager 5.2.
In accordance with the criteria of Trevisan et al,50 a pooled analysis was performed for professionals exposed to a high risk of blood contact from EPPs. This analysis included the following professions/working areas: surgeons, midwives, microbiologists, pathologists, blood bank and dialysis staff.
Stratification by study region was performed on the basis of national prevalence rates. Based on the publications of Te and Jensen,3 Hahne et al21 and Mohd Hanafiah et al,22 pooled effect estimates were calculated for low prevalence countries taking into account countries of north-west Europe and the USA. Studies from Japan were analysed separately as there have been reports that the rate of seroconversion is higher in Japan than in Europe.8
Studies that observed no HCV infection in either group were excluded from the meta-analysis as no information about the relative probability of the event could be derived.18
Heterogeneity and sensitivity analysis
The presence of heterogeneity was tested using the χ2 test, taking p<0.10 as the level of significance. An I2 test was performed to quantify the diversity between studies. If there was no evidence of heterogeneity, we used a variance approach with a fixed effect model.18 In cases of statistically significant heterogeneity (χ2 p value<0.10) and I2>50%, the pooled effect estimate was determined using the random effect model. To identify sources of variation, further stratification was performed relative to study quality and to performance of confirmatory tests. In addition, for the sensitivity analyses, the stability of the pooled estimate with respect to each study was investigated by excluding individual studies from the analysis.
Publication bias
Possible publication bias was visualised with a funnel plot. In addition, the probability of publication bias was tested using Egger's linear regression in SPSS V.20.23 The level of significance for asymmetry was taken as p<0.1. The calculated intercept is given with a 90% confidence range.
Results
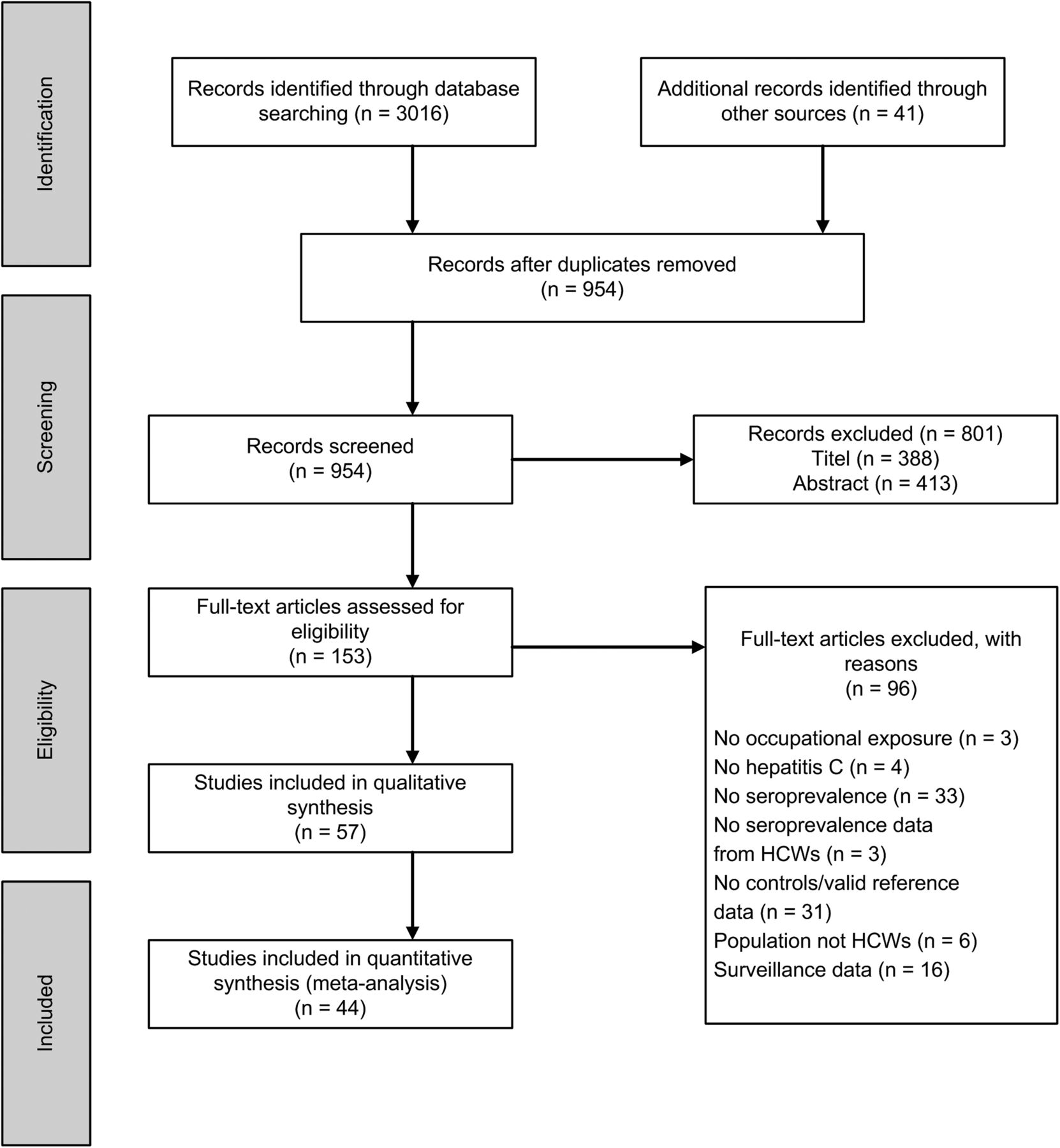
A total of 3016 publications were identified in the databases and 41 by manual search. After checking for duplicates, the titles and abstracts of 954 studies were screened, leading to the exclusion of 801 studies. The full texts of 153 studies were scrutinised and 57 studies were included in the systematic review. This selection process is given in figure 1.

