Article Text

Abstract
The aim of the study was to evaluate the evidence for an association between hip osteoarthritis (OA) and physical work demands. Systematic searches were made and epidemiological studies on hip OA and heavy lifting, including farming and construction work and climbing stairs, were reviewed for the period 1966–2007 inclusive. The quality of the studies was assessed and best-evidence syntheses of a causal relation between hip OA and physical demanding work have been made using specific criteria of the different degrees of evidence of causality. Limitations of the studies include few participants, use of different diagnostic criteria, and a poor description of the exposure. It is concluded that moderate to strong evidence was found for a relation between heavy lifting and hip OA. The burdens have to be at least 10–20 kg and the duration at least 10–20 years to give a clearly increased risk of hip OA. For farmers the risk of hip OA seems doubled after approximately 10 years of farming and the evidence is considered as moderate to strong. The evidence for a relation between hip OA for construction workers is limited and there is insufficient or no evidence that climbing stairs or ladders causes hip OA.
Statistics from Altmetric.com
Hip osteoarthritis (OA) is the most common reason for total hip replacement (THR) and a major source of disability in developed countries. Symptomatic hip OA occurs in 0.7–4.4% of adults.1–3 Hip OA can be inherited.4 Congenital dislocation, Legg-Calve-Perthe disease, slipped femoral capital epiphysis, body mass index (BMI) >25,5 major hip injuries,6 and some sports activities result in an increased risk of developing hip OA in later life.7–11
The aim of this study was to critically review the epidemiological evidence for a causal relation between hip OA and an exposure to heavy lifting, climbing stairs or ladders and exposure to heavy lifting combined with kneeling or squatting. The review is based on a scientific report12 made on behalf of the Scientific Committee of the Danish Society of Occupational and Environmental Medicine for the use of the Danish National Board of Industrial Injuries in their evaluation of whether knee OA and hip OA caused by physical work demands should be included on their list of occupational diseases that may be compensated through the Danish Worker Compensation act. The relation between knee OA and occupational work demands is presented in another paper.13
MATERIAL AND METHODS
The relevant studies were identified through searches in the following literature databases: MEDLINE (1966–May 2007), NIOSH-tic (1990–May 2007), EMBASE and HSEline (1990–May 2007). The following keywords were used: [Hip and (osteoarthritis or osteoarthrosis) and (work or occupation)]. Further relevant literature was found by screening the reference lists of all relevant articles identified.
