Article Text

Abstract
Background Observational studies suggest that shift work may be associated with diabetes mellitus (DM). However, the results are inconsistent. No systematic reviews have applied quantitative techniques to compute summary risk estimates.
Objectives To conduct a meta-analysis of observational studies assessing the association between shift work and the risk of DM.
Methods Relevant studies were identified by a search of PubMed, Embase, Web of Science and ProQuest Dissertation and Theses databases to April 2014. We also reviewed reference lists from retrieved articles. We included observational studies that reported OR with 95% CIs for the association between shift work and the risk of DM. Two authors independently extracted data and assessed the study quality.
Results Twelve studies with 28 independent reports involving 226 652 participants and 14 595 patients with DM were included. A pooled adjusted OR for the association between ever exposure to shift work and DM risk was 1.09 (95% CI 1.05 to 1.12; p=0.014; I2=40.9%). Subgroup analyses suggested a stronger association between shift work and DM for men (OR=1.37, 95% CI 1.20 to 1.56) than for women (OR=1.09, 95% CI 1.04 to 1.14) (p for interaction=0.01). All shift work schedules with the exception of mixed shifts and evening shifts were associated with a statistically higher risk of DM than normal daytime schedules, and the difference among those shift work schedules was significant (p for interaction=0.04).
Conclusions Shift work is associated with an increased risk of DM. The increase was significantly higher among men and the rotating shift group, which warrants further studies.
Statistics from Altmetric.com
Introduction
Diabetes mellitus (DM) is considered to be one of the major public health challenges in both industrialised and developing countries.1 By the year 2025, the number of cases of type 2 diabetes mellitus (T2DM) will have increased by 65% to reach an estimated 380 million individuals worldwide. The substantial mortality and morbidity of DM impose enormous economic, health and societal costs.2 Therefore, the identification of modifiable risk factors for the primary prevention of DM is of considerable public health importance.3
Shift work involves irregular or unusual hours of work, compared with those of a normal daytime work schedule.4 Many different work schedules can be described as shift work, including regular evening or night schedule, rotating shifts, irregular schedules and so on.5 ,6 For shift workers, night work compromises cognitive capacity and challenges the physiological need for sleep and recuperation.7 The stress of shift work can induce tiredness, irregular sleep patterns and digestive problems.4 Studies have shown an association between shift work and breast cancer8 and vascular events.5 However, whether shift work increases the risk of DM remains unclear.
Over the past decades, a few epidemiological studies have assessed the association between shift work and the risk of DM, but the results are inconsistent. A previous systematic review6 summarised the association between shift work and chronic diseases, including DM, but did not use quantitative techniques to compute summary risk estimates between shift work and DM. Thus, we aimed to conduct a meta-analysis of observational studies to summarise the epidemiological evidence on an association between shift work and the risk of DM.
Methods
We planned and reported this review in accordance with the Meta-analysis Of Observational Studies in Epidemiology (MOOSE) guidelines.9
Search strategy
We conducted a literature search of PubMed, Embase, Web of Science, ProQuest Dissertation and Theses databases up to April 2014 for studies describing an association between shift work and DM. We used ‘shift work’ or ‘night shift work’ or ‘work schedule tolerance’ [Mesh] or ‘rotating shift work’ or ‘light at night’ or ‘work at night’ and ‘diabetes’, ‘diabetes mellitus’ [Mesh] or ‘impaired glucose tolerance’ or ‘impaired fasting glucose’ or ‘insulin resistance’ as the search terms. We imposed no limitation on the regional origin, the study design or the nature of the control group, which could consist of day workers or the general population. In addition, we reviewed the reference lists of retrieved articles to identify any studies that had not been identified by the preliminary literature searches. Only articles published in the English language were considered.
