Article Text

Abstract
Objectives Asbestos is an inflammatory agent, and there is evidence that inflammatory processes are involved in the development of cardiovascular disease. Whether asbestos is a risk factor for cardiovascular disease has not been established. The objective of this study was to investigate cardiovascular disease mortality in a large cohort of workers occupationally exposed to asbestos.
Methods Cardiovascular disease mortality in a cohort of 98 912 asbestos workers, with median follow-up of 19 years, was analysed. Unadjusted and smoking-adjusted standardised mortality ratios (SMRs) were calculated. The association between indicators of asbestos exposure and mortality was analysed with Poisson regression models, for deaths occurring during the period 1971–2005.
Results Altogether 15 557 deaths from all causes, 1053 deaths from cerebrovascular disease and 4185 deaths from ischaemic heart disease (IHD) occurred during follow-up. There was statistically significant excess mortality from cerebrovascular disease (SMR: men 1.63, women 2.04) and IHD (SMR: men 1.39, women 1.89). Job and birth cohort were associated with the risk of cerebrovascular and IHD mortality in the Poisson regression model including sex, age, smoking status, job, cohort and duration of exposure. For IHD only, duration of exposure was also statistically significant in this model.
Conclusions Cerebrovascular and IHD mortality was significantly higher among these asbestos workers than in the general population and within the cohort mortality was associated with indicators of asbestos exposure. These findings provide some evidence that occupational exposure to asbestos was associated with cardiovascular disease mortality in this group of workers.
- Asbestos
- longitudinal study
- cardiovascular disease
- epidemiology
- pesticides
- cancer
- statistics
- mortality studies
- cross-sectional studies
- health and safety
- occupational health practice
- public health
- health surveillance
Statistics from Altmetric.com
- Asbestos
- longitudinal study
- cardiovascular disease
- epidemiology
- pesticides
- cancer
- statistics
- mortality studies
- cross-sectional studies
- health and safety
- occupational health practice
- public health
- health surveillance
Introduction
Inflammation plays a central role in the pathogenesis of cardiovascular disease.1 A substantial body of evidence exists, which demonstrates that long-term exposure to airborne particulate matter is associated with cardiovascular diseases and atherosclerosis.2 3 Inflammation, oxidative stress and the promotion of atherosclerosis have been observed in animal models exposed to airborne particulate matter,4 5 and cohort data exist linking airway inflammation with the risk of ischaemic heart disease (IHD).6 Asbestos also has a strong inflammatory effect and promotes atherogenesis in animal models.7–9 An increased risk of cardiovascular disease mortality associated with exposure to asbestos, as suggested in some exposed cohorts,10–13 could thus be a result of similar underlying mechanisms as for particulates even though the physical characteristics of asbestos fibres and particulates are different.
The primary focus of studies of asbestos-exposed workers tends to be on the major asbestos-related diseases, namely mesothelioma, lung cancer and asbestosis, and the majority of these studies have no information on cigarette smoking. Consequently detailed analysis of cardiovascular disease outcomes with adjustment for smoking have not typically been undertaken, although one study of Swedish shipyard workers exposed to asbestos has reported an age- and smoking-adjusted RR of IHD (3.1; 95% CI 1.5 to 6.4).14 Previous analysis of the British asbestos workers cohort found statistically significantly raised standardised mortality ratios (SMRs) for cerebrovascular disease (CD) and IHD,15 and a separate analysis of the removal workers in the cohort-indicated significant excess mortality from circulatory diseases.16 17 The objective of the current study was to undertake a detailed analysis of cerebrovascular and IHD mortality in relation to information on smoking behaviours and indicators of asbestos exposure among British asbestos workers.
Methods
In 1971, the Asbestos Workers Survey was established in order to monitor the long-term health of workers covered by regulations to control occupational exposure to asbestos. Details of the survey have been published previously.15 In brief, workers taking part in voluntary medical surveillance for the early detection of asbestos-related disease under the 1969 Asbestos Regulations were included in the survey, as well as workers undergoing regular statutory medical examinations as required by the 1983 Asbestos Licensing Regulations and subsequent regulations. At the time of the medical, workers were invited to participate in the survey and to complete the survey questionnaire. The questionnaire requested information on duration of occupational exposure to asbestos, current job type and smoking history. Information on job type and smoking history were updated for workers returning for further medicals. Workers, who agreed to take part in the survey, were flagged for death registrations with the National Health Service Central Register; 98% of workers were successfully traced. The British Medical Association Research Ethics Committee gave approval for the original survey.
