Article Text

Statistics from Altmetric.com
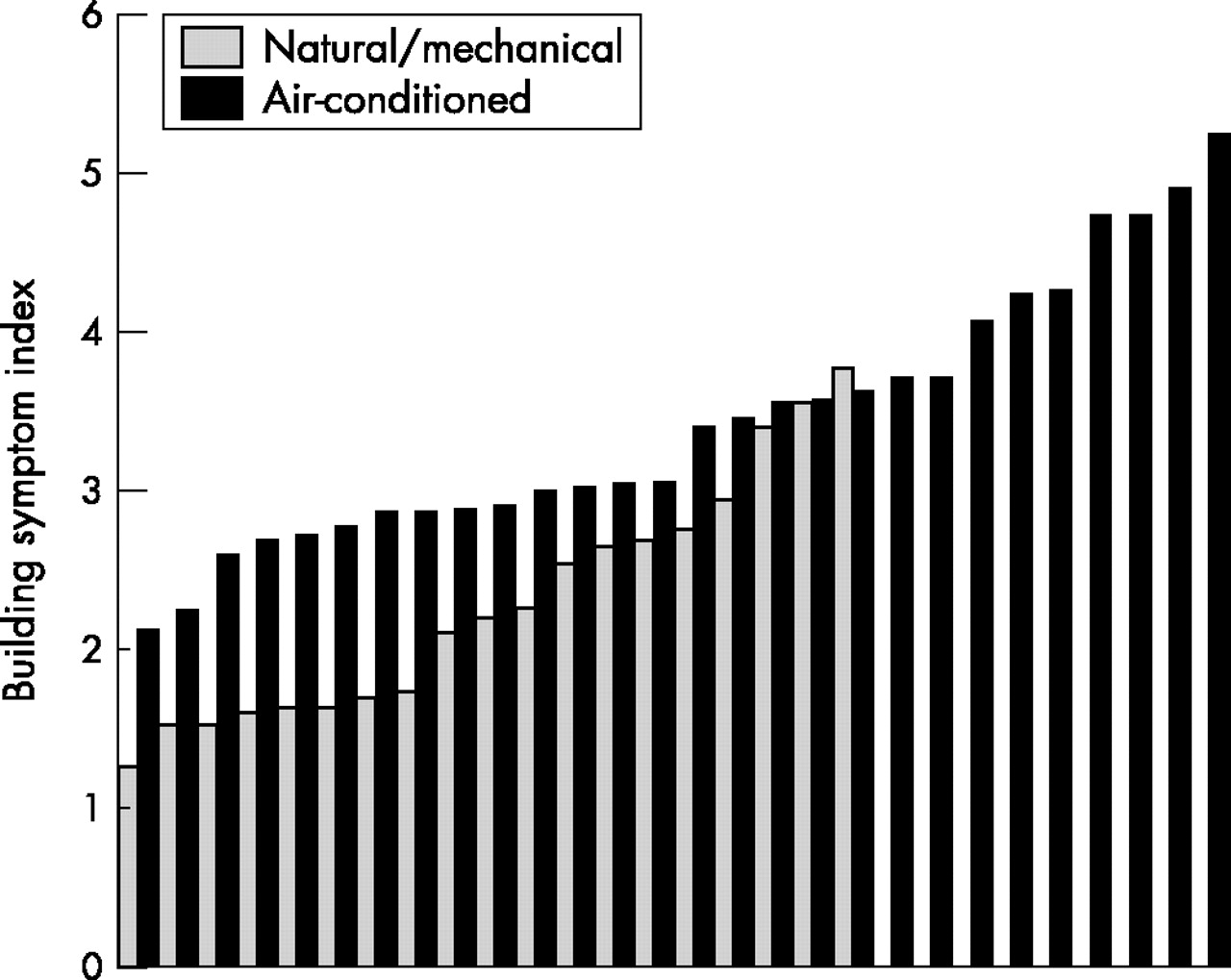
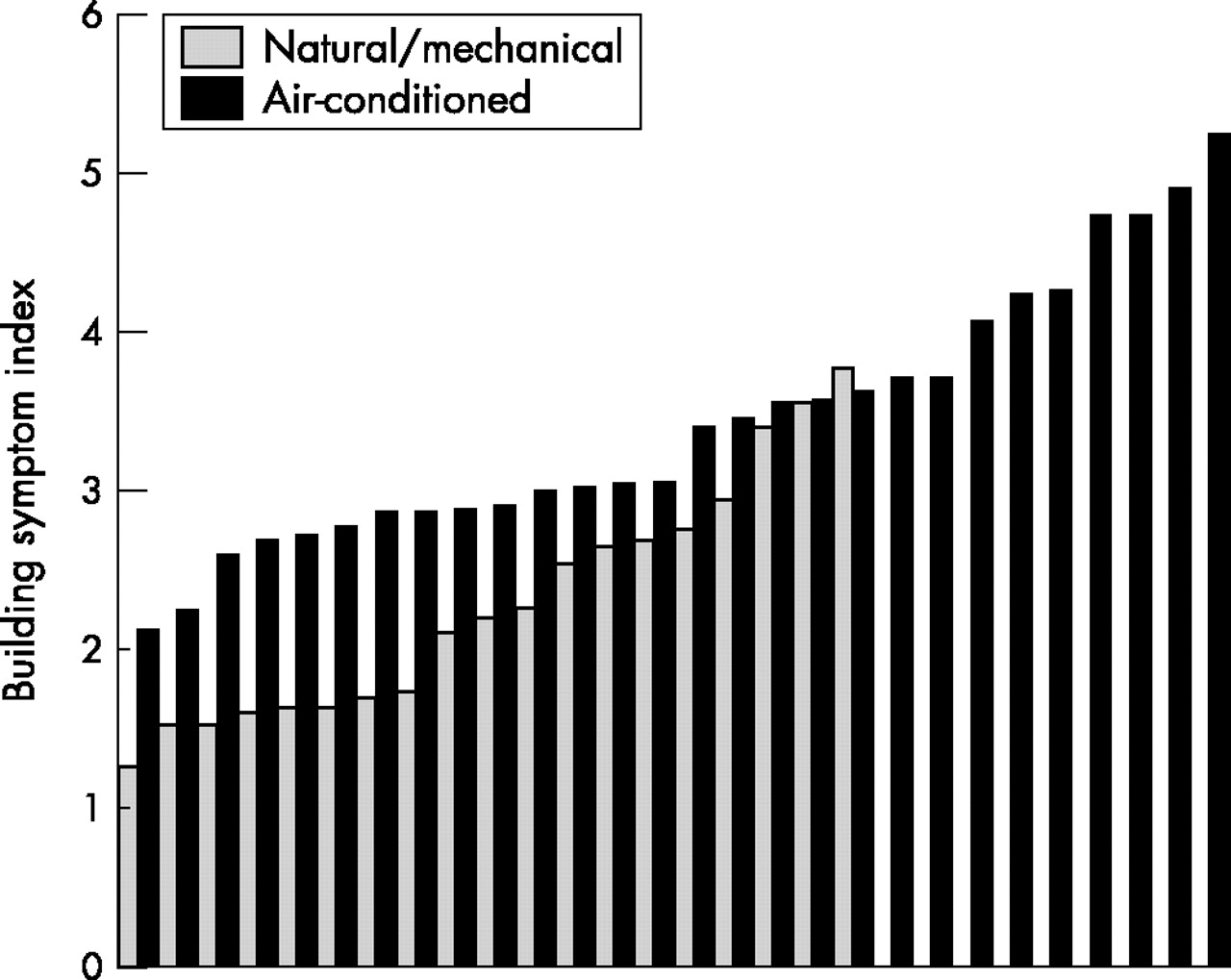
The sick building syndrome (SBS) consists of a group of mucosal, skin, and general symptoms that are temporally related to working in particular buildings. It is the workers who are symptomatic, but the building or its services which are the cause. The common symptoms and a method of assessment are shown in box 2. The average number of work related symptoms per occupant is known as the building symptom index. It can be measured reproducibly by simple questionnaire surveys. The building symptom index shows a wide variation between different buildings (fig 1); “sicker” buildings often have conditions of air temperature, humidity, and lighting levels that fully comply with current standards. Some of the reproducible “facts” shown in studies in different countries are shown in box 1, and factors related to higher (sicker) building symptom indices shown in box 3. Box 4 shows the WHO standards for the management of building ventilation systems. Money spent on the building services is likely to be cost effective in terms of the lost productivity in symptomatic workers.
{kind=link}
Range of building symptom indices in a group of buildings studied with the same questionnaire with a maximum of 10 symptoms (the actual BSI is dependent on the number of possible positive answers and differs between questionnaires).
Box 1: Reproducible observations related to sick building syndrome (?facts)
-
There is a wide range of symptom prevalences between the occupants of different buildings, not explained by personal factors.
