Article Text

Abstract
Objectives The purpose of this study was to review the literature on the content of interventions focusing on return to work, employment status, or work retention in patients with cancer. Furthermore, the effect of the interventions on return to work was assessed in studies reporting return to work.
Methods A literature search was conducted using the databases MEDLINE, PsycINFO, EMBASE and CINAHL. Articles that described a work-directed intervention focusing on return to work, employment status, or work retention in patients with cancer were included. The content of the work-directed part of the interventions was assessed based on two criteria for content analysis: 1. does the setting fit the shared care model of cancer survivor care? 2. Does the intervention target work ability and physical workload? For studies reporting return-to-work outcomes, the return-to-work rates were assessed. For studies that used a control group the ORs and the 95% CIs were calculated.
Results Twenty-three articles describing 19 interventions met the inclusion criteria. Seven studies reported return-to-work outcomes of which four used a control group. Only three interventions aimed primarily at enhancing return to work or employment status. The most frequently reported work-directed components were encouragement, education or advice about work or work-related subjects (68%), vocational or occupational training (21%), or work accommodations (11%). One intervention fit the shared care model of cancer survivor care and five interventions enhanced work ability or decreased physical workload. The rate of return to work ranged from 37% to 89%. In one of the four controlled studies the intervention increased return to work significantly and in the other studies the results were insignificant.
Conclusions Only few interventions are primarily aimed at enhancing return to work in patients with cancer and most do not fit the shared care model involving integrated cancer care. Future studies should be developed with well-structured work-directed components that should be evaluated in randomised controlled trials.
- Cancer
- cancer survivor
- return-to-work
- (vocational) rehabilitation
- interventions
- OH services
- sickness absence
- intervention studies
Statistics from Altmetric.com
- Cancer
- cancer survivor
- return-to-work
- (vocational) rehabilitation
- interventions
- OH services
- sickness absence
- intervention studies
What this paper adds
Return to work is seen by cancer survivors as an important part of recovery. However, the risk of becoming unemployed is 37% higher for cancer survivors in comparison with healthy controls.
Most work-directed interventions are not primarily aimed at enhancing return to work or employment of patients with cancer.
Most frequently reported work-directed components of the included studies are: occupational training, encouragement, work advice, work accommodations, or education.
Very few work-directed interventions have studied the effect on return to work.
Future studies should be designed to include well-structured work-directed components and should have high methodological quality.
Introduction
Survival rates of cancer have increased in recent years as a result of screening, earlier and better diagnosis, and advanced treatment.1 It is generally assumed that the incidence of cancer in the working population in Western countries will increase due to the ageing of the working population and the trend that people have to work longer until their retirement.2 As a consequence, patients with cancer and cancer survivors will become more common in the workplace.
One of the aspects of quality of life is the preservation of work or return to work,3 which is decreased in cancer survivors as compared with cancer-free controls. Loss of work may result in a lower quality of life, lower self-esteem, and financial losses.4 In contrast, working gives a sense of normalcy, distraction, and is seen as an important part of recovery by cancer survivors.5 6 Not being able to work is not only a loss for cancer survivors, but also for the employer and society at large due to absenteeism and lost productivity.7
Earlier research showed that not all cancer survivors who were working prior to their diagnosis do return to work. In their review, Spelten et al found a mean return-to-work rate of 62% (ranging from 30% to 93%).8 Furthermore, cancer survivors who do (partly) return to work still have a greater level of work limitations and suffer from loss of productivity in comparison with the general population.9–11 In addition, some patients with cancer experience job discrimination, hostility in the workplace, lack of emotional and practical support from managers and from occupational health services, and become involved in disputes on terms of employment.7 12–14
Interventions to support cancer survivors in solving these work-related problems are needed. The International Classification of Functioning (ICF) offers a theoretical framework for developing interventions, whereas three opportunities for interventions are provided: 1. improving body structure and functioning, 2. improving environment-related factors, and 3. improving person-related factors.15 16 Better treatment of cancer and management of cancer-related problems such as fatigue will improve body structure and functioning, with a subsequent improvement in disabilities and work functioning. Interventions to adapt the work environment and interventions to improve person-related factors such as thoughts and expectations regarding return to work will have a potential for preventing long-term disability as well.7 8 17 Cancer treatment is well studied, however, work-directed interventions to improve work functioning are not. A review, studying the effects of interventions in patients with breast cancer with return to work as an outcome found only four studies of low methodological quality.18 More information on the characteristics of work-directed interventions, for all patients with cancer, is needed to further develop interventions that can help patients with cancer with their return to work.