Causes of death
The end points for the study were two forms of cardiovascular disease: CD (International Classification of Diseases (ICD) codes 430–438 for ICD-9 and codes I60–I69 for ICD-10) and IHD (ICD codes 410–414 (ICD-9) and codes I20–I25 (ICD-10)) mortality, identified through the underlying cause of death. Deaths occurring to the end of 2005 were included in the study.
Statistical methods
SMRs were calculated by sex-specific 5-year age and calendar time periods, using mortality rates for Great Britain (GB). The population attributable fraction due to smoking was calculated for the general population using the formula for multicategory exposures,18 published data on risks of mortality among current and former smokers relative to never-smokers19 20 and the average prevalence of smoking in the general population of Great Britain over the period.21 Smoking-adjusted SMRs could then be calculated using the formula given in Yu and Tse.22 Proportional mortality ratios (PMRs) were calculated to provide comparisons of mortality by job type within the cohort; PMRs rather than SMRs were used to show the relative importance of different causes of death in this cohort. Poisson regression was used to investigate whether potential indicators of asbestos exposure were related to cardiovascular disease mortality. Person-years at risk were calculated from the date of the first medical examination to the end of the study period, the date of death or the date of emigration, whichever was earliest. Four job types were used in the analysis: manufacturing, removal, ‘other exposed’ and insulation work. For the analysis, individuals were allocated to the job type they had spent most time in. Smoking status (current, former and never-smoker), age attained and duration of exposure were entered as time-varying covariates in the Poisson regression models. Relative risks of mortality were calculated within smoking categories, using predicted mortality rates from the Poisson regression models. For example, the mortality risk for a non-smoker aged over 70 years relative to that of a non-smoker aged <40 years and the mortality risk for a current smoker aged over 70 years relative to that of a current smoker aged <40 years were calculated. The models were checked for goodness of fit using Pearson's χ2 statistic.
Results
During the period 1971–2005, 99 680 men and women agreed to participate in the survey. After exclusions for incomplete data or unsuccessful flagging, 98 912 individuals were included in the analysis. There were 15 557 deaths from all causes, 1053 deaths from CD and 4185 deaths from IHD during the follow-up period (table 1). Over 55% of men and women completed only one survey questionnaire, and the median follow-up time was 19.3 years. The mean age overall at the first medical exam was 35 years; the majority of men were in the asbestos removal industry, while the majority of women were in the manufacturing industry. The proportional mortality ratios for lung cancer, asbestosis and mesothelioma differed substantially between the job categories: insulation workers (PMR lung cancer=131; PMR asbestosis=10 814; PMR mesothelioma=1828) and removal workers (PMR lung cancer=143; PMR asbestosis=4944; PMR mesothelioma=1398) had the highest PMRs, while ‘other exposed’ workers (PMR lung cancer=103; PMR asbestosis=2472; PMR mesothelioma=709) and manufacturing workers (PMR lung cancer=109; PMR asbestosis=1676; PMR mesothelioma=591) generally had the lowest PMRs. Over 58% of men and 52% of women were current smokers at the first medical examination and a slightly smaller per cent (55% and 49%, respectively) were current smokers at their last recorded medical (table 1). Attributable fractions for smoking were 16% and 20% for CD and 23% and 42% for IHD for men and women, respectively. The crude death rates for CD were 57 per 100 000 and 94 per 100 000 and for IHD were 238 per 100 000 and 181 per 100 000 for men and women, respectively.
Characteristics of the British asbestos workers (1971–2005)
SMRs and smoking-adjusted SMRs were calculated to compare mortality among the asbestos workers with those in the GB population (table 2). The SMR for all causes of death was 1.42 (95% CI 1.39 to 1.44). Overall, in unadjusted calculations, there were statistically significant excesses in cerebrovascular and IHD deaths in both men (SMR CD=1.63, 95% CI 1.52 to 1.73; SMR IHD=1.39, 95% CI 1.35 to 1.43) and women (SMR CD=2.04, 95% CI 1.64 to 2.51; SMR IHD=1.89; 95% CI 1.62 to 2.19). For never-smokers, the SMR for IHD was less than one among men but not so among women. The SMR for CD was elevated for female never-smokers, even though reference rates included smokers. The majority of the other SMRs were statistically significantly elevated.
