Article Text

Abstract
The models most commonly used, to study the effects of psychosocial work factors on workers' health, are the Demand-Control-Support (DCS) model and Effort-Reward Imbalance (ERI) model. An emerging body of research has identified Organisational Justice as another model that can help to explain deleterious health effects. This review aimed: (1) to identify prospective studies of the associations between organisational justice and mental health in industrialised countries from 1990 to 2010; (2) to evaluate the extent to which organisational justice has an effect on mental health independently of the DCS and ERI models; and (3) to discuss theoretical and empirical overlap and differences with previous models. The studies had to present associations between organisational justice and a mental health outcome, be prospective, and be entirely available in English or in French. Duplicated papers were excluded. Eleven prospective studies were selected for this review. They provide evidence that procedural justice and relational justice are associated with mental health. These associations remained significant even after controlling for the DCS and ERI models. There is a lack of prospective studies on distributive and informational justice. In conclusion, procedural and relational justice can be considered a different and complementary model to the DCS and ERI models. Future studies should evaluate the effect of change in exposure to organisational justice on employees' mental health over time.
- Industrial psychology
- organisational justice
- mental health
- absenteeism
- review
- epidemiology
- workload
- back disorders
- public health
- sickness absence
- risk assessment
- preventive medicine
- longitudinal studies
- intervention studies
- international occupational health
- stress
- musculoskeletal
- cardiovascular
Statistics from Altmetric.com
- Industrial psychology
- organisational justice
- mental health
- absenteeism
- review
- epidemiology
- workload
- back disorders
- public health
- sickness absence
- risk assessment
- preventive medicine
- longitudinal studies
- intervention studies
- international occupational health
- stress
- musculoskeletal
- cardiovascular
Introduction
Psychosocial stressors in the workplace, and their deleterious effect on mental health, have become an important public health issue.1–4 Prospective studies have identified some psychosocial factors leading to physical and mental health problems.1–3 5–7 Most of these studies preferentially used the Demand-Control-Support (DCS) model8 and Effort-Reward Imbalance (ERI) model.9 Previous systematic reviews on the effects of work stressors on mental health were limited to these models.4 However, a third model, the Organisational Justice (OJ) model, has been recently proposed.10 ,11 It has been argued that in today's rapidly changing work life, job control (from the DCS) may become less meaningful, as a result of the increased use of short-term contracts and the job insecurity that goes with them.12 In fact, the current developments in the labour market, the recent changes in work characteristics across a range of organisational contexts, and the emphasis on occupational equity may reflect the growing importance of underemployment, redundancy and forced occupational mobility.12 In this context, the OJ model, which has been found to be prospectively associated with physical health,5 ,13 may become increasingly important to employees' mental health.14 There are also some prospective studies on the effect of organisational justice on mental health,13 but no systematic review has been conducted. The extent to which this model is related to mental health disorders and is independent of the DCS or ERI factors therefore remains unclear. To help answer these questions, we will review both, the theoretical framework and empirical studies, on organisational justice and mental health.
Theoretical and empirical background for the organisational justice model
The organisational justice concept has developed out of a pre-existing conceptual framework called Adams' ‘equity theory’. According to Adams,15 ,16 individuals develop beliefs about what would be fair recognition for their work. Then, they compare themselves or someone else with a ‘referent’ in terms of the input/output ratio. A referent is another employee who is deemed to be equivalent in terms of duties and work status.16 The inputs are effort, time, skill, loyalty, tolerance, flexibility and integrity. The outputs are salary and bonuses, job security, recognition, reputation and responsibilities/promotions. In some situations, the comparison may lead to a perception of unequal treatment between an employee and one or more referent(s), which could in turn lead to potentially negative outcomes. Adams points to possible emotional and/or physical problems as evidence of a relationship between inequity/injustice and health.15
Organisational justice refers to the equity in the rules and social norms that govern companies, particularly in terms of ‘resources and benefits distribution (or distributive justice), processes and procedures conditioning that distribution (or procedural justice) and interpersonal relationships (or interactional justice)’. Interactional justice has two components: relational justice (degree of dignity and respect received from managerial authority) and informational justice (presence or absence of explanations from the managerial authority about new procedures).5 ,7
In theory, the OJ model can assess perceptions of workplace situations, even when the subject is not personally and directly concerned.15 This seems to be one of the differences, when compared with the DCS and ERI models, which measure perceptions of individual situations. Indeed, one might perceive a balance between its efforts and compensation (control or rewards), but still perceive injustice when compared with other employee of the workplace.