Inclusion criteria
Studies meeting the following criteria were included in the meta-analysis: (1) the study design was observational, (2) shift work was an exposure variable and the outcome was DM, (3) the study reported risk estimates with 95% CIs for the association between shift work and DM or provided sufficient information to allow their calculation. Animal studies, clinical trials, reviews, letters and commentaries were excluded. Studies were also excluded if they involved involuntary or non-work-related night-time light exposure, or included subjects with recurrent DM. If study populations were reported more than once, we included the result with the longest follow-up time. Two authors (YoG and CY) independently screened all studies by title or abstract and then by a full-text assessment. Disagreements were resolved through consultation with the third reviewer (ZL).
Data extraction
We extracted the following information from studies included: name of first author, year of publication, country of origin, study design, characteristics of the study population at baseline, duration of follow-up (for cohort study), outcome measurements, number of cases, number of participants, risk estimates and corresponding 95% CI and covariates adjusted in the statistical analysis. We classified shift work schedules according to the original study methodological description as rotating, irregular and unspecified, night, mixed and evening. Data extraction was conducted independently by two authors (YoG and CY). Interobserver agreement was assessed using Cohen's kappa (κ), and any disagreements were resolved by discussion with the third author (ZL).
Quality assessment
Two reviewers (YoG and CY) independently performed the quality assessment using the Newcastle-Ottawa Scale10 (for the cohort and case–control study), which is a nine-point scale allocating points based on the selection process of cohorts (0–4 points), the comparability of cohorts (0–2 points) and the identification of the exposure and the outcomes of study participants (0–3points). We assigned scores of 0–3, 4–6 and 7–9 for low, moderate and high quality of studies, respectively.
Assessment involving 11 items recommended by the Agency for Healthcare Research and Quality was applied for cross-sectional studies.11 The quality of the articles was first evaluated according to the established questions, which were scored according to the following: 1 point if the item was considered in the study, 0 points if the item was not considered or we were unable to determine if it had been considered. Each study was rated independently by two authors (YoG and CY); ratings are reported in online supplementary tables S2 and S3.
Statistical analysis
We preferentially pooled multivariable adjusted risk estimates where such estimates were reported. If adjusted analysis was unavailable (one study), we pooled the unadjusted estimate. The ORs were considered as a common measure of the association between shift work and DM, and both HRs and relative risks (RRs) were considered equivalent to ORs, because the ORs and RRs provide similar estimates of risk when the outcome is rare.12 One study13 consisting of two separate cohorts was considered as two independent studies. Another study14 respectively compared the risk estimates of two-shift and three-shift workers with fixed daytime workers, and was considered as two independent reports. Any studies stratified by sex, age or duration of shift work were also considered as independent reports.
Statistical heterogeneity among studies was evaluated using the I2 statistic, where values of 25%, 50% and 75% represent cut-off points for low, moderate and high degrees of heterogeneity, respectively.15 When appropriate, we used a fixed-effects model or random-effects model. The ORs were pooled using the fixed-effects model if no heterogeneity was detected, or the random-effects model was used otherwise, and the weights were equal to the inverse variance of each study's effect estimation.
We conducted subgroup analyses and sensitivity analyses to explore potential heterogeneity across studies, and the differences among subgroups were tested by meta-regression analysis (using STATA ‘metareg’ command). Priori hypotheses were formed to explore subgroup interactions to explain inconsistency in the direction and magnitude of associations among studies. We used the method of Altman and Bland to test the hypotheses of a subgroup effect, which involves a test of interaction with a predetermined two-tailed α of 0.05.16 We also conducted leave-one-out analyses17 for each study to examine the magnitude of influence of each study on pooled ORs.
Potential publication bias was assessed with visual inspection of the funnel plot, Begg correlation test18 and Egger linear regression test.19 We used the Duval and Tweedie's non-parametric trim-and-fill method to adjust potential publication bias.20 All statistical analyses were performed with STATA V.11.0 (StataCorp, College Station, Texas, USA). All tests were two sided with a significance level of 0.05.