Therefore, the aim of this study was to review the literature on the content of interventions focusing on return to work, employment status, or work retention in patients with cancer. Furthermore, the effect of the interventions on return to work was assessed in studies reporting return-to-work outcomes.
Methods
A review protocol has been made in which the search strategy, article selection and data extraction were taken into account. The Preferred Reporting Items for Systematic Reviews (PRISMA statement) have been used as formal systematic review guidelines.19
Search strategy
The following databases were searched: MEDLINE (PubMed), PsycINFO (ERL Webspirs/Ovid), EMBASE (Ovid) and CINAHL (EBSCO), with no restriction on language or on publication year but restricted to human studies (until October 2008). The following main medical subject headings were used: neoplasms AND intervention studies AND (vocational) rehabilitation. These medical subject headings were completed with text words and synonyms for neoplasms, work-directed terms, and intervention studies. To exclude irrelevant articles on occupational exposure, occupational diseases, and palliative care, the search strategy was refined by introducing a number of medical subject headings as ‘not-terms’ (see appendix for the search strategy for PubMed).
Article selection
Articles were included if the following criteria were met: 1. patients were diagnosed with cancer at age≥18 years, 2. description of an intervention aiming at the improvement of return to work, employment status, or work retention through improvement of work-environment-related or person-related factors. Articles describing an intervention that were exclusively focused on improvement of body structure or functions were excluded. Article selection was performed in three steps. In the first step, articles were independently selected by two authors (ST and AdB) based on title and abstract. In the second step, full articles were retrieved and included if the inclusion criteria were met. Articles in a language other than English, Dutch or German were translated by an expert. In the third step, the reference lists of the selected articles and of the selected reviews were hand-searched for additional references, and experts were asked to recommend relevant articles. In cases of disagreement, a third author (MF) decided if the article met the inclusion criteria.
Data extraction
The data were extracted by one author (ST) onto a pre-designed data extraction form and checked by another (AdB or JV). In cases of disagreement, a third author (MF) decided which data were correct.
Criteria for content analysis
The content of the work-directed components of the interventions were assessed based on two criteria for content analysis. The first criterion considered if the setting in which the intervention was carried out fitted the shared care model for survivor healthcare.20 According to this model, the oncologist provides cancer therapy in the early phase and the primary care physician takes over survivorship care after 1 or 2 years. They communicate with each other during all times and transfer knowledge periodically. For countries where an occupational physician is involved, we assumed a similar role for them as for the primary care physician. The model addresses both return to work in an early phase and improved communication which is beneficial for return to work.21
The second criterion was if the intervention included measures to improve self-perceived work ability and adapt physical workload which are the most important amenable prognostic factors for return to work in patients with cancer.17 22
Effect of the interventions on return to work
For those studies that reported return-to-work outcomes the characteristics of the study design and return-to-work outcomes were extracted. The return-to-work outcome was based on the number of patients who worked at the start of the study and who were employed but not on sick leave at follow-up. Furthermore, the ORs and 95% CIs for not returning to work were calculated if a study used a control group. These data are presented as a forest plot using the software implemented in the software program RevMan5.23
Methodological quality assessment
The methodological quality of the articles, which included return-to-work outcomes, was assessed using the Methodological Index for Non-randomised Studies (MINORS).24 The MINORS consists of 12 items of which each item can receive a score of 0–2 points, resulting in a maximum score of 24 points. Four of these items are only applicable in case of an article which used a control group. The quality assessment was conducted by two authors independently (ST and AdB). In cases of disagreement, a third author (MF) decided which score was correct.