Selection process. HCWs, health care workers.
Table 2 gives an overview of the studies included. A total of 27 studies from Europe were included, along with 13 from Asia, eight from Africa, seven from North America and two from South America. In most studies, HCWs were examined within the inter-professional framework. In five studies, the HCWs were stratified by professional group and, in five studies, by working area or exposure. Ten studies examined only a single professional group.
Characteristics of studies included
In 33 out of 57 studies, population-based controls, consisting mainly of blood donors, were used. A hospital control group was used in 18 studies. Ciorlia and Zanetta38 used a population-based and a hospital control group. Four studies used a population control and several other control groups, including risk groups such as dialysis patients and men who have sex with men.
Study design and quality
Fifty-one studies had a retrospective design and six a prospective design.24–29 The annual incidence was reported in two studies only. According to Puro et al,24 the rate was 0.1%; and 0.15% according to Cooper et al.26
The methodological quality was rated as high in seven studies, as moderate in 33 studies and as poor in 17 studies.
HCV detection
A HCV confirmation test was performed in 37 studies. Five studies used the same test for the confirmation as for the first test. There were differences between the studies with respect to the quality of the tests used (table 2).
HCV exposure among HCWs—a qualitative summary of studies not included in the meta-analysis
Thirteen studies could not be included in the meta-analysis because of missing case numbers (table 2). Increased HCV seroprevalence in HCWs in comparison to population controls was found in four out of seven studies of moderate methodological quality and in three out of six studies of low methodological quality. Cooper et al,26 Goetz et al53 and Zaaijer et al66 studied employees stratified by their exposure risk. All seropositive employees worked in areas with high exposure to blood contact (eg, dialysis, blood bank, laboratory), or reported prior NSI.26 With the exception of Mijakoski et al,73 all controls were from reference sources.
Meta-analysis
The main results are shown as plots in figure 2. Further results of pooling analyses and subgroup analyses are summarised in online supplementary table S3.

{kind=link}
{kind=link}
Forest plots of high and moderate quality studies on hepatitis C among healthcare workers. HCWs, health care workers.
A total of 44 studies were included in the pooled analysis (seven high quality studies, 26 moderate quality studies and 11 low quality studies—table 2). The pooled analysis of all studies showed a significantly increased OR of 1.5 (95% CI 1.15 to 2.06) for a HCV infection among HCWs compared to controls, with significant evidence of heterogeneity (χ2=110.8, p<0.001, I2=61, see online supplementary table S3). The increased prevalence of HCV infection in HCWs was also observed in the 14 studies with high and moderate methodological quality, using population control groups and confirmatory tests (OR 1.6; 95% CI 1.03 to 2.42, no evidence of heterogeneity, figure 2).
After stratification by publication period, HCWs were found to have a statistically significant increased prevalence of HCV infection in the period 1989–2000 compared with all controls (OR 1.3; 95% CI 1.09 to 1.63). For the period 2000–2014, the pooled effect estimate was the same, but without a statistically significant increase (OR 1.3; 95% CI 0.89 to 2.02). As there are only a few current studies, it was not possible to conduct a test for time trend by subgroups (see online supplementary table S3).
The following analyses were based on high and moderate quality studies only.