A study was selected for a more detailed review if it fulfilled specific criteria described in Jensen, 2007.13 The diagnostic criteria for hip OA was: (a) radiological verified hipOA including radiological joint space narrowing (JSN) or the Kellgren and Lawrence criteria for hip OA; (b) a diagnostic code of hip OA (WHO International Classification of Diseases: ICD-8 = 713.00 or ICD-10 = M16 (hip OA)); (c) had a THR or (d) were on a waiting list for THR.
The quality of the studies, and the strengths and the weaknesses of the studies were evaluated according to the aspects outlined in Jensen, 2007.13 The quality assessment is shown in table 1.
The studies were considered to be heterogeneous with regard to the population studied, outcome measures for hip OA, and exposure measurement and it was therefore refrained to make statistically pooling of the data. There was instead carried through a “best evidence” synthesis5 14 according to the aspects described in Jensen, 2007.13
RESULTS
Identification and selection of literature
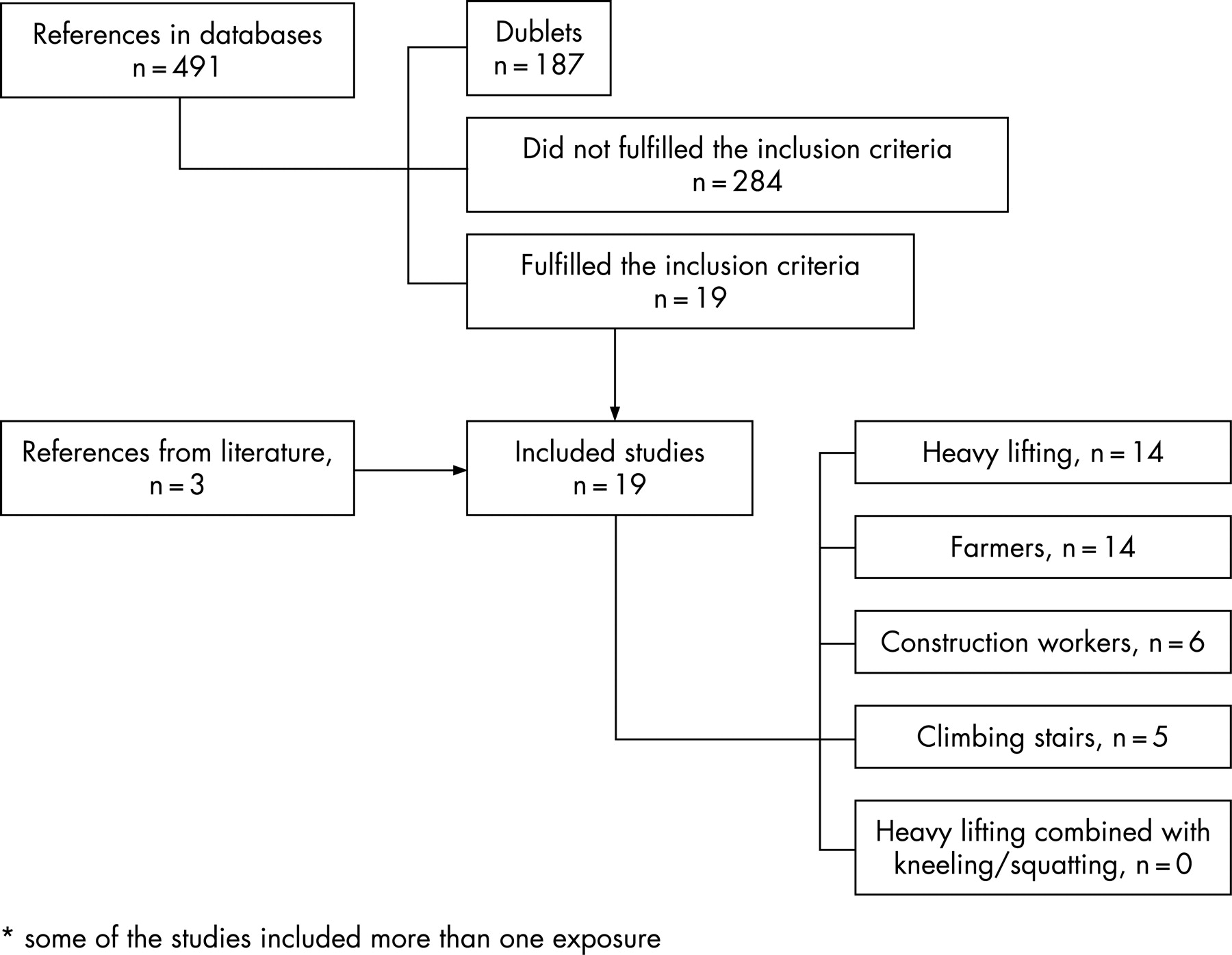
The electronic search retrieved a total of 491 references. Of these the 19 articles shown in table 1 met the inclusion criteria. Three articles were found in references of the retrieved literature. Of 22 articles, 14 studies investigated an association between hip OA and heavy lifting;15–29 14 studies investigated hip OA among farmers15 16 20 24 26 27 29–36 and six among construction workers.15 16 24 26 27 32 Five studies investigated the relation between hip OA and climbing stairs or working on ladders;15 16 21 28 29 and no study dealt with heavy lifting combined with kneeling/squatting. Figure 1 shows the results of the searches, and the number of epidemiological studies that remained after applying the inclusion criteria on the search.

{kind=link}
Description of the studies
Heavy lifting
Fourteen epidemiological studies focused on the relation between hip OA and heavy lifting (see table 2 for study details).
Twelve of 14 studies showed a significant association with an OR range of 1.97 to 8.5 or relative risk range (RR) of 1.5 to 12.4. Four studies were considered to be of the highest quality.15 16 18 25
In the case-control study by Vingaard et al25 233 men receiving the first THR were compared with 322 controls randomly selected from the study population. The workload was assessed by interview. Men with high exposure to heavy lifting, age 30–49 years, had a high risk of hipOA (RR 3.31, 95% CI 1.97 to 5.57) (results adjusted for age, BMI, smoking and sports activities). The strengths of the study were the specified exposure, the high number of participants, high participation rate, the description of the study and the analysis. Exposure was divided into three groups. Unexposed and the 5% lowest exposed were defined as low exposure, and medium and high exposure were divided into two equally large groups. This may lead to a risk of misclassification, and to a dilution of the results. 335 men, treated for myocardial infarction in the same hospitals, were also included to investigate possible recall bias in relation to the exposure measurement giving strength to the study. The differences between these men and men from the general population in relation to self-reported physical workload were very small and non-significant.