Standardised mortality ratios for cerebrovascular and ischaemic heart disease among British asbestos workers (1971–2005)
Adjusting for smoking reduced the overall SMRs for both CD and IHD disease—as expected given the high rates of smoking in this cohort—and reduced the SMRs among smokers while increasing those for non-smokers. Nevertheless, all smoking-adjusted SMRs remained statistically significantly greater than 1, except for IHD among male never-smokers and CD and IHD among female former smokers which were not statistically significantly raised.
The Poisson regression analysis showed that, adjusted for age and smoking status, women had a similar risk of CD mortality as men (RR=1.04, 95% CI 0.84 to 1.30) but that women had a significantly lower risk of IHD than men (RR=0.55, 95% CI 0.47 to 0.64) (table 3). Adjusted for sex and smoking status, risk of mortality for both diseases increased rapidly with age: compared with workers aged <40 years, those aged 70 years or more had relative risks of 198 (95% CI 125 to 313) for CD and 256 (95% CI 186 to 354) for IHD. Relative to current smokers, adjusted for age and sex, the risk of mortality from both diseases was substantially lower for former smokers (RR CD=0.61, 95% CI 0.53 to 0.71; RR IHD=0.66, 95% CI 0.61 to 0.70) and never-smokers (RR CD=0.59, 95% CI 0.49 to 0.71; RR IHD=0.44, 95% CI 0.40 to 0.49).
Poisson regression analysis of cerebrovascular disease and ischaemic heart disease mortality in British asbestos workers (1971–2005)
Table 4 shows the associations between mortality and indicators of asbestos exposure in Poisson regression models adjusted for age, sex and smoking status. Associations were similar for the two diseases, but they tended to be stronger for IHD mortality. Compared with manufacturing workers, removal workers had significantly lower risk of mortality from both diseases (RR CD=0.74, 95% CI 0.60 