-
Air conditioned buildings generally have a higher prevalence of symptomatic workers than naturally ventilated buildings.
-
The sick building syndrome occurs in buildings that fully comply with current design standards in terms of temperature, ventilation, and lighting.
-
Although various chemicals (particularly volatile organic compounds) have been related to symptoms in individual buildings, none have been shown to be a cause of SBS in a wide range of buildings, including those with natural ventilation.
-
Naturally ventilated buildings often have conditions of temperature and ventilation outside recommended standards, and yet often have fewer workers with SBS symptoms.
Box 2: Questionnaire for estimating the prevalence of sick building syndrome in a building14
Each question is prefaced by:
“In the past 12 months have you had more than two episodes of ...?”
And sufficed by:
“If ‘yes’, was it better on days away from the office?”.
-
Itchy or watery eyes
-
Blocked or stuffy nose
-
Runny nose
-
Dry throat
-
Lethargy and/or tiredness
-
Headache
-
Dry, itchy, or irritated skin
Box 3: Factors related to increased prevalence of sick building syndrome
Personal factors
Individual factors
Building factors
-
High indoor temperature (over 23°C in air conditioned buildings)39,40
-
Low fresh air ventilation in air conditioned office (<10 litres/sec/person)41,42
-
Poor individual control of temperature and lighting1,24,40,43,44
-
Poor building service maintenance39
-
Poor cleaning or cleanability39
Box 4: WHO guidelines for the management of building ventilation systems75
-
The building and its heating, ventilation, and air conditioning systems should not produce biological contaminants which are introduced into the ventilation air. If biocides are unavoidable, they should be prevented from entering space which can be occupied.
-
Standards and building codes should ensure effective maintenance of ventilation systems by specifying adequate access paths, regular inspection, and maintenance schedules.
-
In a building, in which occupants cannot effectively control the quality of ventilation air, an individual who is responsible for this task should be identified to the occupants.
-
The maintenance personnel of public and office buildings should be given adequate training for routine inspection and maintenance for the building systems.
HEALTH PROBLEMS RELATED TO WORKING IN OFFICE TYPE BUILDINGS
Health problems are usually divided in building related diseases and sick building syndrome. Building related disease include infectious diseases spread from the building services, such as Legionnaires’ disease, and diseases spread from worker to worker within a building, such as virus infections. They also include any toxic reactions to chemicals used within the building, or derived from fungae growing within a building. They will not be discussed further here. The sick building syndrome comprises a group of symptoms of unclear aetiology divided into mucous membrane symptoms related to the eyes, nose, and throat; dry skin; together with what are often called general symptoms of headache and lethargy. All these symptoms are common in the general population; the distinguishing feature which makes them part of the sick building syndrome is their temporal relation with work in a particular building. All except skin symptoms should improve within a few hours of leaving a problem building; dryness of the skin may take a few days to improve. Office workers are the easiest to study as there are few other confounding factors. Similar problems occur in other buildings, particularly schools, hospitals, and care homes. Problems with indoor air also occur in homes, particularly those with water damage. In Nordic countries the term sick building syndrome is also applied to domestic dwellings. The causes and remedies are often different in these situations, and will not be discussed further in this review.
General symptoms
A general feeling of tiredness is often the most prevalent symptom.1 It usually starts within a few hours of coming to work, and improves within minutes of leaving the building. Symptoms may be seasonal in northern climates, being worse in the winter months, suggesting a relation with sunlight. The typical headache is non-migrainous, rarely throbbing, usually described as dull, and often as a pressure on the head. In Scandinavia the associated symptom of heavy headedness is often prevalent. It is usually less frequent than the lethargy.
Mucous membrane symptoms
The most common symptom is the sensation of a blocked or stuffy nose. True rhinitis with sneezing and running of the nose is much less common. The latter are the typical symptoms of allergic rhinitis due to an inhaled allergen. A feeling of dryness of the throat, perhaps associated with increased thirst, is the next most prevalent mucous membrane symptom. It can be a particular problem in those who use their voice professionally, such as broadcasters or telephonists. Although dry eyes are the least prevalent mucous membrane symptom, it can cause particular problems in those wearing contact lenses, who may not be able to use them throughout the day. Objective signs include reduced foam in the inner epicanthus, and increases tear film break up time.2–6
Dryness of the skin
Dryness of the skin is the most difficult symptom to elicit from questionnaires, which generally require a symptom to improve on days away from the building to be classed as a work related symptom. The more prolonged recovery of skin dryness may lead to its under-recognition. There is a specific facial rash related to VDU use which is very rarely identified, and may relate to precipitation of charged particulates onto the face.7–9
IS THE PROBLEM “REAL”
There are many sceptics as to the validity of the sick building syndrome diagnosis. The name is confusing, as it is the workers rather than the building who suffer from the symptoms, but the cause is with the building and its services. There are few objective tests to validate the symptoms, the exception being those with dry eyes where objective validation is possible but difficult.2–4 Some regard the symptoms as psychological (implying that they don’t really exist). Lethargy is a psychological symptom, but yet can have organic (within the building) causes. The psychological versus organic debate does not produce much enlightenment or resolution of the problem.