Results
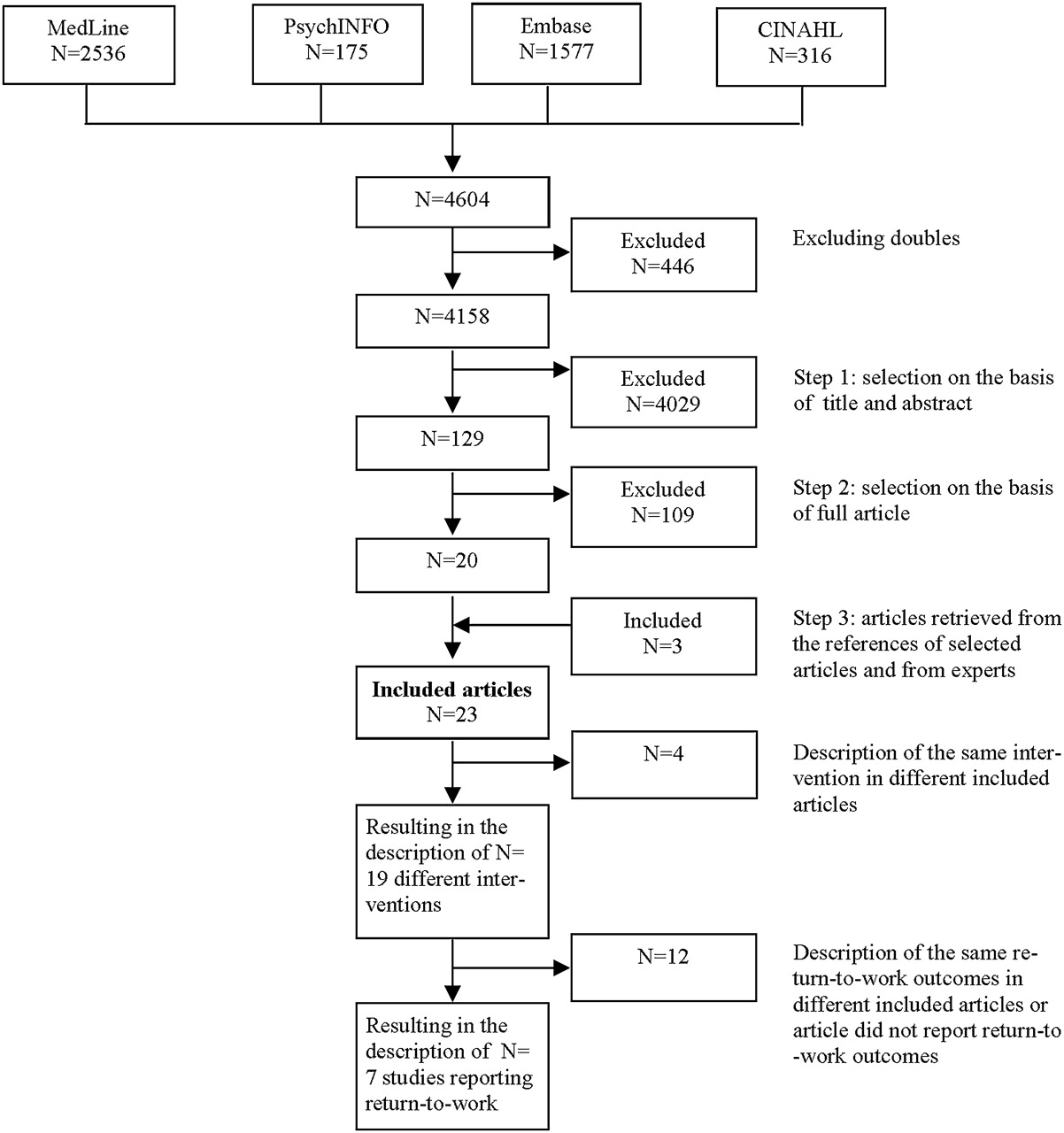
The search yielded 4606 articles and after excluding for doubles, 4158 articles were identified (figure 1). Based on title and abstract, 4029 articles were excluded mostly because the intervention was not focused on return to work, employment status, or work retention or because the article did not involve an intervention. Of the 129 remaining articles, 20 articles were included after reading the full text. The other 109 articles were excluded because in 75 articles the intervention was not focused on return to work, employment status, or work retention; in 30 articles there was no intervention; and in five articles the content of the intervention was not described or the intervention did not contain a work-directed component. Three additional articles were identified through the references of the selected articles and selected articles from experts. The references of 10 selected reviews did not reveal new articles. This resulted in 23 articles that were included in this review.5 25–46 Two interventions were reported twice,31 32 44 45 and one intervention was reported three times,25–27 resulting in the description of the content of 19 different interventions.5 25 28–31 33–43 45 46 Furthermore, of the 23 articles, seven studies reported return-to-work outcomes25 26 28 32 37 38 41 of which four used a control group.25 26 28 38

Article selection.
Study and patient characteristics
Table 1 summarises the author(s), publication year, country, and patient characteristics of the 23 included articles. Ten articles (43%) were published more than 15 years ago while 10 articles (43%) were published in the last 5 years. The included articles were conducted in the USA (39%), Scandinavia (26%), the Netherlands (22%), Germany (9%), and the UK (4%). Female patients with cancer were studied most, with seven articles (30%) composed exclusively for patients with breast cancer, and in another nine articles (39%), breast cancer was the most common diagnosis. Furthermore, one article (4%) was composed exclusively for male patients with cancer aiming at patients with prostate cancer. Three articles (13%) included patients with non-metastatic cancer only, and one article (4%) included both patients with metastatic as non-metastatic cancer. Of the remaining 19 articles (83%) the disease status was either unknown or another kind of eligibility criterion was used, such as life expectancy. The mean age of the patients in the included articles was 48±6 years.