Study region
Pooled analysis of studies from countries with comparably low HCV prevalence in Europe (Belgium, Denmark, France, Scotland, Sweden) and the USA showed a significantly increased prevalence of HCV infection in HCWs compared with controls (OR 2.1; 95% CI 1.31 to 3.42, figure 2). Further stratification by population-based controls could not be performed because of considerable variability between the studies (I2=70). Pooled analysis of Japanese studies showed no increased HCV prevalence in HCWs (OR 1.1). Stratification of studies from the other countries by individual regions resulted in a statistically significant increased HCV prevalence in HCWs only for North Africa, the Middle East and South Asia (OR 1.9; 95% CI 1.10 to 3.15), compared to controls (see online supplementary table S3).
Gender
Six studies reported anti-HCV prevalence stratified by gender. By pooling studies using population-based controls with confirmatory tests, a significantly increased prevalence was observed only for male HCWs (women OR 1.5; 95% CI 0.45 to 5.24; men OR 3.1; 95% CI 1.21 to 7.99).
Professions
Medical staff: For medical personnel, pooled analysis of studies with confirmatory tests gave an OR of 2.7 (95% CI 1.65 to 4.51, figure 2). For medical staff excluding dentists, the OR was 2.2 (95% CI 1.30 to 3.77) for a HCV infection compared to population-based controls (see online supplementary material table S3).
Dental staff (medical and non-medical): Pooled analysis of studies with confirmatory tests gave an OR of 3.5 (95% CI 1.37 to 9.15, figure 2) for a HCV infection among dental staff compared to controls. Further stratification could not be performed because of considerable variability between the three studies.
Nursing staff: The pooled analysis of studies with confirmatory tests showed an OR of 1.7 (95% CI 0.86 to 3.31) for nursing staff compared to the population-based controls (see online supplementary table S3).
Laboratory staff: Pooled analysis of studies with confirmatory tests gave an increased OR of 2.2 (95% CI 1.10 to 4.39, figure 2) for a HCV infection in laboratory staff compared with all controls.
Professionals at high risk for blood contacts: Six sources contributed data on the following professions/working areas performing EPPs: surgeons, midwives, microbiologists, pathologists, blood bank and dialysis staff. All studies were published before 2000. The pooled analysis shows a statistically significant increased OR of 2.3 (95% CI 1.51 to 3.54) for a HCV infection among HCWs compared with all controls and of 2.7 (95% CI 1.84 to 5.53, figure 2) compared to population-based controls.
Heterogeneity and sensitivity analysis
Heterogeneity was present when pooling all studies. Pooling the studies with high and moderate methodological quality only, reduced heterogeneity. Further stratification was performed related to performance of confirmatory tests. In addition, individual studies were then sequentially excluded from the analysis in order to verify their influence on the pooled estimate.
Publication bias
The funnel plot did not show evidence of publication bias (see online supplementary figure S3), nor did Egger's linear regression show significant evidence of funnel plot asymmetry (intercept 0.19, 90% CI 0.33 to 0.71, p=0.47).
Discussion
This is the first systematic review to perform a meta-analysis on the prevalence of HCV infection among HCWs in comparison to controls. The pooled analysis of high and moderate quality studies gave a statistically significant increase in OR of 1.6 for HCV infection among HCWs compared to population-based controls. Stratified pooled analysis of studies with confirmatory tests from countries with comparable low HCV prevalence also resulted in a statistically significant increase in OR for HCWs in comparison to controls (OR 2.1). Stratification by occupational groups demonstrated an increased prevalence among medical staff (OR 2.2), laboratory staff (OR 2.2) and dental staff (medical and non-medical, OR 3.5), compared to controls. However, due to the few studies found for dental staff, further stratification by profession could not be performed. In addition, the pooled effect estimated is mainly caused by one high quality study with a wide CI.32 When the pooled analysis was stratified by nursing staff, no significant increase in OR was found. A differentiated examination of activity profile-related occupational hazards was carried out for this profession in only a few studies. This lack of differentiation may lead to underestimation of the occupational risk of infection due to exposure misclassification. This happens particularly when HCWs who are frequently exposed to blood while performing EPPs are examined in combination with less exposed HCWs in the same job category. Pooled analysis for each individual group—such as cleaning staff—was not possible as the studies were few and their methods heterogeneous in design, HCWs examined, serological testing and controls. This diversity is the main reason for the lack of consensus in the assessment of the occupational risk of HCV infection in HCWs.81–83 Additionally, it is difficult to quantify the occupational risk given to a specific profession, such as for laboratory staff, as there is no systematic record of how exposure depends on the activity.84 To estimate HCV prevalence in HCWs due to specific work profiles, we conducted an exemplary pooled analysis of professions that performed EPPs in accordance with the criteria of Trevisan et al.50 The pooled analysis shows a significantly increased OR of 2.7 for these employees in comparison to the population-based controls. However, the results of this subgroup analysis are based only on studies published before 2000. The assessment of personal risk factors for a HCV infection was not performed consistently in the investigated studies, particularly in studies published earlier. Those examinations were conducted prior to the Needlestick Safety and Prevention Act (NSPA). Both in the USA and in Europe, guidelines have been issued since 2000 that aim to prevent exposure to blood, for example, from NSI.6 ,85