There are a number of observations which have been reproduced in different surveys in different countries, which are as close to facts as it is possible to get. They are shown in box 1.
IS THERE A PROBLEM IN A PARTICULAR BUILDING?
Problems can easily get out of hand due to the organisation within a working group. To whom should an individual who perceives health related symptoms due to work in an office type environment turn? There is an association between the perception of poor indoor air quality and symptoms.10 For instance it is likely that the perception of dryness in the air relates more to increased temperature and particulates in the air than to water content; one study showed a fourfold reduction in perceived air dryness following air filtration, without changing the water content of the air.11 Indoor air is often perceived as dry and stuffy, which can easily lead to the ventilation engineer being asked to solve the workers’ symptoms. Unfortunately there is no association between the sensation of air dryness and the water content of the air.10 The measurement of normal humidity if often used to show that the air is not dry, and that by implication the workers’ symptoms are not due to the building environment. Assessment of workers’ symptoms is the role of occupational health professionals, who should be involved at an early stage.
The first step is to visit the workplace and carry out a “walk through survey”. Obvious factors of gross overcrowding, poor cleaning, space management, water damage, and the occupancy of areas of a building not designed as workplaces can be identified without technology. A workforce questionnaire is the next step if there is doubt as to the “realness” and degree of the problem. The questionnaire aims to estimate the building symptom index, the average number of work related symptoms per worker. There are different questionnaires available; many are sufficiently robust for use.12–14 Box 2 shows a suitable one. If the building symptom index is outside the norms, further work is needed. Responding to complaints by measuring individual pollutants is rarely helpful.
In Nordic countries the MM questionnaire is frequently used. Unlike the questionnaires referenced above this does not provide a validated summary measurement,15 but has been the tool for much useful indoor air research.8,16–20
The principal factors shown to be associated with SBS are shown in box 3.
There are a number of individual exposures in the workplace which have been associated with symptoms; the most important are VDU use, paper use, and cigarette smoke.
Visual display units
Several studies have shown a fairly weak but positive relation between the number of hours spent at a VDU and the symptoms of sick building syndrome. One study only found increased symptoms when working at a VDU for seven or more hours a day;24 other studies have however shown an effect at much lower times of VDU use.27,38 Poor software quality might contribute.21 There appears to be a rare but specific facial rash due to VDU use, perhaps due to precipitation of charged air particulates on the skin.9
Paper
There is an association between the amount of paper handled and the symptoms of sick building syndrome in some studies, particularly those in low-technology government departments.27 No carbon required paper has also been associated with respiratory and dermal symptoms,52 as well as the usual sick building syndrome symptoms,30 perhaps due to release of the inks encapsulated on the back of the top sheets, a particular problem during paper shredding. Paper is a major contributor to the fibrous dust associated with symptoms in some studies.
Cigarette smoke
Non-smokers who work in a room with smokers have more symptoms than those working in a smoke-free environment.18,33,34 The major source of environmental tobacco exposure in non-smokers is at work.32 One study has shown a reduction of symptoms when smoking was stopped in the workplace.31 Other studies have not shown an effect of cigarette smoke on symptoms; however smokers and non-smokers were not separated and the levels of exposure in the workplace were low.53
BUILDING FACTORS
After adjustment for the factors described above, the average number of work related symptoms per building occupant (the building symptom index), still shows a four- to fivefold difference between good and bad buildings (fig 1).1 The building symptom index is stable over time, provided that proper sampling is used to avoid responder bias, and a sample size of about 100 is used.39 In general naturally ventilated buildings have fewer symptomatic occupants than those from air conditioned offices,1,45–49 despite measurements of air quality being better in the air conditioned buildings. It seems that the major factors controlled by air conditioning can have both positive and negative effects; the balance often being decided by post-design factors, particularly plant and system maintenance.39 The main factors which have been studied include fresh air ventilation rates, temperature, humidity, dust, and the microbial content of the air. Finding an association between these factors and symptoms does not however imply that altering that factor is likely to reduce symptoms. It is quite likely that all of them are surrogate makers of the underlying causes. Similar problems have been found in hospitals,19,20,54 where the confounding factors of allergens such as latex, infected patients, and a more mobile workforce present problems with epidemiological studies of sick building syndrome.
