Article Text

Statistics from Altmetric.com
Contact dermatitis is an eczematous eruption caused by external agents, which can be broadly divided into irritant substances that have a direct toxic effect on the skin (irritant contact dermatitis, ICD) and allergic chemicals where immune delayed hypersensitivity reactions occur (allergic contact dermatitis, ACD). Contact urticaria is an immediate reaction from exposure to a substance and is mediated by either irritant or immunological mechanisms; it can resemble ICD but the onset is immediate and short lived. Many allergenic chemicals are also irritants and it is thought that ICD enhances the development of ACD.1 ICD is the commonest presentation of occupational skin disease.2 In industries where workers engage in wet work, almost all workers develop some degree of irritant contact dermatitis. Most workers with mild occupational irritant contact dermatitis do not seek medical attention and accept the condition as an occupational hazard. A better understanding of irritant contact dermatitis will lead to improved management of this common condition.
INCIDENCE AND PREVALENCE
Dermatitis is a common condition that is reported to affect 5–9% of men and 13–15% of women.2 Occupational skin disease accounts for up to 30% of all cases of occupational illness in industrialised countries.3 The overall annual incidence of occupational contact dermatitis (OCD) from reports by dermatologists and occupational physicians to EPIDERM estimated levels at about 1.3 cases per 10 000 workers,4 manufacturing industries accounting for the greatest number of cases seen, followed by healthcare employment. The economic impact of OCD is considerable. Approximately 4 million working days are estimated to be lost every year due to absenteeism resulting from work related skin diseases.1 This can be costed at approximately £200 million. During 1996, dermatological problems accounted for 23.4% of all work related health problems reported to UK occupational physicians. In addition to its economic impact, OCD has an appreciable impact on the quality of the sufferer’s life.5 However, EPIDERM does not record cases sources such as general practitioners, and a recent study of OCD among printers in the UK has shown the prevalence to be much higher.6
CLASSIFICATION AND CAUSES OF ICD
ICD can be divided into several different categories depending on the irritant and its exposure pattern. Chronic cumulative ICD is the most common type seen by healthcare professionals.
-
Subjective irritancy. Idiosyncratic stinging and smarting reactions that occur within minutes of contact, usually on the face, in the absence of visible changes. Cosmetic or sunscreen constituents are common precipitants.
-
Acute irritant contact dermatitis. This is often the result of a single overwhelming exposure or a few brief exposures to strong irritants or caustic agents. Common work chemicals, which cause acute irritant reactions, include:
Concentrated acids, e.g. sulphuric, nitric, hydrochloric, chromic, hydrofluoric acids
Strong alkali, e.g. calcium, sodium, potassium hydroxide, wet concrete, sodium and potassium cyanide
Organic and inorganic salts, e.g. dichromates, arsenic salts
Solvents/gases, e.g. acrylonitrile, ethylene oxide, carbon disulphide, mustine.
-
Chronic (cumulative) irritant contact dermatitis. This occurs following repetitive exposure to weaker irritants which may be either “wet”, such as detergents, organic solvents, soaps, weak acids, and alkalis, or “dry”, such as low humidity air,7 heat, powders, and dusts. Chronic ICD is due to a stepwise progression of damage to the barrier function of the skin (see fig 1).8 It usually presents with dry, scaly fissuring, and eczematous lesions on the fingers and hands; vesicular lesions do occur but are less common than in allergic contact dermatitis. Common causes of chronic ICD include weak irritants, e.g. water, skin cleansers, solvents, and cutting fluids (box 1). At risk occupations include those that involve wet work, e.g. chefs, bakers, bar tenders, caterers, cleaners, hairdressers, metalworkers, nurses, solderers, fisherman, and construction workers.