Study and patient characteristics
Content of the interventions
Table 2 summarises the characteristics of the 19 interventions and the content of the work-directed part of the intervention. Only three interventions (16%) focused primarily on improving work outcomes. Of these, two (11%) focused on return to work,5 41 and one (5%) on employment status.29 Of the other interventions, 15 (79%) aimed more broadly at improving quality of life and/or general functioning,25 30 31 33–40 42 43 45 46 and one (5%) aimed at improving psychosocial symptoms.28 Six interventions (32%) were at least partly carried out in an inpatient setting,28 33 38 39 42 43 while 13 interventions (68%) were carried out in an outpatient setting. The start of the rehabilitation programme varied from before treatment,28 to several years after diagnosis.43 In six interventions (32%) follow-up care was provided by telephone or face to face.5 31 38 40 42 43 One programme (5%) was entirely carried out in groups,25 eight programs (42%) were carried out entirely on an individual basis,5 28 29 38–42 and 10 interventions (53%) were carried out both individually and in groups.30 31 33–37 43 45 46
Characteristics of the work-directed part of the interventions
All interventions consisted of more than one component. Thirteen interventions (68%) were a combination of counselling and education, usually carried out by a nurse, a social worker or a psychologist.5 25 31 34–38 40 42 43 45 46 Six interventions (32%) had an additional component of physical exercise, usually carried out by a physical therapist.25 31 34–36
Content of the work-directed components of the interventions
The work-directed components are divided according to the ICF model into person-directed intervention components and environment-directed intervention components. Since some interventions have more than one work-directed component, the total number exceeded the 19 interventions.