The concept of organisational justice has grown in use over the last two decades.5 ,7 The studies that had investigated this concept mainly focused on two components of organisational justice: procedural justice and relational justice. Organisational injustice measured as a single factor or by the above-mentioned components has been associated with adverse cardiovascular outcomes.17–20 There is an emerging body of empirical research investigating whether deleterious effects on mental health can be observed. This paper aims to produce a systematic review of these studies.
Objectives
-
To review prospective studies of the association between organisational justice and mental health in industrialised countries from 1990 to 2010.
-
To evaluate the extent to which organisational justice has an effect on mental health independently of the DCS and ERI models.
-
To discuss theoretical and empirical overlap and differences with previous models.
Methods
Data were collected using three databases: PsychINFO (to identify psychosocial studies), Web of Science and Pubmed. The studies were first selected on the basis of their title and abstract. For practical reasons, articles had to be available in English or French. Second, the scientific literature was searched via the lists of references provided by selected papers, and by literature reviews or meta-analyses. The databases were searched with a combination of three types of search strings: (1) terms related to workplace exposure—(in) justice, organisational justice, relational justice, procedural justice, distributive justice and inequity; (2) terms related to medical issues—mental health, distress, depression, anxiety, fatigue, somatisation, psychological disorders, absenteeism, sickness absence and well-being; and (3) terms related to work setting—job, work, occupation, work stressors and psychosocial factors.
The studies selected for this review were those: (1) published between 1990 and 2010 (2) in a peer review journal, (3) which had a sample size of over a hundred subjects, (4) measured justice as an exposure factor, and (5) used mental health or its consequences as the outcome. This review was limited (6) to prospective studies (7) from industrialised countries. Papers on well-being were also included because these measures often contain items that may be related to mental health symptoms.21 Sickness absence was included because mental health is often the primary or secondary cause of sickness absence among workers in industrialised countries.1–3 ,5 ,6 ,22–24
The studies included here had to present detailed and main results. Therefore, abstracts and short report studies were not considered. Duplicated studies were excluded; intermediate and final results of a single study were considered to be part of the same study. Two studies on fairness25–27 were excluded, as their conceptual framework and measurement differed from the OJ model.
