Article Text

Statistics from Altmetric.com
More than 20 years ago, it was suggested that the normal reproductive development of the male embryo may be affected by exposure to oestrogens, the focus initially being on the mother's endogenous oestrogen. In 1993, Sharpe and Skakkebaek proposed the hypothesis that increased oestrogen exposure in early life increases the risk of the two genital malformations hypospadias and cryptorchidism, and of testis cancer in adult life, as well as restricting the achievable sperm concentration (also called density, or more loosely, sperm count).1 In recent years, the focus has shifted to concern about exogenous (xenobiotic) substances. This has become generalised beyond oestrogens to encompass effects relating to other types of hormone, leading to the concept of an endocrine disrupter: “ . . .an exogenous substance that causes adverse health effects in an intact organism, or its progeny, consequent on changes in endocrine function”.w1 Some prefer the term “endocrine modulator”, as some effects may be neutral or beneficial.
It has been suggested that this type of mechanism has caused a deteriorating trend in male reproductive health—involving the same four end points of hypospadias, cryptorchidism, testicular cancer, and sperm density—throughout the world in recent decades,w1–4although it is generally agreed that direct evidence is lacking. Juxtaposition of the fragmentary human evidence with that on fish, reptiles, and other wildlife has fuelled concern in the media, and has led to a large research effort.
It is important to separate the two main questions—the possible existence of a generalised deterioration in male reproductive health, and the hypothesis that endocrine disruption can cause these effects. There are other possible mechanisms: the most potent known testicular toxin in adult life is the nematocide dibromochloropropane (DBCP), an alkylating agent (like many pesticides).w5 Germ line genetic damage to either parent before conception could theoretically affect male reproductive health, but this possibility has received little attention.
The purposes of this paper are: (a) to summarise the descriptive epidemiology; and (b) to review critically the plausibility of the endocrine disruption hypothesis as a possible explanation. Evidence from toxicology and endocrinology and from studies on wildlife are not directly considered, although they inform the discussion. Prostatic cancer is excluded, as age distribution and other features indicate that it is epidemiologically distinct from these four end points. Other human health end points are not reviewed, such as thyroid function, female reproduction, and breast cancer, which have also been linked with endocrine disruption.
DESCRIPTIVE EPIDEMIOLOGY
TIMING OF EXPOSURE
For hypospadias and cryptorchidism, exposure would need to take place before birth. Adult life end points such as semen quality and testicular cancer could be affected by exposures at any time over a broad span. The most likely possibilities are recent exposures, and those occurring in early life that affect long term development of the reproductive system.
The idea of an early impairment with long term effects accords well with what is known about embryonic, fetal, and infant development. Timing of an exposure is as important as its chemical, biological or physical nature: windows of sensitivity occur, which may be relatively short lived. This formed part of the original oestrogen hypothesis, but it is also compatible with non-endocrine mechanisms. In epidemiological terms, early impairment corresponds to a cohort effect—for example, a birth cohort effect in the case of exposure in utero.
A combination of short and long term exposures could be relevant. The most obvious example is for testicular cancer, as it is usual to distinguish initiators and promoters of carcinogenesis.
TESTICULAR CANCER
Epidemiological information on cancer of the testis is very reliable. As a disease of relatively young men that has unmistakable features, it is likely to be rarely missed or misdiagnosed, so that only an efficient collating system is required to produce high quality ascertainment. Good data on incidence have been available from cancer registries in many developed countries for some decades. Mortality data are also available for certain countries going back 100 years, and since the disease is invariably fatal if untreated, these are reliable for the early decades of the 20th century. This is not true more recently, however, as cure rates are now high.
In principle, the descriptive epidemiology should be reviewed separately for each histological type, seminoma and non-seminoma. However, as the descriptive data are generally remarkably similar for both major types, this refinement will be ignored.
Trends
In recent decades, this disease has been increasing in most if not all countries for which data exist. An important and often overlooked question is when this trend began.
In England and Wales, mortality started rising around 1920, having been stable before the first world war (fig 1).2 The age distribution also changed, from one that increased steadily with age throughout life to the now familiar pattern with much lower rates over the age of 40 years. It may be that the disease present in the 19th century was different from that which increased during the 20th century, or at least that its aetiology differed.