In a case-control study by Coggon et al15 cases comprised 210 men and 401 women placed on a waiting list for THR and 611 controls selected from the general population matched by age, sex and general practice. The exposure was estimated by interviews and specified for each job. Hip OA was more common in men lifting burdens of 10 kg before the age of 30 (OR 2.3, 95% CI 1.2 to 4.2) adjusted for potential confounders. No association with heavy lifting was shown in women. The strengths of the study were the high number of participants, the specified work demands, the description of the study and the analysis. A weakness was the participation rate. Of those who were invited to participate 84% of cases and 58% of controls were included in the analysis. This might lead to bias if subjects with heavy lifting were under-represented among the controls or if subjects with hip OA reported their past exposure more completely than the controls (recall bias).
Croft et al16 selected 60–75-year-old men who had had an out-patient intravenous urogram. 245 cases (THR or JSN <2.5 mm in at least one hip) were compared with 294 controls (JSN >3.5 mm). Exposure included lifetime occupational history with specified physical activity. Associations were found among severe cases (JSN <1.5 mm) and heavy lifting (OR 2.5 (95% CI 1.1 to 5.7)) (adjusted for age and hospital group). The strength of the study was the use of intravenous urogram. A bias which can be caused if cases with symptomatic hip disorders seek hospital treatment more often than the general population may be avoided by this selection method. The exposure measurement was defined as lift >25 kg. The frequency of lifting was not described. Many workers may lift 25 kg every day or week, and it is questionable if this criterion is sufficient to classify workers as subjects with heavy lifting. This may lead to a misclassification of non-cases as cases, most probably non-differential and thereby diluting the associations.
A cohort study by Flugsrud et al18 used data from a cardiovascular screening including 50 034 participants matched with nine years of national data on THR. During follow-up, 672 people had a first THR because of primary hip OA. Exposure data were collected by questionnaire during cardiovascular screening. The question was: “During the last year, have you had: mostly sedentary work; moderate (mostly walking); intermediate (walking and lifting); intensive (heavy manual labour)”. Intensive versus sedentary physical activity had an RR of 2.1 (95% CI 1.5 to 3.0) (men) and 2.1 (95% CI 1.3 to 3.3) (women). A large number of participants, high participation rate (92%) and the prospective design gave strength to the study. A weakness may be the exposure measurement. The information on physical work activity was collected during a 12-month period. This may not describe the physical activity during the whole work-life. The study included middle-age subjects. In general people have jobs with highest physical demands when young and still capable of lifting and carrying, and tend to change occupation to less heavy work as they get older. It seems likely that middle-aged workers with heavy work will also have had heavy work when younger. This may lead to a non-differential misclassification, and thereby dilute the associations.
Dose-response relation
There seemed to be a dose-response relation with higher risks for the high exposure groups (OR range 1.5–12)18 25–28 than for the medium exposed groups (OR range 1.1–4.1)18 25 26 28 compared with the low exposure groups. In three studies,15 21 29 there seems to be a dose-response relation with an increase in OR range of 1.2–1.9 for lifts of burdens >10 kg to OR range 1.5–2.7 for >25 kg and OR range 3.2–8.5 for >50 kg. The risk increased in relation to the amount lifted, with the frequency of lifting, and with the duration of lifted loads.
Farming
Fourteen epidemiological studies focused on the relation between hip OA and farming (see table 3 for study details).
Thirteen studies showed a significant increased risk of hip OA among farmers with an OR range of 1.98–12.0, an RR of 13.8 (one study) or an SHR of 273–286 (two studies). Four studies16 31 33 36 were assessed as being of high quality.
In the case-control study by Croft et al16 (already described) of 245 cases and 294 controls, farmers who had >10 years of employment showed a higher risk of severe hip OA compared with farmers with <1 year of employment, OR 2.0 (95% CI 0.9 to 4.4). No difference was shown for the farmers in total, or for farmers with 1–9 years of employment (OR 1.0). The number of farmers with severe hip OA who have worked as farmers >1 year was relatively small (n = 19), which may explain the non-significant differences.