Person-directed intervention components
In 13 interventions (68%), the work-directed component consisted of encouragement, education such as educational leaflet, counselling or advice about work or work-related subjects, or topical discussion of work in a group session.5 28 30 33–35 37 38 40–42 45 46 In three interventions (16%), the intervention engaged the participants more by means of coping skills training, discussing the relationship with co-workers, and the learning of applying self-management skills in striving for personal goals such as work.25 31 36
Environment-directed intervention components
The environment-directed intervention components consisted of one intervention each of work which corresponds with the needs of rehabilitation and of change of job,37 gradual return to work with limited work hours and of workplace training/vocational aid,33 the sending of two letters from the treating physician to the occupational physician in order to enhance communication,41 and the speech pathologist or rehabilitation counsellor calls or visits the employer of the patients.39 In 13 interventions (68%),25 28 30 31 34–38 40 42 45 46 job demands were not taken into account and in 12 of these (63%)25 28 30 31 34–36 38 40 42 45 46 neither the workplace, nor the employer, nor the occupational physician, were part of the intervention.
Combination of intervention components
Three interventions (16%) consisted of a combination of person-directed and environment-directed intervention components. Clark and Landis conceived an intervention that consisted of prevention-anticipatory guidance such as strategies are selected to clarify misconceptions and myths related to cancer, restoration-rehabilitation counselling such as a comprehensive work re-entry plan and support-health maintenance consisting of for instance regular follow-up in the early phase of the re-entry process.5 The intervention of Chan et al consisted of state vocational rehabilitation services consisting of for instance vocational rehabilitation counselling, occupational/vocational training or job search assistance.29 The intervention of Sherer et al consisted of work site observation, volunteer job placement, assistance with returning to desired independence or productive activities, and therapist visits to the job site.43
Content analysis
Shared care model
One intervention (5%) fitted the shared care model completly,41 while eight interventions (42%) partly met this criterion. Of these, four interventions (21%) were integrated into normal cancer care, but, transition to a primary care physician or occupational physician did not take place.28 38 39 42 Four interventions (21%) were not integrated into normal cancer care but the transfer to the occupational physician or primary care physician did take place.5 29 37 43 The nine other interventions (47%) did not match the shared care model,25 30 31 34–36 40 45 46 and for one intervention (5%), it was impossible to determine.33
Work ability
In six interventions (32%), work ability was directly addressed by specific activities as coping skills training, vocational rehabilitation counselling and guidance or behavioural problem-solving therapy,25 29 36 by developing a strategy for information sharing about the cancer experience with co-workers, or by discussing the relationship with co-workers,5 31 or by assisting patients with returning to their desired productivity activities.43 Work ability was in 13 interventions (68%), only indirectly dealt with by addressing work in group sessions or by encouraging and giving advice, or information about return to work or work-related subjects.5 28 30 33–35 37 38 40–42 45 46 Work ability was not addressed in one intervention (5%).39
Physical workload
In two interventions (11%), physical workload was the focus of the work-directed component of the intervention and was done by making a return-to-work plan.5 41 Physical workload was addressed, in one intervention each by facilitating patients' use of a compensatory strategy,43 by change of job,37 by vocational aid,33 by retraining for another job,5 33 by assessing job requirements,5 or by training, on-the-job training/support and disability-related augmentative skills training.29 The physical workload was not addressed in 13 interventions (68%).25 28 30 31 34–36 38–40 42 45 46
Effect of the interventions on return to work
Table 3 summarises the effect of the interventions on return to work for the seven studies reporting return-to-work outcomes.25 26 28 32 37 38 41 The rate of return to work at follow-up in the intervention group ranged from 37% to 89% with a median of 76%. The return-to-work rates were collected by questionnaire (66%),25 26 32 semi-structured interviews (22%),28 38 41 or hospital reports (11%).37 Three studies were uncontrolled prospective cohort studies.32 37 41 Four studies used a control group25 26 28 38 of which only one used randomisation to assign the intervention.26 One study showed an OR significantly lower than 1,38 indicating that the intervention improved return to work (figure 2). The other three studies were insignificant.25 26 28 The methodological quality score of the seven studies that measured return-to-work outcomes was 15 (ranging from 9 to 18) of the possible maximum of 24. Prospective calculation of the study size (100%), adequate control group (57%), and adequate statistical analysis (57%) were mostly lacking.