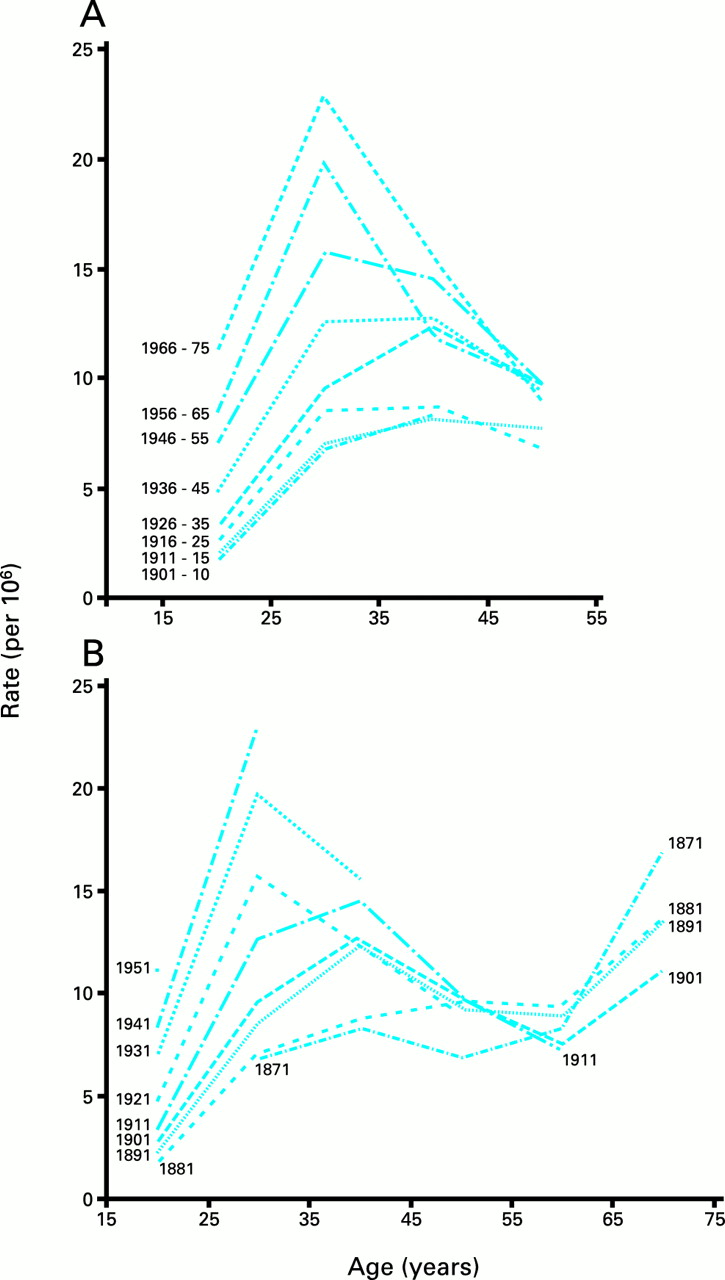
Death rates per million from testicular cancer in England and Wales, by age, in successive decades by (A) year of death (period effect) and by (B) birth cohort. Reproduced from Davies2 with permission of the publisher.