to 0.90; RR IHD=0.72, 95% CI 0.65 to 0.79), whereas ‘other exposed’ workers had a lower risk of mortality from IHD only (RR IHD=0.86, 95% CI 0.79 to 0.94). However, the risks of CD and IHD mortality were similar for manufacturing and insulation workers. Mortality was inversely associated with year of birth and for IHD, there was a small increase in mortality with increasing occupational exposure to asbestos.
Poisson regression analysis* of cerebrovascular disease and ischaemic heart disease mortality in British asbestos workers (1971–2005)
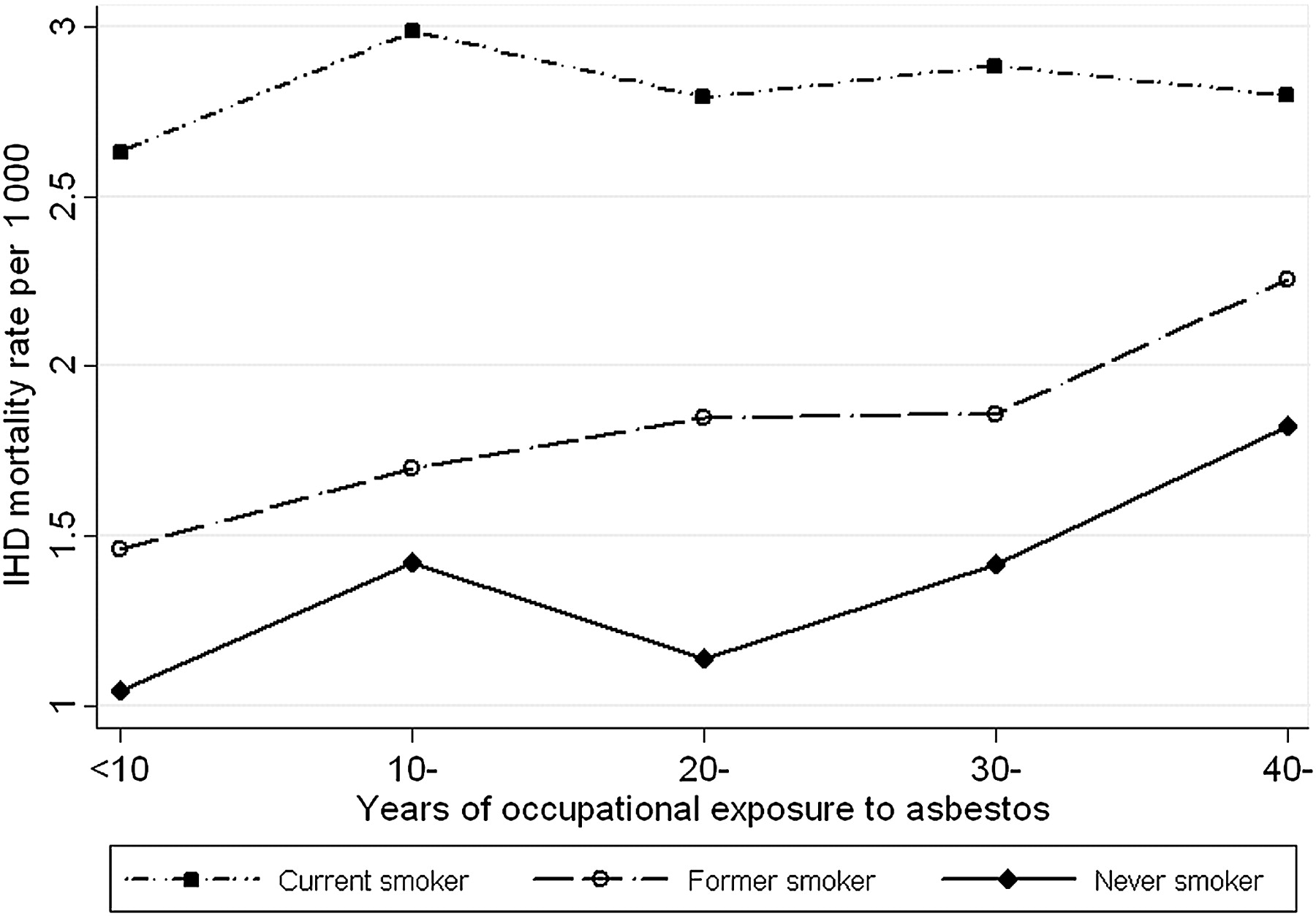
There was a statistically significant interaction between age and smoking status on IHD mortality (p<0.001) in the analysis adjusted for sex, job, year of birth and duration of exposure. Figure 1 shows IHD mortality rates by age and smoking category. Mortality increased with age in all smoking categories but more rapidly for never-smokers: for current smokers, the RR of IHD in those aged 70+ years compared with those aged <40 years was 37, whereas in never-smokers, it was 143. There was also a significant interaction (p=0.004) between duration of exposure and smoking status in the analysis adjusted for sex, job, smoking status and year of birth, which implied that the positive association between increasing IHD mortality and increasing duration of asbestos exposure was restricted to never- and former smokers (figure 2). The risk of IHD mortality for current smokers occupationally exposed to asbestos for 40 or more years was only 6% higher than for current smokers exposed to asbestos for <10 years. However, the risk of IHD mortality in former and never-smokers was, respectively, 54% and 75% higher in those exposed to asbestos for 40 or more years compared with former and never-smokers exposed to asbestos for <10 years. These interactions were not significant in the models of CD mortality.