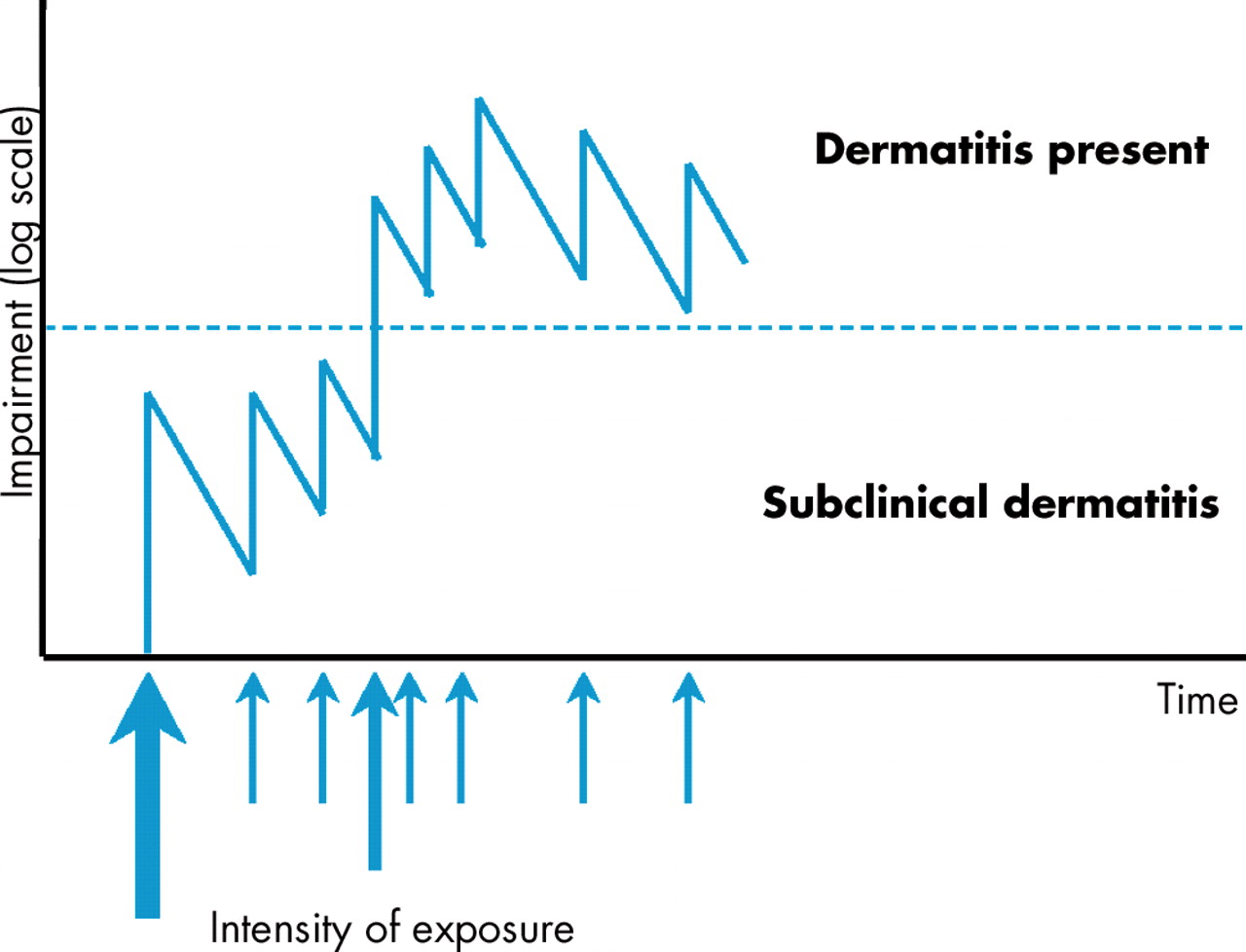
A series of cumulative irritant episodes of vary degree of severity leading eventually to dermatitis. Often the patient does not link the weaker exposures with the dermatitis.
Box 1 Causes of irritant contact dermatitis
-
Water/wet work
-
Degreasing agents
-
Detergents
-
Solvents
-
Metal working fluids
-
Dusts/friction
-
Low humidity
Identification of risk factors for ICD can give an improved understanding of the aetiology of a disease and inform preventive strategies. The development of ICD might be influenced by a combination of exposure characteristics (chemicals handled and working methods) and individual susceptibility. The use of safe working methods and personal protective equipment (PPE) may also vary. Substantial dermato-epidemiological research has also assessed the role of endogenous factors in the susceptibility to ICD.3
In many occupational studies it has been found that the symptoms of ICD tend to decrease when some study subjects were away from work, although it persisted in others. Recurring symptoms in populations varied between 35% and 80%. In addition, healing of ICD may or may not be influenced by a change in occupation. Because patients with ICD notably have a poor prognosis for clearing their skin diseases,9 the primary prevention of ICD is most important (see below).
MAKING THE DIAGNOSIS
Great care must be taken in the accurate distinction between contact dermatitis and endogenous eczema, and between irritant and allergic contact dermatitis. Skill is needed, not only in dermatology, but also in taking an occupational history, and in obtaining as detailed a picture as possible of what the patient actually does at work.10
The clinical distinction on the hands, forearms, or face between endogenous eczema, irritant contact dermatitis, and allergic contact dermatitis is beset with pitfalls. Differences in distribution and morphology are useful guides but dangerous to rely on uncritically. There is a tendency for irritant contact dermatitis to affect the dorsa of the hands (fig 2) and fingers and the finger webs, rather than the palms, and to be relatively devoid of vesicles. There is a tendency for vesicular eczema of the palms and sides of the fingers to be endogenous. However, certain irritants and allergens can produce a highly vesicular eczema of the palmar aspects of the hands and fingers (fig 3), and both allergic contact dermatitis and endogenous eczema frequently involve the dorsal aspects of the hands, fingers, and webs. Discs of eczema on the dorsa of the hands and forearms are frequently endogenous, but allergic contact dermatitis from chromium and cumulative irritant contact dermatitis can present in a similar distribution. Gross eyelid swelling usually indicates allergic contact dermatitis, but degrees of eyelid swelling can occur in both irritant contact dermatitis and endogenous eczema.