In Denmark, a continuous rise in age standardised incidence is observable since cancer registration began in 1943.3 A similar picture is seen throughout the developed world, with trebling of rates being common. The rise has been steady, except for a few instances—for example, in Victoria, Australia where the rate was transiently stable or fell slightly in the early 1970s.w6
Predisposition to testicular cancer is present from an early age, probably in utero.w7 Environmental agents could influence this predisposition. If these trends are examined in relation to the time of birth rather than of death or diagnosis, mortality started rising among men born before 1900 in England and Wales, for those who developed the young onset form of the disease (fig 1).2 In Denmark, the increase began in men born around 1905.4 In Denmark, Norway, and Sweden, rates stabilised or fell for men born during 1935-45 (slightly earlier for Sweden), whereas the rise was rapid and inexorable among men born from 1920 until at least 1960 in East Germany, Finland, and Poland.4 Recent data suggest that the rates may be stabilising for Danish men born since about 1960.w8
Spatial and ethnic variation
The highest incidence in the world is found in Denmark, where the lifetime risk is now almost 1%. However, the Nordic countries do not have a uniformly high risk, as Finnish men have comparatively low rates, with Norway and Sweden in intermediate positions (fig2).3 The spatial pattern for testicular cancer in the Nordic countries does not resemble that of other hormone sensitive carcinomas such as those of the prostate or female breast, but is not dissimilar from that of colorectal cancer in both sexes.5However, testicular cancer is unusual in that the gradations in risk appear to follow national boundaries.5
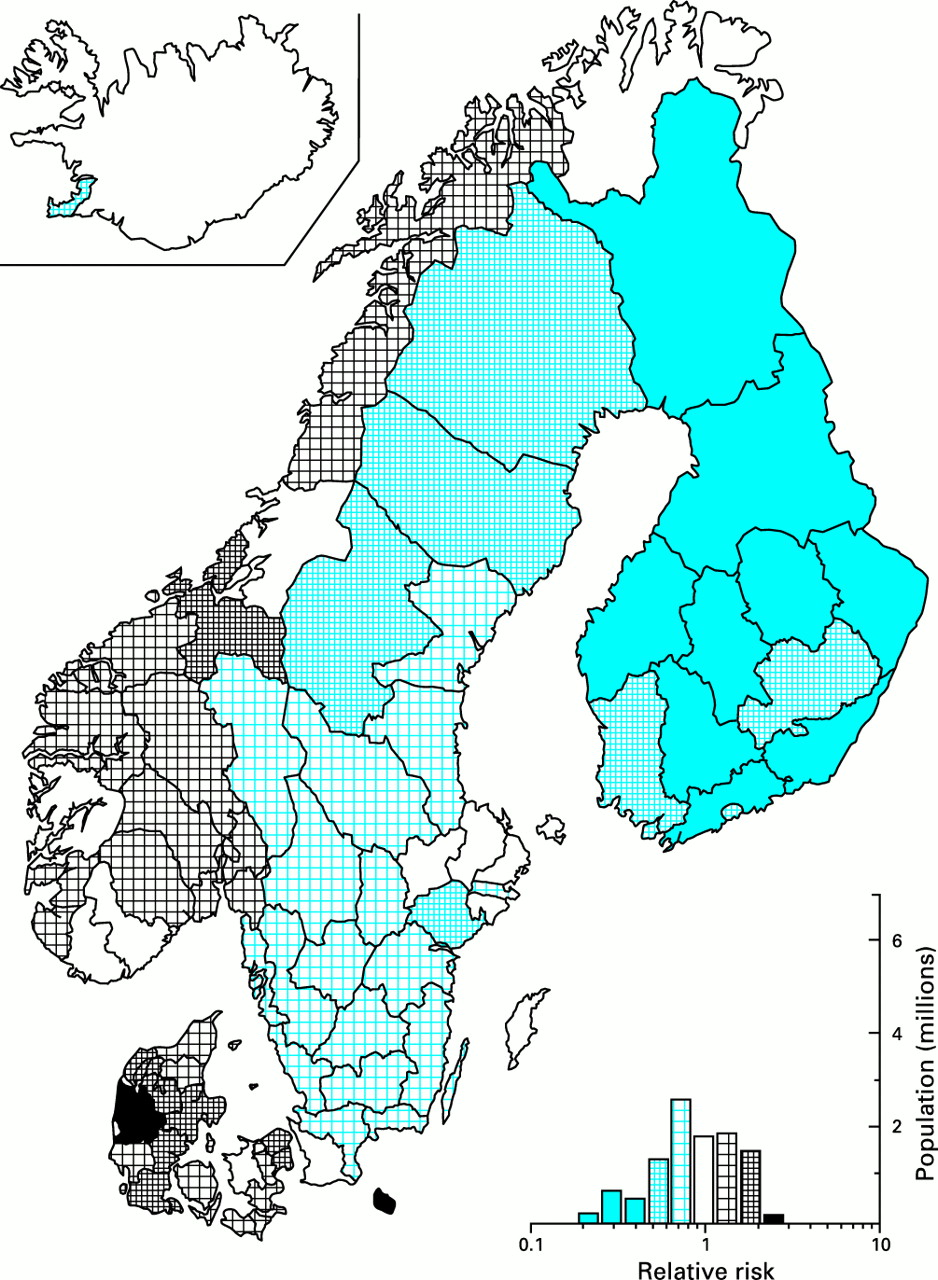
Map of age standardised incidence of testicular cancer in the counties of the Nordic countries, 1970-79. A frequency diagram is also given. Reproduced from Møller Jensen et al,5 with permission of the Danish Cancer Society.