Croft et al31 selected 1231 men, aged 60–76 years, from five rural practitioners at random. 890 (72%) answered questionnaires and 412 had worked as farmers or as office workers. Of those, 167 male farmers (cases) and 83 sedentary workers (controls) underwent x ray examination. The risk of hip OA was increased in farmers, especially in farmers employed >10 years (OR 9.3, 95% CI 1.9 to 44.5) (adjusted for age, height, weight and presence of Heberden’s nodes). One of the strengths of the study is the selection of the study population which in the primary questionnaire did not focus on farming or hip disease. Therefore farmers had no reason to reply more often than men from other occupations. The greatest limitation is the relatively low participation rate and the over-representation of symptomatic farmers (78%) compared with asymptomatic farmers (54%). Even though there had been no further cases of hip OA among the non-responding farmers, it could not explain the big differences between the cases and controls.
In a case-control study by Thelin et al33 269 cases of radiologically diagnosed hip OA (JSN <3 mm) were compared with 538 randomly selected controls matched for age, gender and place of residence. Radiological examinations of the pelvis and hip joint in a two-year period were re-evaluated. Farmers showed an increasing risk at increasing number of years of farming compared to controls: 1–10 years, OR 1.58 (95% CI 0.59 to 4.23); 11–20 years, OR 2.81 (95% CI 1.31 to 6.03); and 21–30 years, OR 7.35 (95% CI 2.87 to 18.82). By using radiological findings on previously taken x rays as case definitions, selection bias may be avoided which gives strength to the study. On the other hand farmers with heavy physical demands may seek medical treatment and have x rays taken because of hip symptoms more often than the general population, leading to selection bias. There is also the possibility that farmers may be less likely to consult hospitals if they live far from hospitals and traditions in the trade.
Tüchsen et al36 investigated four consecutive cohorts of all employed Danish men, aged 20–59 years with follow-up for five years in relation to hip OA. Exposure was classified by job title. Self-employed farmers had a SHR for hip OA of 286 (262 to 313) (only age-adjusted) (1994–9). The risk of hip OA showed a 0.14% average annual increase in the predicted SHR in the period 1981–99. The strengths of the study were that all first hospital admissions due to hip OA in Denmark were included, and the longitudinal design. A limitation may occur if farmers seek medical care because of hip pain more often than the general population (selection bias). Another limitation is the definition of hip OA (use of a diagnostic code) which is not as valid as radiological JSN (risk of misclassification), which may dilute the risk. The mean age for developing hip OA is approximately 60–65 years. Although this study includes relatively young subjects aged 20–59 years there may be a possibility of underestimation of the real risk. Farmers who had left their earlier occupation in farming because of hip OA were not included (healthy worker effect). This will probably have diluted the calculated risk which despite this showed significant results.
Construction work
The association between hip OA and construction work has been investigated in six studies. The study details are presented in table 4. Four of the six studies showed significant increased risk of hip OA with RR range of 1.66 to 7.0,26 27 OR 3.3,16 or SHR 151.32 Only the earlier described case-control study by Croft et al16 was evaluated as being of high quality. It showed significantly increased hip OA among workers with employment of 1–9 years (OR 3.3, 95% CI 1.2–9.2), but not for >10 years of employment (OR 0.5, 95% CI 0.1 to 2.3). The association between construction work and hip OA was not as strong as for farmers. This may be the result of inclusion of too few participants, and of misclassification of the workloads. There may be great differences between different kinds of construction work in relation to lifted burdens, in frequency and in weight.15 39 The results may therefore be diluted by only using the job title “construction workers”.
Climbing stairs or ladders
Five studies investigated the relation between climbing flights of stairs and hipOA (see table 5 for study details).
Three of the five studies showed significantly increased risk of hipOA with an OR range of 2.3 to 2.515 21 or RR of 2.1. Only the study by Croft et al16 was evaluated as being of high quality (described in detail earlier). It used radiographic OA as inclusion criteria. The association in this study was not statistically significant.
Best evidence synthesis
The studies were considered to be of high quality if the methodological quality score was >10.
Of 14 studies on the association between hip OA and heavy lifting, four reached the level of high quality.15 16 18 25 All these studies showed significantly increased risk of hipOA with an RR range or OR range of 2.3 to 3.3. One had a cohort design18 and three a case-control design. All studies showed a positive association, and for 12 of 14 studies the relation was significant. A number of studies with different design from several countries indicated an increasing risk of hip OA with an increasing degree of heavy lifting. All 14 studies showed a positive association. With regard to the various indices of heavy lifting, many studies showed a dose-response relation and it seemed that burdens should be at least 10–25 kg and the duration at least 10–20 years to give a clearly increased risk of hip OA. It is not possible to define corresponding thresholds for lifting frequency. Information bias with respect to exposure in case-control studies and selection bias in studies based on subjects having surgery may have occurred. There may also be a risk of misclassification with respect to x ray diagnoses in some studies, but as such misclassification is independent of exposure status the resulting bias would be to attenuate any real associations. For these reasons the evidence of a causal association between heavy lifting and hip OA is considered as moderate to strong.