Irritant contact dermatitis affecting predominantly the dorsal aspects of the hand and fingers.

{kind=link}
{kind=link}
{kind=link}
Vesicular palmar eczema due to allergic contact dermatitis from dandelions.
It is difficult to overemphasise the importance of a sound working knowledge of occupational irritants, as well as allergens, and of patch testing, in overcoming these difficulties in clinical differentiation. It should be appreciated that hand eczemas, in particular, are often the joint outcome of endogenous, irritant, allergic, and even general climatic factors, and may be partly occupational as well as wholly occupational or non-occupational. In identifying the primary and/or major cause of a contact dermatitis, antecedent and aggravating causes should not be neglected. Diagnosis of secondary bacterial infection in OCD, for example, may allow significant improvement to be obtained with antibiotic therapy.
Patch testing
The mainstay of diagnosis in allergic contact dermatitis is the patch test. This test has a sensitivity and specificity of 70–80%.11 It is not used directly to diagnose ICD or urticaria and involves the reproduction under the patch tests of allergic contact dermatitis in an individual sensitised to a particular antigen(s). The standard method involves the application of antigen to the skin at standardised concentrations in an appropriate vehicle and under occlusion. The back is most commonly used principally for convenience because of the area available, although the limbs, in particular the outer upper arms, are also used. A number of application systems are available, of which the most commonly used are Finn chambers. With this system, the investigator adds the individual allergens to test discs that are loaded onto adhesive tape. The International Contact Dermatitis Research Group has laid down the standardisation of gradings, methods, and nomenclature for patch testing.12 The diagnosis of ICD is made by noting the exposure pattern to irritants and with negative patch tests to potential allergens.
MANAGEMENT
The management of ICD can be divided into treating the active case and prevention. Topical corticosteroids, soap substitutes, and emollients are widely accepted as the treatment of established contact dermatitis. Second line treatments such as topical PUVA, azathioprine, and cyclosporin are probably widely used for steroid resistant chronic hand dermatitis.13
PREVENTION
There are several preventative measures that can be introduced into the workplace. Box 2 gives the range of prevention measures for OCD in order of priority.9 Methods of eliminating and replacement of harmful exposures include, in order of priority: substitution of chemicals that are less irritating or allergenic; introduction of engineering controls; and the organisation of work such that all employees are exposed to the same degree. The uses of personal protection, for example gloves, along with the selection of less susceptible individuals (if these can be identified), are believed to be the last possible measures.
Box 2 Range of prevention measures for occupational contact dermatitis
-
Personal protection (e.g. gloves, barrier creams, after-work creams, soaps)
-
Pre-employment screening
-
Elimination or replacement of harmful substances (irritants, allergens)
-
Technical measures (e.g. encapsulation of the process, automation)
-
Organisation (e.g. wet work distributed to all employees)
Elimination or replacement of harmful exposures
The replacement or elimination of harmful substances is the primary aim of any prevention strategy. This may be achieved by using less noxious substances that are still suitable for the task, for example, replacement with less harsh hand cleansers in the workplace. Ferrous sulphate has been successfully added to cement in Sweden and Denmark to inhibit potentially sensitising chromium.14
Technical control measures
The use of technical control measures to enclose, contain, or isolate potential irritants depends on the physical form and route of exposure.15 If exposure occurs directly from a solid or liquid, enclosure and containment by equipment design or ancillary devices such as splashguards are necessary. If skin exposure occurs primarily through the air in the form of a particulate mist, dust, fume, or vapour, ventilatory controls may be sufficient.
Personal protection
The use of PPE is widely recommended, particularly the use gloves. The correct selection of gloves (see table 1), and also other PPE, must be guided by considering the chemical and physical resistance properties of the gloves, their flexibility in relation to job tasks, and skin surfaces most likely to be exposed.15 Unfortunately more research into penetration studies, especially in the workplace, needs to be undertaken. PPE should be checked regularly and replaced if holes and tears are found, or if there is obvious degradation of the material. Cotton gloves that allow the skin to “breathe” could be used for dry work. For wet work thin cotton gloves that absorb sweat may be worn inside rubber or vinyl gloves and can be removed or replaced as required. Gloves should be removed in a manner so as not to contaminate the operative.