Other high risk populations include Switzerland6 w9 and New Zealand (including Maoris),6 w10 whereas the Baltic states3 and African Americans6 have comparatively low rates. The tumour is rare among Chinese and Japanese men.6
Interpretation
Heredity may be relevant for international and inter-ethnic differences, but cannot explain rapid trends. Possible explanations include dietary changes—in macro- or micronutrients or in contaminants—or environmental exposure. The early part of the trend cannot be caused by chemicals introduced since the mid-20th century. During the earlier period there were major changes in diet, such as increasing meat consumption, and an increasingly sedentary lifestyle. However, although these fit quite well with the epidemiological trend, there is currently no evidence to incriminate them causally.
SEMEN QUALITY
The literature on semen quality is much more problematic. It is usually taken to include sperm concentration, motility, and morphology, but the “time trend” debate has focused mainly on the first of these. All are subject to large degrees of within-person biological variation or measurement error, or both. In addition, descriptive epidemiology cannot be based on representative samples of the general population, as participation rates are too low. The best evidence is from candidates for semen donation and for vasectomy; data from men in contact with medical services for a fertility related problem are unreliable.
Trends
The most cited paper is a 1992 review of the world literature that related sperm concentration to date of publication irrespective of location,7 and which claimed a 50% decline in the mean concentration over 50 years, from 113 × 106/ml down to 66 × 106/ml. However, its major importance is that it stimulated analysis of more reliable data, in places where information on semen quality has been continuously available over a long period. Those data are less likely to have been distorted by possible changes in the method of semen examination and/or in selection processes affecting the populations studied.
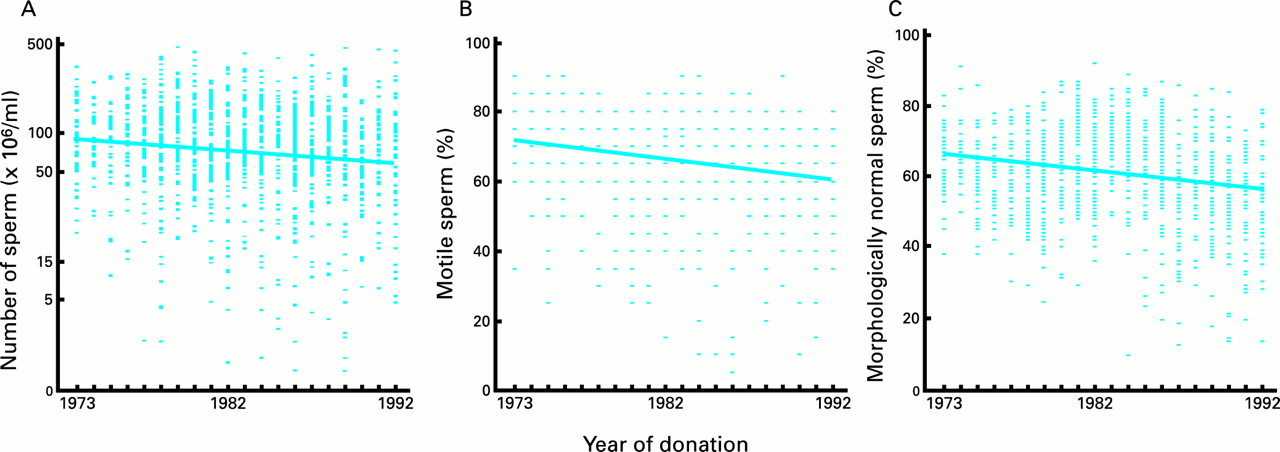
The principal conclusions to emerge are that: (a) declines in semen quality have occurred in some places (for example, Paris (fig 3), Gent, Edinburgh) but not in others (Toulouse, Finland, and the five US cities with published data)8-10 w11–15; (b) at most, the available data go back to the early 1970s; and (c) where concentration has deteriorated, so usually have sperm motility and morphology. Where a decline has occurred, the findings are compatible with a birth cohort effect epidemiologically, affecting men born since about 1950, but this is not conclusive. There is no information on the year when the decline started, for any of the sites, nor what the pre-decline values were. As semen quality is inferior in humans compared with other mammalian species, it is possible that deterioration from a “natural” level has a much longer history than we have the data to substantiate.