The effect of the interventions on return to work of the seven studies reporting return to work

{kind=link}
{kind=link}
Forest plot of ORs and 95% CIs for not returning to work of the four studies that reported return-to-work outcomes and that used a control group.
Discussion
The aim of this study was to review the literature on the content of interventions focusing on return to work, employment status, or work retention in patients with cancer by intervening with a work-directed intervention on environment-related and/or person-related factors. Furthermore, the effect of the interventions on return to work was assessed in studies reporting return to work. The extensive search strategy yielded 23 articles which met the inclusion criteria in which 19 interventions were described. Seven studies reported the effect of the intervention on return-to-work outcomes. The most frequently reported work-directed components of the included interventions consisted of encouragement, education or advice about work or work-related subjects (68%), vocational or occupational training (21%), or work accommodations (11%). One intervention (5%) fit the shared care model of cancer survivor care and five interventions (26%) specifically addressed work ability or physical workload. The rate of return to work ranged from 37% to 89%. In one of the four controlled studies the intervention increased return to work significantly and in the other studies the results were insignificant.
Strengths/limitations
To our knowledge, this is the first review which systematically searched the literature for interventions focusing on enhancing return to work, employment status, or work retention for patients with cancer. A strength of this study is the extensive search of all relevant scientific databases and the lack of restrictions on publication year or language. Extending the review beyond the outcomes has the advantage that we can learn from the description of interventions which components are deemed effective by researchers or care providers. A limitation of this study is that the review has been restricted to work-directed interventions. It was, therefore, impossible to make inferences concerning the content and effect of interventions on return to work for cancer- or treatment-related complaints such as fatigue, distress, or speech problems.
Content of the work-directed components of the interventions
The content of the work-directed components varied widely, which indicates that a clear concept of work-directed interventions is lacking. The work-directed component was, in most interventions, small part and was not a structured part of the intervention, indicating that enhancing return to work, employment status, or work retention was not an important objective. Work-directed interventions in musculoskeletal disorders are more common. Here, there seem to be clearer ideas of which components the work-directed intervention should contain,47 such as the cognitive behavioural approach in graded activity,48 49 or ergonomic approaches.50
The majority of the interventions did not fit the shared care model for survivor healthcare because these interventions were either not carried out in the hospital in the first phase, were not carried out by the occupational physician or the primary care physician in the second phase, or communication and transfer of knowledge was not established. Therefore, new strategies to integrate return-to-work support in the current normal cancer care with active communication between providers needs to be developed. For patients with chronic rheumatic disease, such strategies have been developed and could be used as a model.51 The majority of the interventions did not address work ability or physical workload. In 11 interventions work ability was addressed by giving ‘simple’ advice or counselling which could lead both to an improvement (eg, patients who had had advice about return to work from their physician returned to work more often) or deterioration (eg, physician advising absence