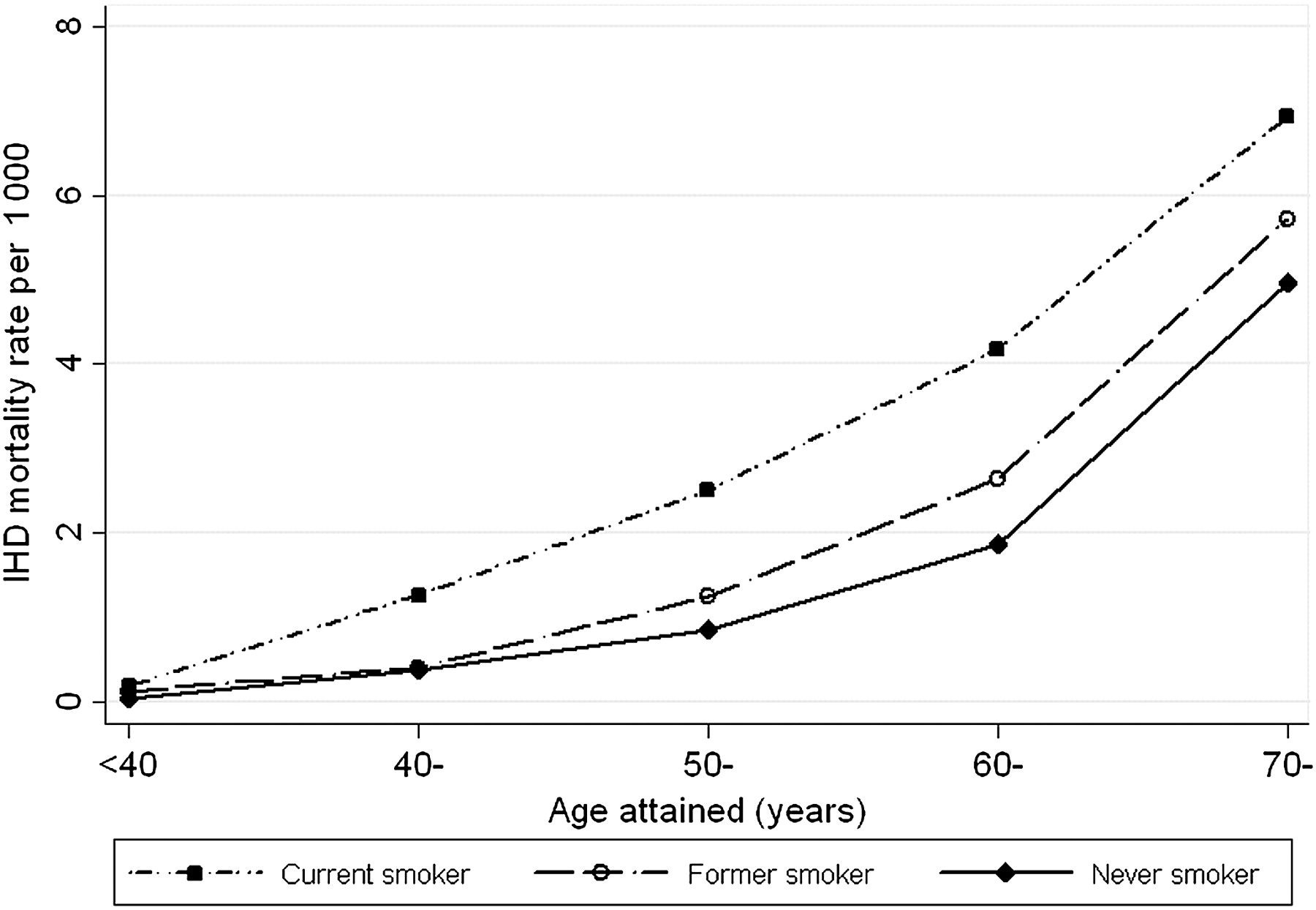
Ischaemic heart disease mortality by smoking status and age attained, adjusted for sex, job, birth year, and duration of exposure to asbestos.

{kind=link}
{kind=link}
Ischaemic heart disease mortality by smoking status and duration of exposure to asbestos, adjusted for age, sex, job, and birth year.