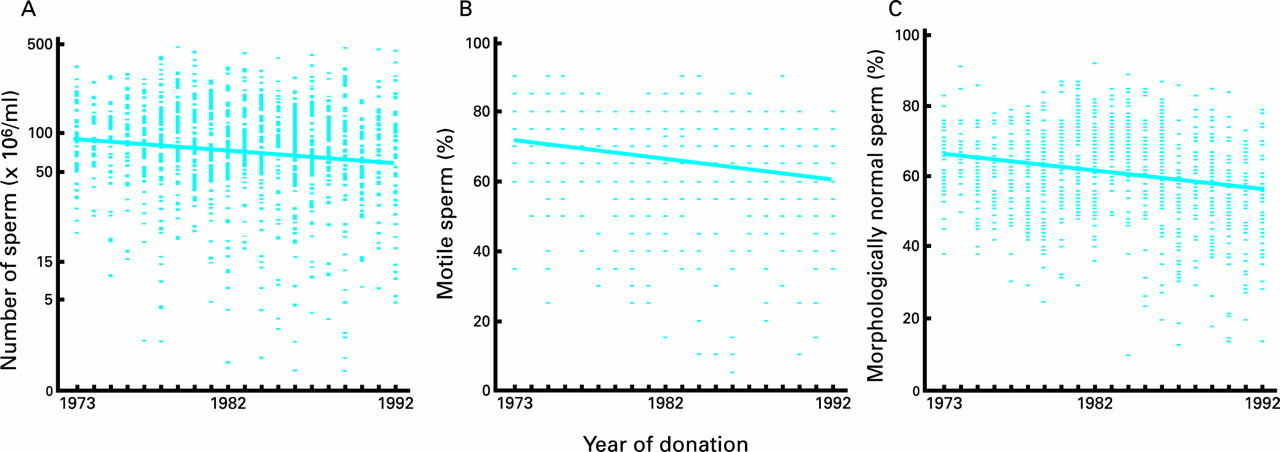
Linear regression of (A) sperm density, (B) mobility, and (C) morphology against year of donation for 1351 fertile men, Paris, 1973-92. The results were equally compatible with a birth cohort effect. Reproduced from Auger8 with permission of the publisher.
A re-analysis of the hypothesis that formed the basis of the original meta-analysis attempted to address its suggested methodological inadequacies.11 The decline in sperm density was found to be much steeper in Europe than in the USA; studies from elsewhere are too sparse and diverse to draw confident conclusions. The principal remaining confounding factors that could at least partially account for a downward trend were age, duration of abstinence, and method of specimen collection. However, a question mark still remains over the plausibility of a hypothesis that involves grouping together all studies that originate from an area as large as the USA or western Europe, especially as the spatial heterogeneity within each is known to be considerable.w16 One way in which this analysis can be reconciled with the more reliable single centre time trend studies is to accept that semen quality has declined in some parts of Europe, but that there has been no such trend in the USA.
Spatial variation
Substantial spatial variations in sperm concentration have been demonstrated, both in Europe and in the USA,10 w16 w17 being relatively high in New York and Finland and low in California and north western Europe, including Denmark and Britain. In the case of Finland, couple fertility is also high compared with Britain,w18 suggesting that the higher sperm counts there are not caused by longer abstinence (less frequent intercourse).