Results
Study selection and evaluation
After removing duplicates, we identified 448 potentially relevant articles by electronic database searches. After reviewing the titles and abstracts, 434 studies were excluded because of non-compliance with the inclusion criteria. Twelve studies13 ,14 ,21–29 with 28 independent reports were finally included in the meta-analysis. A flow chart showing the study selection is presented in figure 1. Interobserver agreement (κ) between reviewers for study inclusion was outstanding (κ=0.95). The average score for all included cohort and cross-sectional studies was 7.9 and 5.3, respectively. The cross-sectional studies scored lower than others, while higher scores went with studies considering the adjustment of confounding factors more fully.

Flow chart showing the relevant observational studies of shift work in relation to diabetes mellitus.
Study characteristics
The characteristics of 12 studies are summarised in online supplementary table 1. They included seven prospective cohort studies,13 ,14 ,22 ,25 ,27 ,28 one retrospective cohort study24 and four cross-sectional studies,21 ,23 ,26 ,29 published between 1983 and 2013. The study samples ranged from 475 to 107 915, with a total of 226 652, and the number of cases of DM ranged from 21 to 6165, with a total of 14 595. The study locations were as follows: six studies14 ,21–23 ,25 ,26 were conducted in Japan, two24 ,27 in Sweden, two13 in the United States, one28 in Belgium, and one29 in China. Two studies27 ,29 included both men and women, eight studies14 ,21–26 ,28 men only and two studies13 women only. According to the classification of shift schedules, four studies21 ,24 ,25 ,28 were classified as rotating shifts, two27 ,29 were irregular or unspecified shifts, three13 ,23 ,26 were night shifts, two14 ,22 were mixed shift schedules and one14 was an evening shift. (The study of Morikawa et al14 reported two shift types.)
Association between shift work and risk of DM
Figure 2 show the results from the random-effects model combining the ORs for DM in relation to shift work. Ten of 28 independent reports from 12 studies suggested a positive relation between shift work and DM, while the other reports did not. The pooled OR of DM for shift work was 1.09 (95% CI 1.05 to 1.12), and a moderate heterogeneity was seen (p=0.014; I2=40.9%). For cohort studies, the combined OR was 1.12 (95% CI 1.06 to 1.19), and there was a moderate heterogeneity (I2=52.9%, p=0.007). For cross-sectional studies, the combined OR was 1.06 (95% CI 1.03 to 1.09), and a low heterogeneity was detected with an I2=10.9% across cross-sectional studies.

Pooled random effects OR and 95% CIs for the association of shift work and diabetes mellitus by study design.
Subgroup analyses
Table 1 shows the results from subgroup analyses examining the stability of the primary results and exploring the resource of potential heterogeneity. To assess whether specific study characteristics influenced the association between shift work and DM, we performed subgroup analyses by sex, study design, study location, occupation, shift schedule, and whether body mass index (BMI), family history of DM or physical activity were controlled or not in models. Shift work was associated with an increased risk of DM in most subgroups. The increased risk was more evident in the groups with a rotating shift schedule, male shift workers and lack of statistical control for BMI or physical activity. Subgroup analysis by shift schedules showed that rotating shifts, irregular and unspecific shifts and night shifts were associated with an increased risk of DM. The highest point estimate was noted for rotating shifts (OR=1.42, 95% CI 1.19 to 1.69). The difference in the pooled OR among these five groups reached statistical significance (p for interaction=0.04), suggesting an interaction between shift work and shift schedule. Subgroup analysis by sex showed a greater increase of odds in men (OR=1.37, 95% CI 1.20 to 1.56) than in women (OR=1.09, 95% CI 1.04 to 1.14), and the difference was significant (p for interaction=0.01). Additionally, the increased risk was more pronounced for participants from Europe than Asia and the USA, but the difference did not reach statistical significance (p for interaction=0.13). Study design, occupation and adjustment for family history of DM also did not influence the summary ORs (see table 1).