To determine whether the effect of organisational justice had been observed independently of DCS and ERI, we evaluated whether and how the studies controlled for these models. Emphasis was placed on the components of these models, which seemed to overlap conceptually with a justice component.
Results
A total of 403 studies were identified via the database search. We identified a further nine studies from the listed references of selected papers, and five studies were from suggestions made by experts as presented in figure 1. Eleven prospective studies were selected based on reading of the abstracts, gathering of complementary information in the text and the application of selection criteria.

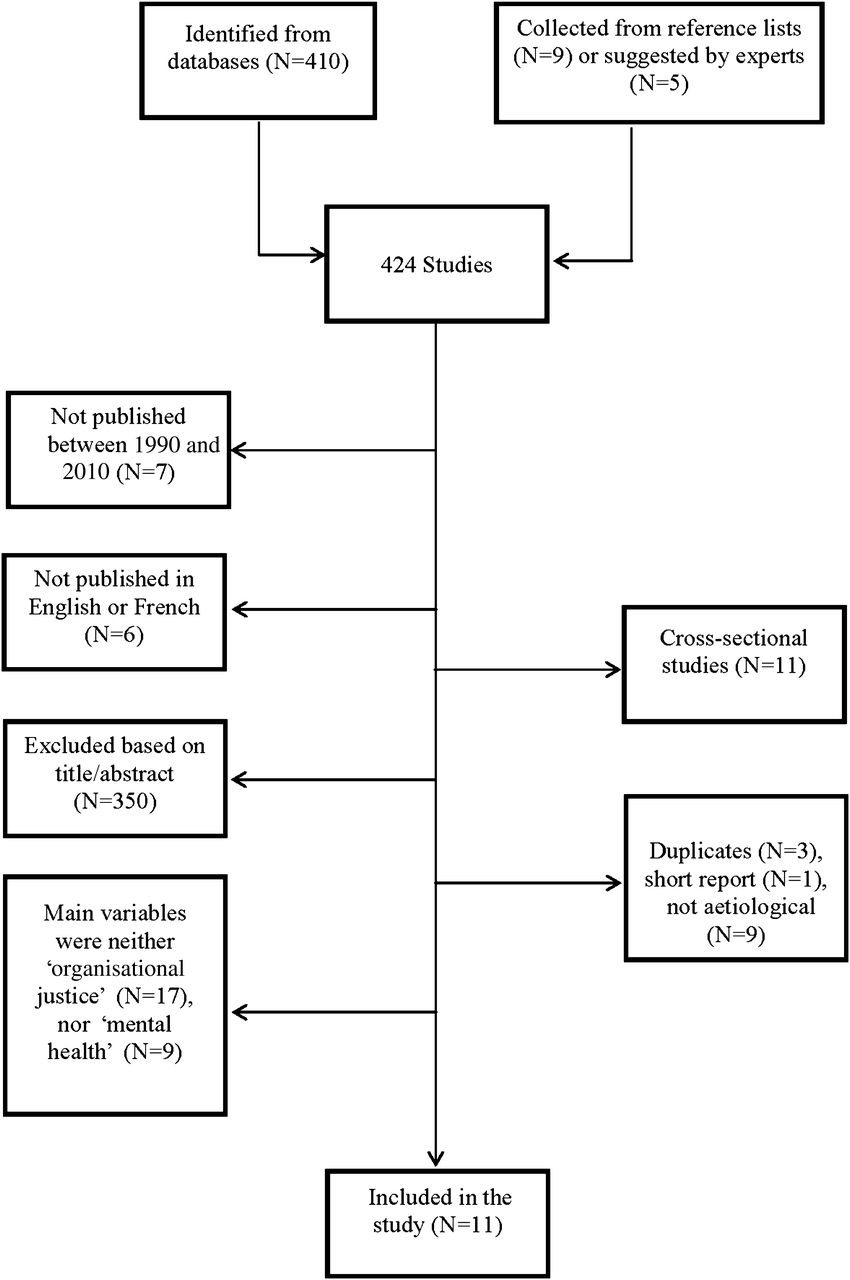{kind=link}
Selection process for identification of studies.
Of the eleven selected studies,28–38 five examined mental health, two examined sickness absenteeism, two focused on well-being, and two looked at more than one of these outcomes. The components of organisational justice fell into the three categories: relational justice, procedural justice and distributive justice.
The populations under study were British civil servants in Whitehall II (approximately 30% of whom were women), hospital personnel in all of the Finnish studies (77% to 100% being women), a representative sample of Dutch employees (43% being women) from various companies in the SHAW cohort, and employees from three Swedish National Labour Market Administration agencies (56% being women).
The main survey instrument was a questionnaire derived from Moorman39 but other instruments derived from Price and Mueller,40 De Boer et al 41 and Darly42 were also used in two studies. Most studies controlled for socio-demographic and lifestyle covariates (such as age, work position, baseline health and lifestyle factors), as well as for psychosocial factors from DCS or ERI models (8/10). All selected papers are presented here in the online supplementary table 1.
Relational justice
Relational justice was the most frequently measured component of organisational justice (10/11 studies). The 10 studies examining relational justice assessed it using 11 items (box 1).28–38 These items refer to a worker's self-evaluation of his relationship with his immediate supervisor.
Items used to assess relational justice
-
Do you get consistent information from line management (your supervisor)?
-
Do you get sufficient information from line management (your supervisor)?
-
When you are having difficulties at work, how often is your supervisor willing to listen to your problem?
-
Do you ever get criticised unfairly?
-
Do you ever get praised for your work?
-
Your supervisor considers your viewpoint.
-
Your supervisor is able to suppress personal biases.
-
Your supervisor treats you with kindness and consideration.
-
Your supervisor takes steps to deal with you in a truthful manner.
-
Your supervisor shows concern for your rights.
-
Your supervisor provides timely feedback.