Interpretation
Variations in semen quality are poorly understood, and are hampered by lack of good quality data. Focusing on the hypothesis that there has been a roughly simultaneous worldwide decline obscures important spatial variation, and the occurrence of trends at different times in different places.
If unlinked to other end points, possible explanations for these variations could include an increasingly sedentary way of life, possibly together with tight clothing, since raising the intratesticular temperature has a potent effect on the quality as well as the quantity of sperm.w19 A decreasing duration of abstinence, perhaps as a result of increasing acceptability of masturbation, could account for a decline in sperm quantity but not a deterioration in quality.
CONGENITAL ABNORMALITIES OF THE MALE GENITALIA: HYPOSPADIAS AND CRYPTORCHIDISM
Hypospadias is a condition in which the urethral opening is abnormal in position, in severe cases on the shaft of the penis. Cryptorchidism refers to the failure of the testes to descend into the scrotum. Both are likely to be unreliably ascertained at birth, particularly in mild cases, and the study of cryptorchidism is further complicated by the difficulty of distinguishing testes that have not descended from those that readily but reversibly retract back into the abdominal cavity. The consequence is that published data from congenital malformation registries cannot be relied upon to reflect real variations: reported time trends and differences between registries may both merely reflect differences in ascertainment and reporting.12 Self-reported data (by mothers) are similarly unreliable.
Trends and spatial variation
The only clear indication of an upward trend in hypospadias is from Atlanta, Georgia, where a step increase was observed between 1982 and 1985 in the severe form, which is more reliably ascertained.12 w20 Recent studies in Denmark and Finland using strict criteria have shown a higher rate in Denmark.w21 w22
In the case of cryptorchidism, a study was carried out in Oxford during the 1950s using strict diagnostic criteria, and examination of the baby boys at 3 months when the diagnosis is more reliable.13 A subsequent study also in southern England using the same criteria found an approximate doubling of the proportion of boys having cryptorchidism at 3 months.13 Recent studies in New York w23and in Finland,w24 again using the same criteria, found a similar proportion to the original Oxford estimate, whereas in Denmark it was close to the later English value.w25
Interpretation
The scarcity of good data is a serious problem for both these conditions. Cryptorchidism may well have increased in England, and appears to be more prevalent there and in Denmark than in New York and Finland. Hypospadias is also more frequent in Denmark than in Finland.
THE QUESTION OF LINKAGE
If two conditions frequently occur together, it is likely that they share common causal agents. Thus, the observation that cancer tends to arise in the testes of subfertile men more often than expected by coincidence14 encourages the search for a causal agent that underlies both end points. However, if one causes the other, as is likely for cryptorchidism and testicular cancer,w26 this inference does not follow (fig 4); cryptorchidism does not necessarily share determinants with testicular cancer in non-cryptorchid testes (over 90% of cases), and other evidence is required. The principal risk factor known to be shared—low birth weightw27—does not contribute to the present discussion, as its spatial and temporal variation are insufficient.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
In the left hand diagram, the apparent association between A and B is brought about by the confounding effect of C. In the right hand diagram, as C causes A and A causes B, there is no need to infer any relation between C and B.
Common risk factors can be inferred from epidemiological evidence if the conditions have a similar pattern of variation. For example, the sharp contrast between Finland and Denmark for all four end points suggests possible linkage.
Simultaneous time trends for different conditions may also suggest a shared causal factor that varies in a corresponding manner, allowing for latent periods, etc. Thus, for an exposure acting in utero, linked trends in congenital malformations and adult life end points will tend to be a few decades apart. However, as many factors vary with time, an observation of simultaneous variation is unreliable evidence for linkage.