Thirteen of 14 studies showed a significant increased risk of hip OA among farmers with an OR range of 1.98 to 12.0, an RR of 13.8 (one study) or an SHR of 273 to 286 (two studies). Of these, four studies reached the level of high quality.16 31 33 36 One had a cohort design36 and three had a case-control design.16 31 33 Three of the studies31 33 36 showed significantly increased risk for hip OA with OR range of 5.8 to 7.35 and an SHR of 286.36 A number of studies of different design from several countries indicate an increasing risk of hip OA with an increasing degree of years in farming. Information bias with respect to exposure may have occurred in case-control studies and selection bias in studies based on subjects having surgery. In relation to x ray diagnoses there is the same possibility for misclassification. For farmers the risk of hip OA seemed at least double after approximately 10 years of farming. For all these reasons the evidence of a causal association between farming >10 years and hip OA is considered as moderate to strong.
One high quality case-control study on construction workers was found.16 It showed a significantly increased risk of hip OA among construction workers (1–9 years), but no association for ⩾10 years. All studies showed a positive association, but only in two of the studies were the differences significant. Therefore the evidence for a relation is considered as limited.
Five studies investigated the relation between climbing stairs and hip OA.15 16 21 28 29 Three of five studies showed significantly increased risk of hip OA with an OR range of 2.3 to 2.515 21 or RR of 2.1. Only the study by Croft et al16 was evaluated as being of high quality. It used radiographic OA as inclusion criteria. The association in this study was not statistically significant. All were case-control studies. Information on exposure was collected retrospectively. In general, people with hip pain experience worse symptoms when climbing stairs. People in occupations which include climbing stairs may seek treatment earlier than other workers because of this pain. The case-control design may lead to a high risk of selection and recall bias in relation to stair-climbing. The evidence of a causal association is therefore considered to be insufficient. No studies investigated the relation between hipOA and climbing on ladders.
There is no information on the relation between hip OA and heavy lifting combined with kneeling or squatting. Thus, it is not clear if heavy lifting combined with kneeling/squatting is a stronger risk factor for hip OA than heavy lifting alone.
DISCUSSION
Study design and bias
This review may have some limitations including missing identification of relevant literature, publication bias of the literature, and the method of assessment of the quality of the studies. These limitations are described in detail elsewhere.13
Some of the problems with the included studies were related to few participants, use of different diagnostic criteria, and a poor description of the exposure.
Yoshimura et al29 and Lau et al21 carried out case-control studies in Japan and Hong Kong. The design was similar to the design used by Coggon et al.15 Among Japanese and Chinese subjects, and especially among male subjects, only a few have had THR, probably because of a lower prevalence of hip OA among Asians. The greatest limitation of these studies is the small number of included cases, especially of men. In spite of these factors, the results showed a positive association.
In studies such as Roach et al23 the greatest limitation was a high exclusion rate, where only 48% of the primary study population was used in the final analysis.
In some of the studies the results were only adjusted for age, but not for earlier traumas, BMI or other relevant confounders.26 27 32 33 35 36
The development of OA normally takes many years. Pain-disabled people who work in heavy lifting occupations and cannot meet the requirements for managing their physical job tasks may leave their trade (healthy worker effect); this underestimates risk, if only working people are included.18 32 Many of the studies in this field have also included people who were no longer working in their trade, thus avoiding the healthy worker effect.
Measurement of outcome
In eight epidemiological studies16 19 20 30 31 33 35 40 the diagnostic criterion for OA was JSN with the cut-off point ranging from 1.5–4 mm. There is no stringent definition of the cut-off point for JSN. Croft et al16 evaluated two definitions of JSN—2.5 mm and 1.5 mm. Only the more stringent cut-off point was clearly associated with other criteria, pain, other radiographic changes and occupational risk factors. Jacobsen et al41 showed an association between self-reported hip pain at a joint space width <2 mm.