Most prospective studies (8/10)28–38 controlled for other psychosocial factors (ERI, DCS), and found that relational justice had a significant effect on mental health (seven studies) or sickness absences (three studies). The increases in the effect measures ranged from 1.20 to 1.60 for psychiatric morbidity and almost all were statistically significant. The RR found, in the three studies on sickness absenteeism were modest but statistically significant, about 1.20 regardless of the participants' gender and type of recorded absence (long, short, certified or self-reported).28 ,31 ,32 After adjustment for covariates from DCS and ERI, the observed associations remained the same in five studies,28–37 it became marginally significant in two studies,33 ,35 and non-significant in some of the results of a third study.28 Two studies controlled specifically for social support (SS) at work, the effects remaining statistically significant.29 ,30 ,32
Two studies assessed the effects of change in relational justice and over time on mental health.29 ,30 Favourable changes in relational justice, between baseline and follow-up, were associated in both genders with less risk of deteriorating mental health. The first study found a significant effect of relational justice on minor psychiatric morbidity in men (OR =0.75 (95% CI 0.60 to 0.94)), and a marginal significant effect in women (0.74 (95% CI 0.55 to 1.01)).30 Adverse change was associated with a statistically significant increased risk of psychiatric morbidity: OR =1.81 (95% CI 1.48 to 2.21) for men and 1.74 (95% CI 1.31 to 2.30) for women. In the second study, statistically significant associations of the effect of change in relational justice with self-rated health were observed. The effect size and direction of these changes for both genders were similar to those of the first study.29
In another study,32 it was observed that relational justice was the strongest predictor of medically certified sickness absence (RR =1.22 (95% CI 1.14 to 1.30), compared with procedural justice, workload, decision authority, skill discretion and hostility, which had smaller effects.
Procedural justice
Eight of the studies assessed procedural justice. Six of these studies used an indicator derived from the Moorman et al instrument.31–36 There were a total of seven different items used in these six studies as shown in box 2. In the two other studies, the authors used four items derived from De Boer et al 41 or from Darly42 (box 2).
Items used to assess procedural justice
-
Procedures were designed to hear the concerns of all those affected by the decision.
-
Procedures were designed to collect accurate information necessary for making the decision.
-
Procedures were designed to provide opportunities to appeal or challenge the decision.
-
Procedures were designed to generate standards so that decisions can be made with consistency.
-
Procedures were designed to provide useful feedback.
-
Procedures were designed to provide clarification about the decision.
-
Procedures were designed to represent all sides affected by the decision.
-
The organisation went about deciding to move in a way that was not fair to me.*
-
The way the management made the relocation decision was not fair to me.*
-
The organisation was fair to me in the way that it made the decision to relocate.*
-
The steps that the company took to make the relocation decision were fair to me.*
-
The opinion of employees is taken into account. **
-
All employees are treated in a similar way.**
-
Complaints of employees are taken seriously.**
-
People only regard their own interest.**
Items used in the studies of: *Liljegren and Ekberg38; **Ybema and Van den Bos.37
The six studies addressing mental health outcomes evaluated psychiatric morbidity including depressive symptoms and medically certified depression. All those found significant associations.32–36 In five studies, the relative effects ranged from 1.4 to 1.9. The remaining study found a statistically significant direct path between procedural justice and depressive symptoms (p<0.001 for the normal causality model) using path-analysis.37
Of the three studies on procedural justice and sickness absenteeism,31 ,32 ,37 two found a significant relationship.31 ,32 ,37 The first study found a slight but significant association between procedural justice and the risk of absenteeism: rate ratio =1.08 (95% CI 1.01 to 1.16).32 In the second study, Elovainio et al (2004)31 presented a structural equation model that also showed a slight but significant association between procedural injustice and sickness absenteeism (p<0.001). Using self-reported data on absenteeism assessed, with one item, a third study found no significant longitudinal path between procedural justice and absenteeism.37 Likewise, one study found that procedural justice had a deleterious effect on psychosocial health (p<0.01).38 Five out of the eight studies on procedural justice controlled for either the DCS model31–34 or ERI model.35 In these five studies, the effect of procedural justice remained significant, even after controlling for the other models. The three remaining studies did not control for any psychosocial covariates.
In one study, procedural justice was the strongest predictor of poor self-rated health (rate ratio =1.45 (95% CI 1.18 to 1.77), and the second strongest predictor of minor psychiatric morbidity (rate ratio =1.44 (95% CI 1.22 to 1.72) compared with workload, decision authority, skill discretion and hostility.32
Distributive justice
Two prospective studies evaluated the effect of distributive justice.37 ,38 Distributive justice was measured with items evaluating salary justice, rewards and the appreciation received for one's work (box 3). The structural equation model was used to evaluate the effect of a lack of distributive justice on psychosocial health,38 depressive symptoms37 and sickness absenteeism.37 In the first study, results showed a significant direct path with depressive symptoms and sickness absenteeism (χ2 (68) =234.68, p<0.001 for the model with normal causality). More specifically, distributive justice was associated with a reduction in depressive symptoms and sickness absenteeism 1 year later, after controlling for baseline depressive symptoms.37 In the second study, the authors observed that lack of distributive justice had a deleterious effect on psychosocial health (including role limitations due to emotional problems, social functioning, vitality and mental health), and that this association was statistically significant (p<0.001).38 No control for ERI was performed in either study. Therefore, it was unclear whether this study measured the adverse psychosocial components of distributive justice, which were not assessed by the ERI model.