The results of studies that could not be included in the quantitative analysis did not conflict with the results of the meta-analysis. Professions that performed EPPs are exposed to NSI, with a HCV transmission rate of 1.8% after an NSI according to Henderson,83 Riddell and Sherrard,86 and Baldo et al.87 The results of an American multicentre study performed in 2006 showed that occupational exposure was greater in male HCWs.88 The authors observed that men were three times more frequently infected than their female colleagues. In this context, bivariate analysis showed that glove use when performing invasive work was significantly associated with the female gender. According to the reviews of Kubitschke et al8 and Goniewicz et al,89 NSIs were more frequent in inexperienced personnel. Current findings on the incidence of NSI in the health service show that nursing6 ,88 ,90 and medical personnel88 are the most frequently affected professional group. According to Butsashvili et al88 the highest number of exposures to NSI is in dialysis work. The most recent research on dialysis staff (2006–2010) concluded that there had been no decrease in the number of observed NSIs suffered by staff.6
Strengths and limitations
This is the first meta-analysis to examine the prevalence of HCV infection in HCWs compared to controls. However, the mostly retrospective studies included some recent studies. In addition, older studies tend to report higher anti-HCV prevalence rates than more recent studies (as confirmed by Larney et al91). As there are only a few current studies, it was not possible to draw reliable conclusions about a time trend. Most of the population-based controls were blood donors. Individuals at risk of HCV infection in the general population were probably not included. The results of the studies that referred to reference populations must also be viewed critically. HCWs and controls may not have been tested under identical conditions. Few studies have examined how occupational hazards depend on the activity profile. This lack of differentiation may lead to underestimation of the occupational risk of infection for specific HCWs. So, the present results reveal a strong demand for further differentiated research.
Quality of serological testing
The quality of the confirmatory tests used clearly differs between individual studies. This is due to the development of better detection methods over time, the quality of the procedure or the fact that there is no fundamental difference between the antigens used in the screening and the confirmatory tests. Owing to the limitations in the sensitivity of the first anti-HCV tests (false negatives), earlier studies tended to underestimate seroprevalence. In contrast, limitations in specificity lead to false positive results. This may result in non-differential misclassification, which again is most likely to lead to decreased effect estimates.
Assessment of personal risk factors
The personal risk factors for HCV infection were not recorded consistently in the studies. The risk factors, such as use of injected drugs and injury-prone sex (men with men) were not collected in many studies, especially the earlier ones. The 1998 report of the US Center for Disease Control and Prevention (CDC) on the known risks of HCV infection identified drug use and injury-prone sex as the most common causes.15 Of the six studies that allow stratification by gender, only two examined these confounding factors, which are associated with a higher risk of non-occupationally acquired HCV infection, especially among men.32 ,36
Conclusion
This meta-analysis shows a statistically significant increase in the prevalence of HCV infection in HCWs compared to controls. Medical and laboratory personnel, and staff members who perform EPPs, are particularly affected. For other professions, no adequate calculation of a pooled estimate was possible. Prevalence of HCV infection has probably decreased since 2000, due to improved prevention. However, this needs to be investigated further. To analyse HCWs’ occupational risk of infection, prospective studies are needed that focus on HCWs in terms of specific work profiles bearing in mind the importance of assessment of personal risk factors for infection. Contact with blood, for example, from NSI, is associated with a risk of infection and continues to be the major threat to the health of HCWs. Targeted prevention measures must be based on the epidemiological detection and evaluation of work-related accidents. Readily accessible reporting and treatment procedures, and the use of safe practices for working with blood, can help to minimise occupational exposure.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
- Data supplement 1 - Online supplement
- Data supplement 2 - Online supplement
Footnotes
Collaborators Melanie Harling.
Contributors CW conceived the study protocol, performed the study selection, data extraction, quality assessment and statistical analysis, and wrote the first draft of the manuscript. CP was involved in performing data extraction, quality assessment and statistical analysis and made substantial contributions toward revising the first draft. BL performed the study selection and assessment, and made substantial contributions towards revising the first draft. ML made substantial contributions toward revising the first draft. AN coordinated the study, amended the study protocol, assisted in study selection and statistical analysis, and made substantial contributions toward revising the first draft.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.