When comparing different radiographic measures, minimal joint-space has in earlier studies been evaluated as the best radiological criterion of hip OA for use in epidemiological studies.42 43
THR or waiting for THR have been used as diagnostic criteria in six studies.15 18 21 25 29 34 and four studies used a diagnostic code for hospitalisation or getting a disability pension because of hip OA,26 27 32 36 which may lead to selection bias and an overestimation of a true risk. However the high risk is also reported in surveys which have been conducted in the general population and in subjects whose OA was found coincidentally on x rays taken for other purposes (urography, venography, angiography).20 24
Hip OA and gender
The association between hip OA and physical demands has been investigated for women in seven studies.15 17 18 21 27–29 The association was only significant in two of the studies, with OR range of 2.1 to 2.9.18 21 All studies revealed more significant results for men than for women. One of the explanations may be that many studies had too few female participants, and women traditionally work in different trades. It is not easy, therefore, to recruit a sufficient quantity of women with high exposure into the studies. The most plausible conclusion is that women are as susceptible to heavy work loads as men and that their risk of getting hip OA is equal to men if they have had the same exposure.
Exposure measurement
The heterogeneous nature of the exposure in many occupations, the variation over time and the long duration from first exposure to the development of OA makes it difficult to obtain relevant measurements of exposure. For these studies, the problems in relation to exposure measurements are the same as described by in a previous paper.13
Pathophysiological mechanisms
The pathogenesis of hip OA in relation to workloads has not been clarified. The forces that act on the hip in the standing position are one third of the body weight. When lifting 12.5 kg the weight increases to three times body weight, and climbing stairs increases the load to 5–7 times body weight.25 44 Obesity may increase the risk of OA by increasing the load on the weight-bearing joints45 or by changing the hormone balance. The last theory is supported by the fact that obesity also may increase the risk for hand OA.
Another hypothesis is that subchondral micro-fractures may induce OA.45 Micro-fractures may occur when the joint is in an extreme position or when physical workload exceeds a critical level.46 These studies indicate a possible pathophysiological mechanism by a mechanical effect and/or micro-fractures during repeated physical workload.
The precise mechanism for an association between hip OA and farming remains a subject for study. Degeneration of the hip may be caused by long-term heavy physical labour in farming. The potential risk factors also include exposure to vibration from tractor driving. These theories could not be confirmed in a study by Thelin et al35 where no relation between hip OA and “work as a farmer at a young age” or “tractor driving” could be confirmed. This may be explained by the fact that most farmers work with tractors and work at a young age and that these factors are something of a proxy for farming. In other studies it was confirmed that farmers have work involving lifting heavy loads, which may be the pathophysiological mechanism.15 16
CONCLUSION
Twelve of 14 studies with different study designs showed a significantly increased risk of hip OA in subjects with heavy lifting and 13 of 14 studies showed a significantly increased risk of hip OA in farmers. The best-evidence synthesis of a causal relation is considered as moderate to strong for both heavy lifting and farming.
There are relatively few studies (five) investigating the association between climbing stairs and hip OA. Although the studies showed a positive association, only some studies showed a significant risk. All studies had the same design, and no studies showed a dose-response relation. The evidence of a causal relation was considered to be limited (stair climbing) and there was no evidence for climbing on ladders.
There is no information on the relation between hip OA and heavy lifting combined with kneeling or squatting. Thus, it is not clear if the combination is a stronger risk factor for hip OA than heavy lifting alone.
Future research should focus on well-designed prospective cohort studies with adequate follow-up time, high quality studies on the risk of different workers in construction industry (for example, concrete workers, carpenters, bricklayers with high lifting demands in their trades) and studies on the dose-response relation with quantification of the amount lifted, frequency of lifting, and duration and amount of stair climbing. Furthermore, investigations are needed on: (1) new methods for outcome measurements (for example, MRI); (2) on exposure measurements for epidemiological studies; and (3) studies clarifying the pathophysiological mechanism of the development of occupational hip OA.
Acknowledgments
The study has been supported by the Danish National Board of Industrial Injuries. The author is grateful for the valuable support and comments from the two reviewers David Coggon and Stig Sonne Holm, and for the discussion in a one-day meeting and the comments during the final writing process from the Scientific Committee of the Danish Society for Occupational and Environmental Medicine including Sigurd Mikkelsen, Susanne Wulff Svendsen, Jørgen Olsen, Henrik Kolstad, Johan Hviid Andersen and Staffan Skerfving.
REFERENCES
Footnotes
Competing interests: None declared.