Ventilation rate
Increasing ventilation helps dilute pollutants generated by the building fabric, the office machinery, and its occupants, but increases exposure to pollutants which may be generated by the ventilation system and its ducting. There are studies showing a relation between ventilation rate and symptoms,42 and others which fail to show a relation.42 Within air conditioned buildings it is likely that low ventilation rates of less than 10 litres/second/person are associated with increased symptoms.41 Studies which have failed to show an effect of changing ventilation rate have generally included only values higher than this. Some studies have shown increased symptoms with increasing ventilation, suggesting that pollutants from the plant are the dominant cause in these cases.55 This effect has also been shown in mechanically ventilated buildings without air conditioning, particularly relating to skin and nasal symptoms.56 Chamber experiments have shown less dry throat with increasing ventilation, and less difficulty thinking clearly.57 Giving individual workplace ventilation control reduced sick building syndrome symptoms over a prolonged period despite a resulting increase in airborne dust and fungal spores, and more variable temperatures.44
Temperature
Increasing symptoms with temperatures above 23°C has been one of the more consistent findings in northern European studies.27,39,40 There is however an association between increasing temperature, overcrowding, and inadequate ventilation which makes it difficult to pinpoint the causative factor.
Humidity
The humidity of indoor air is very dependent on the outdoor climate. Humidification of air to reach indoor air quality standards has not been shown to reduce SBS symptoms. There is an association between the presence of a humidifier in the air conditioning circuit and symptoms, rather than the reverse.1 As with many other factors, humidity can be good and bad. In parts of Scandinavia the humidity may be below 10% for the winter months; there is some evidence that increasing this to around 25% is associated with decreasing symptoms.58 In more temperate climates the humidity indoors rarely falls below 25%; humidifiers in these circumstances can do more harm than good. Humidifiers in the ventilation circuit provide a place for microbes to flourish, and also provide a reason for adding biocides to humidified water. Many of these biocides are irritants or allergens in their own right, for example, isothiozolinones,59–61 glutaraldehyde,62,63 chloramine,64 chlorhexidine,65 benzalkonium chloride,66 and chlorine or nitrogen trichloride.67–69 Their addition to the water used for humidification will result in exposure to the building occupants.60 There are so far no intervention studies investigating biocides in air conditioning systems. They provide a plausible cause for the increased symptoms seen in systems containing a humidifier. In other areas dehumidifiers and chillers can be a potential problem. Water removed from the air can become stagnant and act as a reservoir for microbial growth in the air conditioning system. Many chillers are situated in ceiling and wall spaces where maintenance is difficult. Microbial contamination of chiller condensate trays has caused asthma in one English office.
Freshness of the ambient air
There are no generally agreed methods of assessing the freshness of indoor air. Fanger has developed units of smell emission (the Olf, defined as the smell emission derived from a standard non-smoking person having 0.7 baths per day) and perceived effect (the decipol, the smell in a 10 m3 room containing the standard man, ventilated with fresh air at 10 l/s). Decipols are measured using a panel of trained sniffers.70,71 They can be used to find the source of smells, such as sampling air before and after filters in the air supply ducting. He has shown that the building itself, its ventilation system, the contents such as carpets and furnishings, and its inhabitants, are all measurable sources. For instance the average smoker emits 6 olfs, against 1 for a non-smoker. There is an assumption that all smells are bad. This approach is leading to the quantification and hopefully the elimination of sources.