Subgroup analyses of OR of diabetes mellitus according to shift work status
Sensitivity analyses
Sensitivity analyses were used to find potential origins of heterogeneity in the association between shift work and DM risk, and to examine the influence of various exclusions on the combined OR, and checkout the robustness of all results above. We compared the fixed-effect and random-effect models, but found no significant difference in the pooled OR between the two (fixed-effects model pooled OR=1.06, 95% CI 1.05 to 1.08, random-effects model pooled OR=1.09, 95% CI 1.05 to 1.12). Exclusion of one study without adjusting any confounded factors yielded a pooled OR of 1.08 (95% CI 1.05 to 1.12). A medium heterogeneity was detected with an I2=37.2%. Exclusion of the study by Pan et al, which had the largest sample size, yielded a pooled OR (1.09; 95% CI 1.04 to 1.15; p=0.054, I2=36.2%). Moreover, when this large sample study was excluded, the associations with shift work were still stronger in men than in women for DM (p for interaction=0.004), and higher in the rotating shift group than in other groups (p for interaction=0.019). The differences between sex-specific and shift schedule-specific relations were robust, and were not driven by the Nurse's Heath Study. Therefore, it was relatively appropriate to combine the results from small studies together with a big study in our meta-analysis. Restricting analysis to studies that specified the type of diabetes outcome as T2DM yielded a pooled OR of 1.11 (95% CI 1.04 to 1.17). The positive association was not materially changed in the leave-one-out analyses by omitting one study in turn, with a pooled OR range from 1.08 (95% CI 1.05 to 1.11; p=0.057) to 1.13 (95% CI 1.07 to 1.20; p=0.008), which indicated that none of the individual studies significantly influenced the overall result.
Publication bias
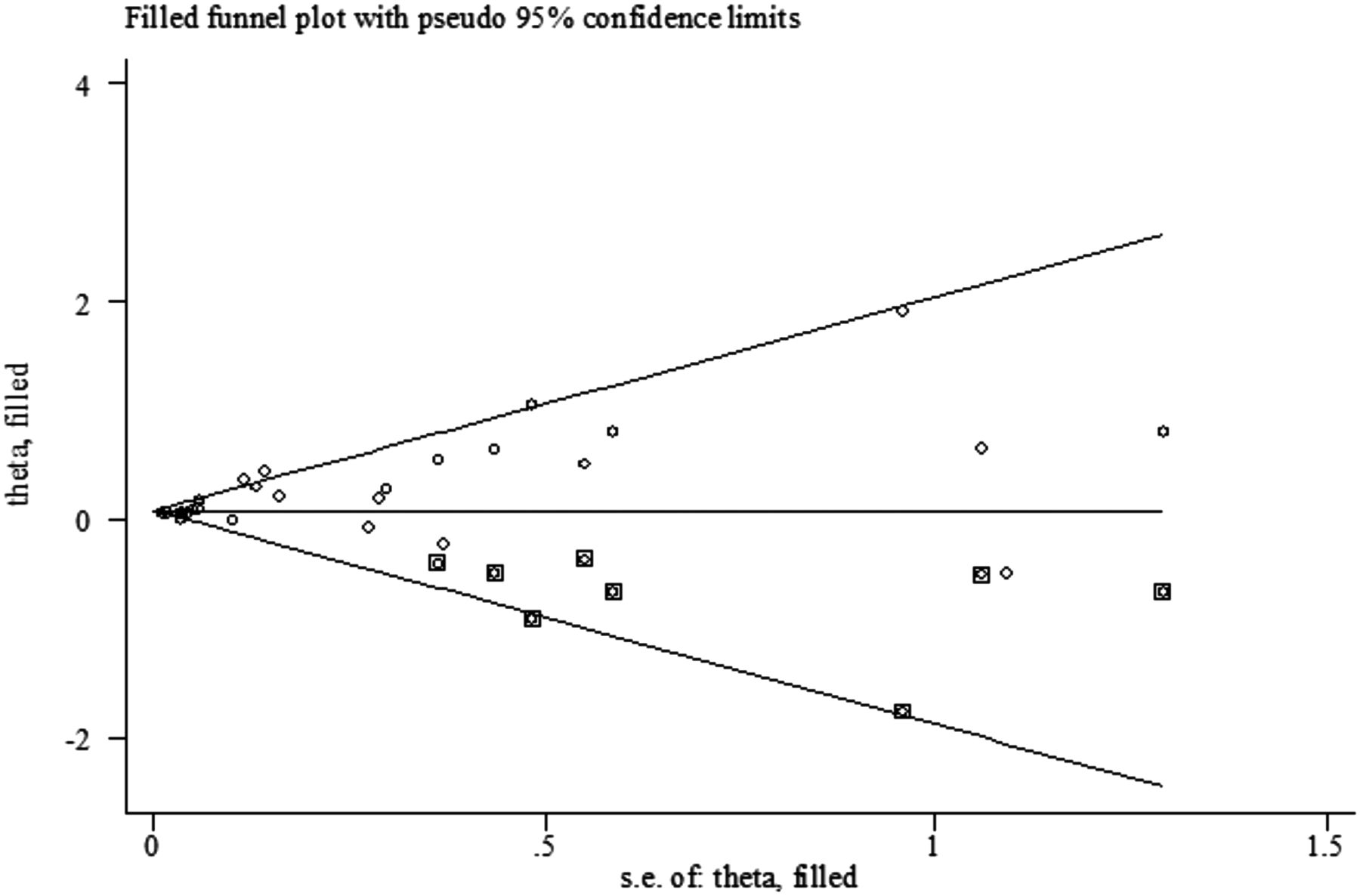
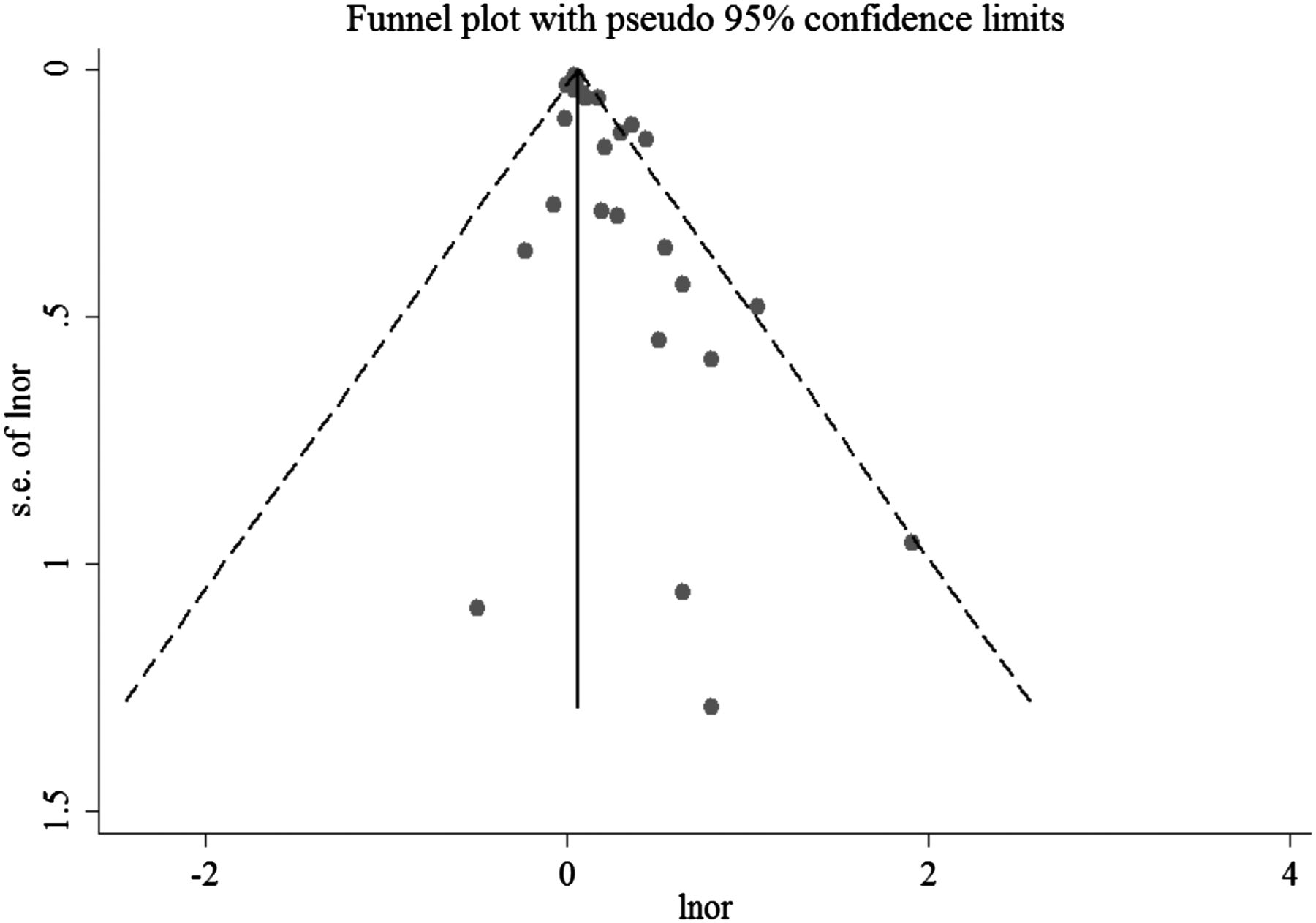
Visual inspection of the funnel plot showed some asymmetry (see figure 3). The Egger test suggested evidence of publication bias, but the Begg test did not (Egger, p=0.002, Begg, p=0.072). Using the trim-and-fill method to assess the impact of any potential publication bias, we found that eight potentially missing studies would be needed to obtain funnel plot symmetry for DM (see figure 4). The corrected OR using the trim-and-fill method was 1.08 (95% CI 1.05 to 1.12; random-effects model, p=0.006). Correction for potential publication bias therefore did not materially alter the pooled OR.
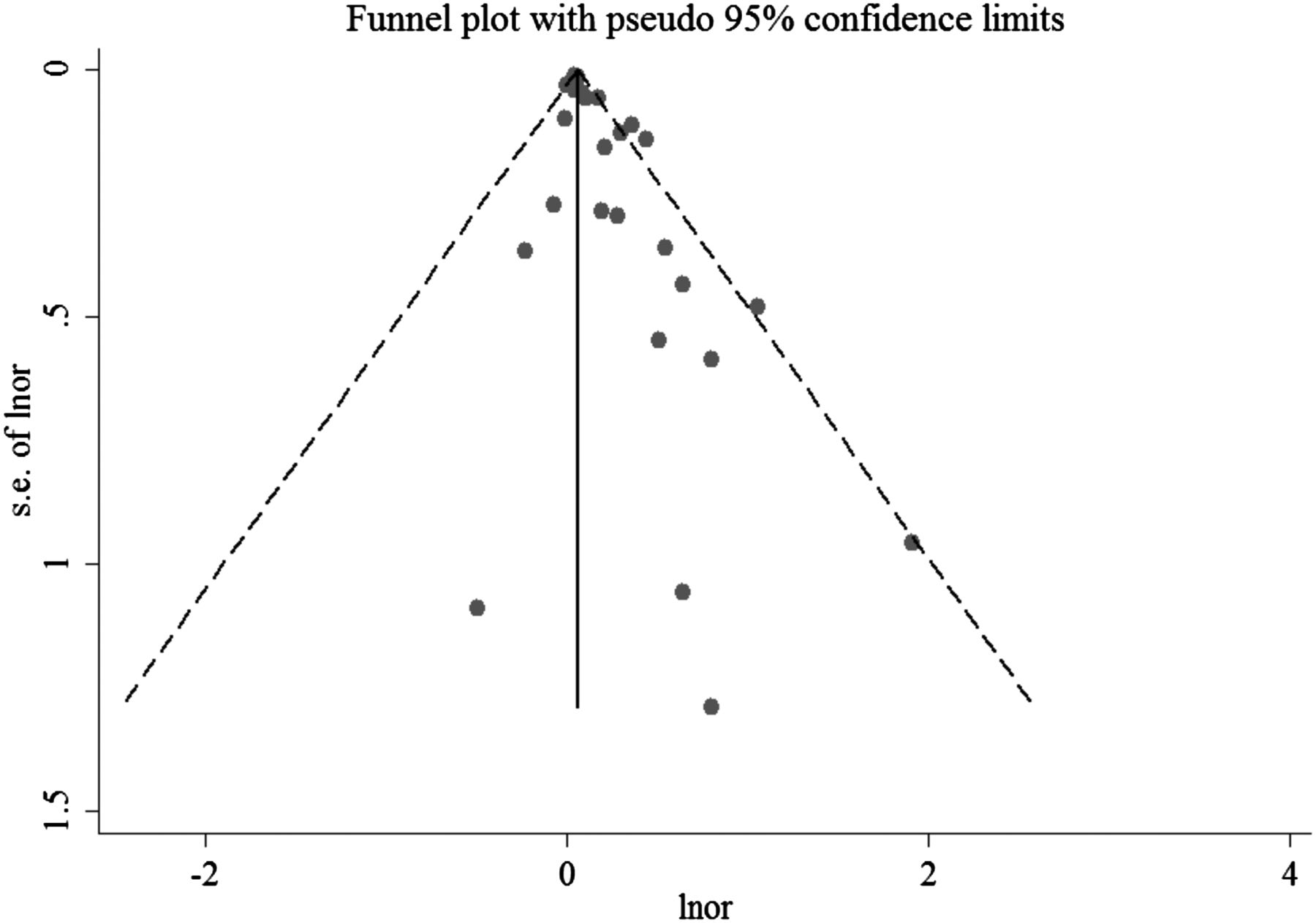
Funnel plot for studies of shift work in relation to diabetes mellitus risk. The horizontal line represents the summary effect estimates, and the dotted lines are pseudo 95% CIs.