Items used to assess distributive justice
-
How fair has the hospital been in rewarding you when you considered the responsibilities you have?*
-
How fair has the hospital been in rewarding you when you take into account the amount of education and training you have?*
-
How fair has the hospital been in rewarding you when you consider the amount of effort you have put forth?*
-
How fair has the hospital been in rewarding you when you consider the stresses and strains of your job?*
-
How fair has the hospital been in rewarding you when you consider the work that you have done?*
-
What do you think of your salary when you compare your work efforts with those of your colleagues?**
-
What do you think of the appreciation you get when you compare the number of tasks you have with those of your colleagues?**
Items used in two studies: *Liljegren and Ekberg38; **Ybema and Van den Bos.37
Discussion
The 11 prospective studies measuring the effect of organisational justice on mental health, evaluated three different components: relational justice (10 studies), procedural justice (eight studies) and distributive justice (two studies). Organisational justice components were associated with mental health problems in most of these studies.
It has been postulated, that it is worth studying the relative contribution of each model to the explanation of well-being and health, in view of their differences and complementary aspects.12 Our second objective was thus to determine whether the effect of organisational justice on mental health could be observed independent of the DCS and ERI models. The results suggest that the OJ model does not completely overlap with the latter two, because the former assesses independent psychosocial work factors, which are not evaluated by the DCS or ERI models.
A possible explanation of the independent effects of organisational justice is that equity matters to people because it helps them to deal with uncertainty.13 ,43 In fact, people seemed to use justice perception when they were concerned about potential problems associated with social interdependence and socially-based identity processes.13 The OJ model differs from the DCS and ERI models in two important respects. First, it emphasises interpersonal rather than individual comparisons; thus, it includes features of the evaluation of a referent ratio in addition to individually-related features. Previous results suggested that people do take into account the experiences of others when they form justice judgements.31 Hence, a difference between an individual and referent ratio (ratio of inputs and outputs) would define the stress-provoking component, especially as the current labour market provides less job security and few alternative choices for many employees.16 ,35 A second difference between the OJ model and the DCS and ERI models concerns the assessment of procedural justice as a new psychosocial work factor, which measures the processes and procedures conditioning the distribution of work. The two next sections of this review will discuss the other aspects of the independent effects of organisational justice components.
Comparison with the Demand-Control-Support model
Relational justice may share some common ground with the SS component of the DCS model (especially with regard to SS from one's supervisor).8 It has been recently stated that relational justice and SS are redundant.44 In fact, relational justice refers to the degree of dignity and respect that employees receive from their supervisors, as defined by researchers who have evaluated its effects on mental health. To clarify the effect and contribution of relational justice, we examined whether the studies had adjusted their analysis models for the DCS model. Six studies had done so,29–34 with three of them adjusting specifically for SS.29 ,30 ,34 Of these three studies, two found a statistically significant effect of relational justice on mental health and therefore showed an independent effect of relational justice on mental health.29 ,30 The third study found an effect but did not reach statistical significance.29 ,30 ,34
It has been pointed out that procedural justice cannot be dissociated from decision authority of the DCS model because items in the procedural justice index overlap with decision authority's existing construct.44 In this review, we observed that only one item out of the seven derived from Moorman et al (number 3 in box 1) tended to overlap with decision authority. Of the eight studies on procedural justice, the associations remained statistically significant while controlling for DCS in four studies. Based on these observations, procedural justice can be considered an independent factor.
Comparison with the Effort-Reward Imbalance model
Relational justice may also share some common ground with the reward component of the ERI model.8 We observed that the four studies (out of ten) on relational justice28–30 ,35 controlled for ERI components. Statistically significant associations between relational justice, and different outcomes were observed in these four studies. In one of the studies,28 even though further adjustments were made for ERI reduced associations, between relational justice and long-term sickness absence for all causes in men, the effects remained significant for both genders. One of these studies aimed to explicitly explore whether ERI and relational justice models were redundant or complementary in explaining self-rated health and psychiatric morbidity.35 Concerning procedural justice and ERI, only one study (out of eight) assessed their independent effects.35 The authors found statistically significant associations with self-rated health and psychiatric morbidity after adjustment for ERI.