Discussion
There was evidence of increased cerebrovascular and IHD mortality in this large prospective study of asbestos workers with a median follow-up time of 19.3 years. Unadjusted and smoking-adjusted SMRs, comparing mortality among the asbestos workers with mortality in the GB population, showed a statistically significant excess of deaths among men and women for both cerebrovascular and IHD, both overall and, with a few exceptions, within each smoking status category. The SMRs for all causes and cardiovascular diseases were relatively high for an occupational cohort, but this has also been reported in a number of other asbestos-exposed cohorts.12 13 Higher mortality rates after adjusting for smoking may be attributable to exposure to asbestos, but they may also be at least partly attributable to occupational class. Compared with non-manual workers, manual workers have increased coronary heart disease incidence.23 Depending on socio-cultural context, different components of job strain, for example job control and skill dependency, and in some cohorts also lifestyle factors, may account for much of the difference in risk between occupational classes.23
There was also some evidence that the risk of mortality was positively associated with indicators of occupational exposure to asbestos; this was stronger for IHD. In Poisson regression analysis, the risks of CD and IHD were associated with job type and year of birth, and for IHD only, with duration of occupational exposure to asbestos. The evidence from studies of the effect of ambient air pollution is also stronger for IHD than for CD.24
Mortality was highest among current smokers. Our observation of a more rapid increase in IHD mortality with age among never-smokers than among current and former smokers, which corresponds to a decline with age in the RR for smokers compared with non-smokers, has been observed in other studies.25 This is likely to be due to the fact that mortality from IHD, a multi-factorial condition, is generally a major cause of mortality among older age groups.25 The interaction between duration of occupational exposure to asbestos and smoking status implies that the mortality rate was positively associated with duration of exposure among never and former smokers, but there was a negligible increase in risk with increasing duration of exposure among current smokers. If true, this suggests that the effect of occupational exposure to asbestos was greater on never- and former smokers than on current smokers and would suggest that the excess of IHD seen among smokers in this cohort after adjusting for smoking was largely a consequence of other factors. However, smoking cigarettes is associated with chronic, systemic inflammation and vascular inflammation,26 and thus, the effect of smoking may have masked any effect of asbestos on cardiovascular risk among current smokers within this cohort.
The main limitation with this study was the lack of information on individual exposure to asbestos, so that proxy measures of exposure had to be used. The effect of birth cohort represented overall working conditions, which tended to be dustier and less well controlled in earlier times. However, the cohort effect, which highlighted the lower risk of cardiovascular disease mortality in the later birth cohorts, may also reflect the general fall in cardiovascular disease mortality in the British population during the study period. Duration of exposure was derived assuming that an individual was exposed from the date they reported being first occupationally exposed until the date they stopped working in a job covered by the asbestos regulations. However, exposure may have been intermittent, and there was no indication of the intensity of exposure or of the type of asbestos involved. The job categories provide some information on the intensity and type of asbestos a worker was exposed to, but they take no account of differences between individual tasks within the job categories. The PMRs for lung cancer, asbestosis and mesothelioma by job category provide some insight into exposures overall; the relative sizes of PMRs are likely to reflect differing responses to exposure for each disease and different patterns of exposure within industry sectors. Manufacturing workers had lower asbestos-related disease risks than other sectors but a higher risk of IHD; this could be a reflection of lower intensity but longer duration exposures in this sector. Conversely, removal workers had among the highest PMRs for lung cancer, asbestosis and mesothelioma but the lowest risk of IHD. The asbestos removal industry is a relatively recent development and removal workers tended to be younger on entry into the study than workers in the other sectors; these two factors may in part account for their lower risk of cardiovascular disease mortality. Changes in the regulation of asbestos during the follow-up period completely altered the nature of the asbestos industry: use of amphibole asbestos was virtually eliminated by 1980 and by 1990, the insulation and manufacturing sectors no longer existed and asbestos removal work dominated the industry. Despite limitations in the variables representing asbestos exposure, statistically significant associations between these variables and mortality levels were observed in this study.
A major strength of the study was the availability of data on cigarette smoking, an important inflammatory agent and a risk factor for both diseases considered. This allowed confounding by smoking status to be controlled for in the analyses. The analysis showed that the increase in risk of IHD with age and with duration of exposure to asbestos was greater among never-smokers than among current smokers. Never smoking tends to be clustered with other healthy lifestyle choices,27 28 many of which are associated with a reduced risk of IHD. The finding that never-smokers' risk of IHD increased more rapidly with increasing duration of exposure than that of current smokers may provide some evidence of an association between asbestos exposure and IHD mortality, possibly through an inflammatory pathway, independent of any effects of cigarette smoking.
Conclusion
The findings from this study provide some evidence of an association between occupational exposure to asbestos and cardiovascular disease mortality in these workers.
References
Supplementary materials
Read the press release for this article
Read the press release for this article
Files in this Data Supplement:
- Read the press release for this article - Read the press release for this article
Footnotes
Funding This publication and the work it describes were funded by the Health and Safety Executive (HSE). Its contents, including any opinions and/or conclusions expressed, are those of the authors alone and do not necessarily reflect HSE policy.
Competing interests None.
Patient consent Obtained.
Ethics approval British Medical Association.
Provenance and peer review Not commissioned; externally peer reviewed.