A guide to which gloves will give some degree of protection for specific types of hazard
Barrier creams
Barrier creams by themselves are of questionable value in protecting against contact with irritants.16 Their use should not be over promoted as this may confer on workers a false sense of security and encourage them to be complacent in implementing the appropriate preventative measures. Despite experimental data showing the efficacy of barrier creams,17 their potential value is still viewed with scepticism.18
Key points
-
Occupational contact dermatitis is common
-
Chronic irritant contact dermatitis is the most common single diagnosis of occupational related health problems
-
Making an accurate diagnosis will help in the management of an established case
-
There is a hierarchy of preventative measures which should be introduced into the workplace
-
Work related health programmes have been shown to reduce the incidence of occupational contact dermatitis
After-work creams
A well conducted trial has shown that moisturisers may increase the susceptibility to irritants, yet in practice19 after-work creams appear to confer some degree of protection against developing ICD. Controlled clinical trials have shown benefit in the use of soap substitutes20 and after-work creams21 in reducing the incidence and prevalence of contact dermatitis. They should be encouraged and made readily available in the workplace.
Hygiene and the use of cleansers
Cleanliness is also another measure to consider for the prevention of dermatitis, and the use of approved industrial skin cleansers should be encouraged. Adequate washing facilities should also be provided for workers. There are several basic requirements for an “efficient” skin cleanser to prevent occupational skin diseases. The cleanser should be soluble in hard, soft, cold, and hot water; it should remove fats, oils, and other foreign matter without harming the skin; it should not de-fat the skin or contain harsh abrasives; it should not deteriorate during storage or become insect infected; and it should flow easily through dispensers and not clog the plumbing.
PRE-EMPLOYMENT SCREENING
Workers with underling predisposing factors, for example, atopic dermatitis, hand eczema, or xerosis should avoid wet work and employment exposing them to irritants such as solvents, acids, and alkalis. These workers should be identified and counselled to change to do dry work. Pre-employment identification of at-risk individuals and early job counselling may prevent the occurrence of irritant contact dermatitis in susceptible people.
WORK RELATED EDUCATIONAL PROGRAMMES
Half of all OCDs have been observed to appear in the first two years of employment, which usually includes the training period.22 Lack of awareness of any potential health hazards may lead to complacency in the workplace. Educational efforts should promote awareness and identify work activities in which exposure to irritants are likely. Job training should teach recognition of early signs and symptoms of OCD, proper use of protective clothing and after-work creams, and personal and environmental hygiene. Training may involve the use of instructional pamphlets, videotapes, lectures, and other traditional educational tools.15 Worker education should be initiated before placement in jobs with potential exposure to irritants and should be repeated periodically. Employers should also receive training and act as on-the-job teachers, reinforcing safety lessons and highlighting dangerous chemicals. In Germany there has been a considerable amount of work done with the hairdressing profession to do this; they have shown a tenfold reduction in hairdressers developing dermatitis.23
QUESTIONS (SEE ANSWERS ON P 674)
(1) Which of the following statements about patch testing are true?
-
It is used for investigating the causes of urticaria.
-
It is used for investigating the causes of ICD.
-
It is used for investigating the causes of ACD.
-
It can be used for investigating the causes of both ICD and ACD.
-
It has a sensitivity and specificity of 90%.
(2) Which of the following statements are true?
-
Up to 30% of occupational health problems are due to skin disease.
-
Up to 10% of occupational health problems are due to skin disease.
-
1 million working days are estimated to be lost every year due to OCD.
-
OCD costs industry £20 million per year.
-
Dermatitis is reported to affect 5% of the population.
(3) Which of the following statements concerning ICD are true?
-
ICD depends upon the irritant rather than the individual susceptibility.
-
CD usually occurs from brief exposures.
-
ACD is more common than ICD.
-
The commonest cause of ICD is wet work.
-
ICD has a better prognosis than ACD.
(4) Which of the following statements concerning ICD are true?
-
There is a tendency for ICD to affect the fingers only.
-
The dorsa of the wrist is commonly affected.
-
There is a tendency for ICD to affect the palms.
-
There is a tendency for ICD to affect the dorsa of the hands, fingers, and web spaces.
-
Vesicles are pathognomic.
(5) Which of the following statements concerning the management of OCD are true?
-
Barrier creams can be useful in preventing ICD.
-
Exposure reduction rarely improves ICD.
-
Impervious gloves are the mainstay of prevention of ICD.
-
After-work creams confer some degree of protection against developing ICD.
-
All atopic individuals should be prevented from undertaking wet-work jobs.