It has been hypothesised that the distributive justice component overlaps with the theoretical framework of the ERI model, which was suggested by Siegrist (1996). This is because the conceptual and theoretical aspects of distributive justice and the ERI model refer to an equitable distribution of resources and benefits.9 ,44 Although both models measure the ratio between inputs and outputs, it has been pointed out that distributive justice also focuses on interpersonal comparison, while ERI is based primarily on intrapersonal comparison.35 ,45 As proposed by Kivimaki et al,35 there is a major theoretical difference between the ERI and OJ models the former is concerned with reciprocity of exchange within a formal contract, hence reflecting the close links that exist between the work role's constraints and opportunities and the satisfaction of personal needs, whereas organisational justice focuses more closely on the managerial climate within formal organisations, and the quality of interpersonal relationships within the hierarchies. Therefore, distributive justice could measure information apart from what is assessed when using the ERI model, such as information related to the workplace situations. As presented previously, the effect of distributive justice on mental health was evaluated and demonstrated in two studies37 but no control for ERI was performed. Therefore, it was not possible to determine whether or not it is an independent effect. Furthermore, future studies on distributive justice should control for ERI, in order to assess its independent effect on mental health.
The different theoretical models provide distinct and complementary information on the relationship between psychosocial work factors and health.46 Therefore, it might be worthwhile to study the combined effect of OJ, DCS, and ERI models in order to better explain the effects of psychosocial work factors on mental health problems.
Strengths and limitations of available studies and perspective for future research
This review included eleven prospective studies, which have a number of strengths: a large sample size composed of women and men, workers from different occupational sectors and a participation rate ranging from 70% to 83%. As suggested by Rodwell et al (2009), the combination of outcome variables included in the present review, can provide a relatively comprehensive insight into the range of mental health effects associated with organisational justice components in the workplace.47 Moreover, the theoretical background of organisational justice was well-defined and psychosocial factors of other models have been controlled as covariates in most studies. One plausible mechanism through which perceived organisational injustice may affect mental health is prolonged stress.13 Previous research suggests that factors associated with justice perception may be related to factors that influence susceptibility to illness.13 ,48 Furthermore, the prospective design of the studies included, suggests a causal relationship between organisational justice and mental health problems and their consequences.49
However, some limitations were observed. Available studies mainly focused on the relational and procedural aspects, and used different instruments to measure exposure. A standard, validated instrument to measure exposure seems necessary to improve the comparability of studies. Only two of the ten studies examined distributive justice, and to our knowledge, informational justice has rarely been analysed.47 ,50 We suggest that informational and distributive justice be measured more often in order to provide a more complete assessment of organisational justice and to contribute to a better understanding of its effects on mental health. This would, in the long run, help to improve preventive efforts to reduce mental health problems for workers and employers.
Even though seven of the ten studies on relational justice adjusted for DCS or ERI models, only three of the studies adjusted specifically for the SS component. As mentioned previously, SS is the DCS component, which seems to conceptually overlap with relational justice. Adjustment for other components of DCS or ERI is therefore not sufficient to clarify the independent effect of organisational justice. It would be useful in future prospective studies to assess the effect of relational justice independently from SS at work.
Our analysis of items, used to measure the organisational justice components, showed that only items related to procedural justice (box 2) measured the workplace situations, even when the subject was not personally and directly concerned. For relational justice (box 1) and for distributive justice, the items used for measurement involved perception of individual situations. Organisational justice is only partly different from the DCS and ERI models.
Finally, there is a need for more prospective studies that would consider the effect of change (or cumulative effects) of the exposure to organisational justice. It has been shown that a single measurement of exposure generally leads to an underestimation of effect.5 ,51 ,52
Conclusion
This systematic review of eleven prospective studies showed that organisational justice is mainly assessed through two of its three components: procedural and relational justice. In most studies, these two components observed significant effects on mental health. The effects were independent of the DCS and the ERI models, which specifically assessed this independence. However, there is a lack of prospective studies on distributive justice and mental health. Likewise, there is a lack of prospective studies evaluating the cumulative effects of these exposures on mental health over time.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Files in this Data Supplement:
- Data supplement 1 - Online Table 1
Footnotes
-
Competing interests None.
-
Provenance and peer review Not commissioned; externally peer reviewed.