from work significantly increased sickness absence) of return to work.52 53 Vocational rehabilitation programmes in low back pain have taught us that education is less effective than problem-solving therapy added to graded activity.54 Problem-solving therapy addresses illness perceptions, which seem to be one of the causes of long sick leave in other chronic illnesses.15 This ‘simple’ advice has been given in seven interventions during a group session. A drawback of group sessions is that the constitution of the group determines the significance of discussing return-to-work problems.55 This means that it is important to discuss work issues at the individual level and preferably with a cognitive behavioural component such as has been done in the study of Korstjens et al or Nieuwenhuijsen et al.36 41 Furthermore, making a plan for employment and individual counselling/structural guidance in the study of Chan et al or making a comprehensive work re-entry plan in the study of Clark en Landis seems suitable as well.5 29
Physical workload was addressed by organising work accommodations. It is known that perceived workplace accommodations are an important factor for return to work and that employers, in general, are willing to carry them out for patients with cancer.56 The occupational physician seems the best suited person to implement these workplace accommodations.57 In more than half of the interventions, neither the workplace, nor the employer, nor the occupational physicians were part of the intervention. However, patients with cancer do need social support from their workplace, especially practical support from the supervisors and from their occupational health service.14
Effect of the interventions on return to work
The seven studies reporting return-to-work outcomes were of poor methodological quality; only one study was a randomised controlled trial. Due to large differences between studies concerning the content of the interventions, study population and study design it was not possible to pool data. Therefore, it was not possible to make an overall conclusion of the effect of the interventions on return to work. However, the intervention of Maguire et al and Capone et al can be compared considering the setting, the start and the content of the intervention and both ORs reveal positive effects for the intervention group.28 38 Even though these studies were non-randomised low-quality trials this indicates that work-directed interventions have the potential to improve work outcomes in patients with cancer. The only controlled trial that did favour the control group, however insignificant, was the study of Berglund et al in which assignment to care as usual was based on the refusal to participate in the intervention but agreement to be monitored.25 Apparently the participants judged correctly that their changes of return to work were so good that they did not need the intervention.
Implications for research
There is a need for improvement of interventions that support patients with cancer in their return to work. Improvement can be made by incorporating the shared care model and better addressing important prognostic factors such as self-reported work ability and physical workload. The small amount of information currently available suggests that successful interventions of this sort are feasible and potentially effective. The next step is to determine the effectiveness of such intervention on return to work in larger randomised controlled trials.
Appendix Search strategy for PubMed
(‘neoplasms’[MeSH Terms] OR cancer*[Text Word] OR neoplasm*[Text Word] OR carcinoma*[Text Word] OR oncology*[Text Word] OR leukemia*[Text Word] OR sarcoma*[Text Word] OR lymphoma*[Text Word] OR melanoma*[Text Word] OR radiotherapy[Text Word] OR chemotherapy[Text Word])
AND