Box 1: Descriptive epidemiology—key points
- ▸
- It has been suggested that the health of the male reproductive system has been deteriorating, affecting four end points: sperm density, testicular cancer, hypospadias, and cryptorchidism
- ▸
- Testicular cancer has increased almost everywhere, the upward trend beginning in the early 20th century or before
- ▸
- Predisposition to cancer of the testis arises in early life, possibly in utero; this may be true of impaired semen quality as well
- ▸
- The evidence for a trend in the other end points is inconclusive, but suggests deterioration in semen quality—not only sperm density—as well as in cryptorchidism and possibly hypospadias
- ▸
- For end points other than testicular cancer, evidence for a trend is weak outside north western Europe, and even there the date of onset is unclear
- ▸
- There is notable spatial variation in all the end points. In each case the reproductive system of Finnish men is healthier than that of Danish men, which is consistent with the idea that the four are linked
Endocrine explanations
THE OESTROGEN HYPOTHESIS
A large number of substances have at least some oestrogenic activity. Lists of these are available (see box), but caution is required, as many of these compounds have important biological actions that are not mediated by this mechanism (and also many published lists are inaccurate). In addition, one needs to consider the mother's endogenous estradiol.
The source of exposure is related to the question of timing. In utero exposure (necessary for the two end points that are present at birth) could be to endogenous or exogenous oestrogens; in addition, exogenous oestrogens could be relevant in postnatal life.
Endogenous oestrogen
Mammals are adapted to starting life inside their mothers, whose blood streams are rich in estradiol (even before the early pregnancy surge). In contrast to other vertebrates the default sex is female, and masculinisation of the gonads and central nervous system depends on the presence of androgens.
There is some evidence that variation in the concentration of maternal estradiol is associated with the risk of testicular cancerw28 w29 and of cryptorchidism.w30 Nutritional intake is associated with estradiol concentration. It has been suggested that the modern low fibre, high fat western diet may increase maternal concentrations, leading to problems with the reproductive health of their male offspring.w31
Exogenous substances with oestrogenic effects
The relative exposure of the fetus to exogenous and endogenous oestrogens is an important issue, which depends both on potency and on concentration in fetal tissues. Diethylstilboestrol (DES) is a synthetic non-steroidal substance that is more potent than estradiol and crosses the placenta. Other oestrogenic substances have much lower potency. Taking account of concentrations likely to occur, by far the most important are phyto-oestrogens, such as the isoflavones which are abundant in soya. They have mixed oestrogenic and anti-oestrogenic effects, as they bind to the receptor but only activate it weakly. Industrial chemicals with known oestrogenic activity similarly tend to have mixed agonist and antagonist effects. They are at least five orders of magnitude (100 000-fold) less potent than estradiol and 100-fold less potent than phyto-oestrogens. They also occur in far smaller quantities than dietary phyto-oestrogens.15
It has often been argued that maternal estradiol does not reach the fetus, because it is bound to plasma proteins. Up to 99% may be effectively removed in this way, although this still leaves 1% of circulating hormone free. It is also said that estradiol does not cross the placenta. However, although the estradiol concentration in the embryo during sexual differentiation is unknown, it seems unlikely that there is close enough to an absolute barrier to overcome the vast difference in potency between endogenous oestrogens and exogenous agents, except possibly in the case of phyto-oestrogens.
DES was prescribed for millions of pregnant women in the 1940s, 1950s, and 1960s, in the mistaken belief that it could prevent threatened miscarriage. Pharmacological doses were given in early pregnancy, and in principle this is therefore a good test of whether the male embryo is sensitive to oestrogens. Of the four end points discussed in this paper, only cryptorchidism was clearly increased.w32 Other genital malformations also occurred, notably epididymal cysts, hypoplastic testes, and urethral stenosis, but not hypospadiasw32 (a mis-reading of stenosis as hypospadias has unfortunately been propagated erroneously in the literature). One study of sperm density found a slight reduction among those who had been exposed in utero (91 × 106/ml versus 115 × 106/ml in the placebo exposed group).w33 This fall was smaller than that observed in Paris, for example, from 89 × 106/ml in 1973 to 60 × 106/ml in 1992.8 Not all studies have found a reduction.w34 The fertility and sexual function of men exposed in utero were unaffected when they were studied at almost 40 years of age.w35
The situation with testicular cancer is unclear, with both positive and negative studies. A review by the US National Cancer Institute concluded that there was no link,w36 but others estimate that the relative risk may be as high as 2.0w2 (which is less than the increase in incidence in many countries). There may have been some underestimation of association in some studies because exposure occurred after the critical developmental period in about half of the subjects, together with problems in ascertaining exposure,w37 but on the other hand the positive case control studies may have been influenced by recall bias.