Bacteria and fungae
The role of indoor air microbial contamination in the aetiology of sick building syndrome is less clear than with alveolitis, humidifier fever, and asthma. There are few adequate studies of the relation between microbial contamination with viable organisms and building sickness, but current evidence does not support a direct relation between the two.49 Pickering and colleagues also studied a building with a clean room, the room being positively pressurised and supplied with air from high grade filters. The microbial lode in the clean area (bacteria plus fungae.) was 125 cfu/m3 compared to 400 cfu/m3 for the area supplied by the standard air conditioning system. Total dust levels were also halved in the clean area. Despite these changes the symptoms of sick building syndrome were, if anything, greater in the clean area.49
Dust
There is evidence that building dust contributes to sick building syndrome, probably in a non-specific manner.36 The first major multibuilding study, the Copenhagen town hall study, showed an association between macromolecular dust and symptoms.27 Most of these buildings were naturally ventilated. Poor cleaning, overcrowding, and poor space management are factors associated with sick naturally ventilated buildings. There are associations between the Gram negative bacterial content of the dust and symptoms, between the particulates and mucous membrane symptoms, between volatile organics desorbed from the dust and general symptoms, and between the macromolecular content of the dust and general symptoms.35 Removing small particles from the air by more efficient filtration reduced the sensation of stuffy air but failed to reduce SBS symptoms in one study.37 Headache, lethargy, and dry nose have been induced in chamber challenges with simulated office dust exposures at about 400 μg/m3.72 One controlled study of office cleaning has shown a reduction in symptoms in the cleaned area which persisted for at least two months after cleaning.73
MANAGEMENT ISSUES
By medical standards the symptoms of sick building syndrome are relatively trivial. Symptoms are generally more common and more problematical in the stressed, the unloved, and in individuals who feel powerless to change their situation. There is a strong association between lack of control of the office environment and symptoms.1,44 There is an association between environmental and job stress and symptoms.24 An inadequate system for dealing with environmental complaints had the strongest correlation with symptoms in one Dutch study.28,74 Good communication between workers, occupational health staff, and building service managers and their plant staff is fundamental to improving existing sick buildings. General guidelines for the management of building services are shown in box 4.
ECONOMIC CONSEQUENCES
The economic consequences of the sick building syndrome relate to the decreased or increased productivity resulting from the working environment, the costs of labour, and the costs of providing the environment. These factors vary widely in different countries and environments. Raw (evidence submitted to the UK parliamentary select committee on the environment) assessed the costs of sick building syndrome in a large government office with 2500 occupants, assuming one day’s sickness absence per year attributed to sick building syndrome and one hour per month dealing with or complaining about the indoor environment. At 1990 prices the costs to the organisation were £400 000 for one year.
Unfortunately it is very difficult to measure productivity in thinking office workers, but chamber experiments have shown faster text typing when the outside ventilation rate was increased from 3, through 10 to 30 litres/sec/person.57 Sickness absence has been used as a surrogate for productivity in several epidemiological surveys; sickness absence however has many determinants apart from the health of the worker. The British office environment study1 included a question asking the worker how much they thought the office environment affected their productivity (on a nine point scale from −40% to +40%). Interestingly there were some workers who thought that the office environment increased their productivity. There was a clear linear relation between the number of work related symptoms of sick building syndrome and self assessed productivity, suggesting that the “disease” was the cause of the reduced productivity.76 The study also showed a clear relation between the type of building and the building symptom index. Those with an average of two (out of 10) work related symptoms had a neutral effect on productivity. The majority of buildings with a building symptom index under two were naturally ventilated with cellular offices and substantial worker control of their environment.
Workers in naturally ventilated buildings often have less sickness absence than those from air conditioned offices. Guberan et al in Switzerland77 found increased sickness absence in a group moving from a naturally ventilated to an air conditioned office. There were six days per hundred workers per month less sickness absence in workers from naturally ventilated offices in a group moving to and from a central air conditioned building in England.78 In Holland there were 34% less days off sick in workers who could control their own environment in their offices. Sickness absence was also higher in buildings with humidifiers.28
A small study has shown improvement in both self rated productivity and measured sickness absence in an office building retrofitted with an air filtration system with both carbon and HEPA filters fitted to each workstation, taking air from the room.11 The intervention area was compared to a control floor of the building. There was a 61% reduction in certified sickness absence compared with a similar period the previous year, equivalent to a 3.1% increase in productive time per worker. A small control area was included on the intervention floor, where the furniture and fan unit was installed without the filtration system. Similar improvements in air quality assessment and symptoms were seen in this area, raising the possibility that the fan unit rather than the filtration were responsible for the improvement.
The current evidence suggests that individuals vary significantly in their requirements for indoor air quality, so that it is not possible to provide one environment that suits a large proportion of the workforce. Workers who are unable to alter environments which they find unsatisfactory are more likely to develop sick building syndrome. Their inability to improve their environment is a source of stress which can contribute to their symptoms, and perhaps to their reduced productivity.38 The workers in a building are its most expensive commodity; looking after their environment as well as that needed for the mainframe computer is likely to be cost effective.