(#‘treatment outcome’[MeSH Terms] OR ‘treatment outcome’[Text Word] OR ‘program evaluation’[MeSH Terms] OR ‘programme evaluation’[Text Word] OR ‘Intervention studies’[MeSH Terms] OR ‘Evaluation Studies as Topic’[MeSH Terms] OR ‘Process Assessment #Health Care#’[MeSH Terms] OR ‘Outcome Assessment #Health Care#’[MeSH Terms] OR ‘program development’[MeSH Terms] OR effect*[Text Word] OR control*[Text Word] OR evaluate*[Text Word] OR compare*[Text Word] OR program*[Text Word] OR outcome*[Text Word] OR intervention[Text Word] OR training[Text Word])
AND
(#Return to work[Text word] OR ‘employment’[MeSH Terms] OR employment[Text Word] OR retirement[Text Word] OR ‘sick leave’[MeSH Terms] OR sick leave[Text Word] OR Sickness absence[Text Word] OR ‘absenteeism’[MeSH Terms] OR absenteeism[Text Word] OR ‘job satisfaction’[MeSH Terms] OR ‘job application’[MeSH Terms] OR ‘work’[MeSH Terms] OR ‘occupations’[MeSH Terms] OR ‘occupational medicine’[MeSH Terms] OR ‘occupational health’[MeSH Terms] OR ‘occupational health services’[MeSH Terms] OR disability management[Text Word] OR ‘rehabilitation, vocational’[MeSH Terms] OR occupation*[Text Word] OR ‘rehabilitation’[MeSH Terms:noexp] OR ‘neoplasms/rehabilitation’[MeSH Terms] OR vocational*[Text Word] OR ‘Occupational Therapy’[MeSH Terms] OR ‘work ability’[Text Word] OR ‘work capacity’[Text Word] OR ‘work activity’[Text Word] OR ‘work attitude’[Text Word] OR ‘work cycle’[Text Word] OR ‘work disability’[Text Word] OR ‘work decrease’[Text Word] OR ‘work environment’[Text Word] OR ‘work health’[Text Word] OR ‘work life’[Text Word] OR ‘work performance’[Text Word] OR ‘work recovery’[Text Word] OR ‘work rehabilitation’[Text Word] OR ‘work research’[Text Word] OR ‘work status’[Text Word] OR ‘work responsibilities’[Text Word] OR ‘work satisfaction’[Text Word] OR ‘work shift’[Text Word] OR ‘work sick’[Text Word] OR vocational[Text Word] OR workability[Text Word] OR workplace[Text Word] OR ‘work stress’[Text Word] OR ‘work capacity evaluation’[MeSH Terms] OR employer[Text Word] OR employability[Text Word] OR employable[Text Word] OR unemployed[Text Word] OR ‘unemployment’[MeSH Terms] OR employee*[Text Word])
NOT
(#‘primary prevention’[MeSH Terms] OR ‘Neoplasms/prevention and control’[MeSH Terms] OR ‘Smoking/prevention and control’[MeSH] OR ‘smoking cessation’[MeSH Terms] OR ‘Smoking/adverse effects’[MeSH Terms] OR ‘risk factors’[MeSH Terms] OR ‘Risk Assessment’[MeSH Terms] OR ‘occupational exposure’[MeSH Terms] OR occupational exposure[Text Word] OR ‘occupational diseases’[MeSH Terms] OR occupational risk factor[Text Word] OR ‘protective clothing’[MeSH Terms] OR ‘inhalation exposure’[MeSH Terms] OR exposure[Text Word] OR exposed[Text Word] OR ‘Proportional Hazards Models’[MeSH Terms] OR occupational vitiligo[Text Word] OR ‘Antineoplastic Agents’[Mesh] OR ‘Molecular Structure’[Mesh] OR ‘Immunoconjugates’[Mesh] OR ‘Mutagenesis’[Mesh] OR ‘Apoptosis’[Mesh] OR apoptosis[Text Word] OR ‘Tumour Markers, Biological’[Mesh] OR ‘Signal Transduction’[Mesh] OR toxin[Text Word] OR toxin*[Text Word] OR toxic*[Text Word] OR toxic[Text Word] OR ‘Toxicology’[Mesh] OR ‘Carcinogens, Environmental/adverse effects’[MeSH Terms] OR ‘Mass Screening’[MeSH Terms] OR ‘Palliative Care’[MeSH Terms] OR ‘Neoplasm Metastasis’[MeSH Terms] OR ‘Mortality’[MeSH Terms] OR ‘aged, 80 and over’[MeSH Terms] OR ‘terminal care’[MeSH Terms] OR ‘geriatric assessment’[MeSH Terms] OR ‘ageing’[MeSH Terms] OR Childhood[Text Word] OR ‘child’[MeSH Terms] OR ‘gene expression profiling’[MeSH Terms] OR ‘attitude of health personnel’[MeSH Terms] OR ‘Radiology/education’[MeSH Terms] OR ‘Case Reports’[Publication type] OR ‘letter’[Publication type] OR ‘editorial’[Publication type] OR ‘Addresses’[Publication type] OR ‘Bibliography’[Publication type] OR ‘biography’[Publication type] OR ‘comment’[Publication type] OR ‘dictionary’[Publication type] OR ‘directory’[Publication type] OR ‘interview’[Publication type] OR ‘festschrift’[Publication type]).
References
Footnotes
Linked articles 051847.
Funding This study is granted by the Stichting Insituut GAK (SIG). Address: Borneolaan 27, 1217 GX Hilversum, the Netherlands, Email: info{at}instituutgak.nl.
Competing interests None.
Provenance and peer review Not commissioned; externally peer reviewed.