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Filled funnel plot of OR from studies that investigated the association between shift work and the risk of diabetes mellitus. The circles alone are real studies and the circles enclosed in boxes are ‘filled’ studies. The horizontal line represents the summary effect estimates, and the diagonal lines represent pseudo-95% CI limits.
Discussion
The meta-analysis of 12 observational studies with 28 independent reports including 226 652 participants (14 595 patients with DM) confirmed a positive association between shift work and DM. Compared with individuals who had never been exposed to shift work, the risk of DM was increased by 9% for shift workers. Furthermore, the association remained significant in most subgroup analyses.
Our subgroup analyses obtained two valuable and important findings. First, that the pooled OR for workers with rotating shifts (1.42, 95% CI 1.19 to 1.69) is clearly higher than that for other shift groups. We did not conduct a dose–response analysis because of limited information in the original studies. Nevertheless, because the frequency of the rotating shift schedule is much higher than that of the other shift schedules, we could preliminarily speculate that the higher the frequency of shift work, the greater the DM risk. Of note, the rotating shift was more common in the type of schedules that forced shift workers to adjust their body functions according to the duty periods, making them unable to adjust their body to the sleep pattern changes.30 In most cases, the human body was exposed to continuous stress from attempts to adjust as quickly as possible to the varying working hours, but at the same time was frustrated by the continuous shift rotation.31 Consequently, the health effect on the rotating shift groups may be more profound and pronounced than for other shift groups, as we found in our subgroup analysis.
We also found that the pooled OR was higher for men (1.37; 95% CI 1.20 to 1.56) than for women (1.09; 95% CI 1.04 to 1.14)—an interesting phenomenon, for which the reasons are unclear. The result suggests that male shift workers should pay more attention to the prevention of DM, and provides a clue for future study of how the biological mechanisms of shift work and DM are affected by gender. These biological mechanisms are complex, and comprehensive research is needed. Some studies32–38 have suggested that hypoandrogenism is associated with insulin resistance and T2DM in men. The diurnal patterns of testosterone levels are controlled by the circadian timing system.39 The possible adverse effect of repeated disruption of the circadian system owing to shift work may influence androgen secretion through regulation of the hypothalamic-pituitary-gonadal axis, which could contribute to the greater DM risk in men than in women. Further population and laboratory studies are clearly warranted to investigate the potential biological mechanism and difference between the sexes.
In the subgroup analysis of study location, the association with shift work was much higher in European participants than in those from Asia and the USA, but the difference did not reach statistical significance (p for interaction=0.13). Thus, we found no difference of shift work in relation to DM risk between ethnic groups in our meta-analysis. To generalise this finding, more studies conducted in other populations from South America and Africa are needed.
Some potential biological mechanisms may explain the link between shift work and DM. First, shift work may interfere with the normal synchrony of the light–dark cycle, sleeping and eating patterns, which might cause a mismatch of circadian rhythms; it is already known that circadian disruption may accelerate the development of T2DM in diabetes-prone individuals.40 Second, shift work makes the workers change their bed time frequently,41 which leads to sleeping problems like poor sleep quality, followed by the disturbance of the chronobiological rhythms.42 ,43 Some studies have shown that insufficient sleep and poor sleep quality may develop and exacerbate insulin resistance.44–46
Evidence from epidemiological investigation has confirmed that shift work is associated with weight gain,47 increase in appetite and adiposity,48 ,49 which are major risk factors for T2DM. Additionally, other mechanisms have suggested that shift work might increase the risk of DM as for two reasons. First, by disturbing socio-temporal patterns as a result of working irregular hours, which might contribute to family problems, reduce social support and induce stress. Second, owing to unfavourable changes to biomarkers, such as cholesterol and other lipids, blood pressure and plasminogen.13 ,50
Our meta-analysis has several strengths. This is the first meta-analysis to systematically quantify the strength of association between shift work and DM. Second, we obtained some important findings that the increased odds of DM risk is much greater for men than for women and higher for groups with rotating shifts than for other shift groups.
A few limitations of our meta-analysis should be acknowledged. Although the shift work is relatively objective and specific, it was not clearly defined in most original studies, which might have affected judgement of the results. Second, different definitions for shift work exposure and DM outcome were used across studies, which might have introduced heterogeneity into the studies’ results. Finally, the limited information provided in the included studies precluded the possibility of a dose–response analysis.
It is worth mentioning that the sample in our meta-analysis was large—larger than that of the other studies combined—but the heterogeneity of our included studies is moderate. By subgroup analyses we found that rotating shift group and male shift workers are at higher risk of DM than other shift groups and female shift workers, respectively—a conclusion which could not be reached by observational studies. The findings have value for DM aetiology, and also enrich the functions of the meta-analysis.
For future studies, based on our findings, we suggest that first, investigators need to improve the standardisation of different shift schedules and outcome definitions, which would provide stronger research evidence. Second, more prospective and interventional studies are needed to explore the underlying mechanisms and to determine the cause and effect relationships of gender difference that link shift work and DM.
In conclusion, our meta-analysis suggests that shift work is associated with a significantly increased risk of DM, especially in men and groups with rotating shifts. Given the increasing prevalence of shift work worldwide and the heavy economic burden of DM, the results of our study provide practical and valuable clues for the prevention of DM and a study of its aetiology.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Files in this Data Supplement:
- Data supplement 1 - Online supplement
Footnotes
-
Contributors YoG and ZL conceived the study. YoG and CY searched and checked the databases according to the inclusion and exclusion criteria. ZL helped to develop search strategies. YoG and CY extracted the data and assessed their quality. YaG, CY, XT, HS, YC, XY, LL and SC analysed the data. XT gave advice on meta-analysis methodology. YoG wrote the draft of the paper. All authors contributed to writing, reviewing or revising the paper and read and approved the final manuscript. ZL is the guarantor of this work and had full access to all the data in the study and takes responsibility for its integrity and the accuracy of the data analysis.
-
Competing interests None.
-
Provenance and peer review Not commissioned; externally peer reviewed.