The clearest epidemiological evidence on the effect of phyto-oestrogens comes from populations with a high soya intake, notably Chinese and Japanese men. The incidence of testicular cancer is lower even than in Finland,6 but semen quality appears to be comparable with that in western Europe.w38
There is no epidemiological evidence on industrial compounds with oestrogenic activity (other than DES), such as bisphenol A, octylphenol, and nonylphenol. Clear cut and repeatable toxicological results are also lacking for the end points considered here. As these compounds are pharmacologically similar to phyto-oestrogens but far less potent, it is difficult to believe that there is a harmful effect.
Box 2: Principal exogenous substances that may affect sex hormone function
A Oestrogenic and anti-oestrogenic effects
(1) High potency
- ▸
- DES (diethylstilboestrol)
- ▸
- Ethinyl estradiol (component of contraceptive pill)
(2) Medium potency
- ▸
- Phyto-oestrogens
- –
- isoflavones (for example, genistein, daidzein)
- –
- coumestans (for example, coumestrol)
- –
- lignans
(3) Low potency
- ▸
- Bisphenol A
- ▸
- Octylphenol and nonylphenol
- ▸
- Pesticides, including chlordecone, DDT, dieldrin, endosulfan, p,p'-methoxychlor, toxaphene
B Anti-androgenic effects
- ▸
- p,p′-DDE
- ▸
- Certain phthalates (for example, DBP, DEHP)
- ▸
- Pesticides, including linuran, procymidone, metabolites of vinclozolin
- ▸
- Hydroxyflutamide
C Others
- ▸
- Dioxins, furans, and “dioxin-like” PCBs (polychlorinated biphenyls)
This classification is an over simplification: it conflates receptor mediated effects with those caused by other mechanisms—for example, interference with hormone synthesis. Moreover, several of the “oestrogens” show considerable affinity for the androgen receptor For the reasons given in the text, compounds in the A3 category cannot plausibly be considered responsible for the types of impairment of the male reproductive system considered in this paper
OTHER ENDOCRINE MEDIATED EFFECTS
Anti-oestrogenic effects
As mentioned above, many exogenous “oestrogens” also have anti-oestrogenic effects. One way in which the original hypothesis has become broadened is the idea that oestrogen antagonism can generate the effects that were originally attributed to oestrogenic stimulation. Empirically, the evidence on phyto-oestrogens is equally relevant to this hypothesis.
Anti-androgenic effects
An alternative version of the endocrine disruption hypothesis is androgen antagonism. Anti-androgens do not face the same problem of competition with endogenous estradiol, and the idea is plausible because the development of maleness in mammals depends on androgens.
Most of the available information on anti-androgens comes from toxicology. Blocking of androgen action has been found by p,p′-DDE, a stable breakdown product of DDT (dichlorodiphenyltrichloroethane),16 and other substances—for example, metabolites of the pesticide vinclozolin.17 Several phthalates are known to inhibit testosterone synthesis.w39 There is some experimental evidence in rats and/or rabbits that such substances can produce hypospadias and cryptorchidism, early malignant change in cryptorchid testes, and reduced sperm counts.w39
EXPECTED SPECTRUM OF EFFECTS
A different approach is to ask, what epidemiological changes would be expected a priori from exposure to endocrine disrupters of various types: which end points would be affected, and in which sex? In general, females are more sensitive than males to oestrogenic effects. Female offspring were far more affected than male by maternal DES exposure,18 and the effects of phyto-oestrogens are principally evident in females.
Many other cancers are hormone sensitive, and could potentially be influenced by xenobiotic endocrine disrupters. One would expect a rise in oestrogenic or a fall in androgenic activity to go with an increase in male breast cancer and a decrease in prostate cancer. Among women, endometrial and breast cancer would be expected to rise. Only the latter has occurred, and its incidence is much lower in populations who consume high quantities of soya.6
Toxicologists routinely use end points involving growth and development as markers of endocrine activity. Any endocrine mediated disturbance would be expected to affect age at puberty. No such change has occurred among boys, either in western Europe or the USA,w40 w41 in contrast with suggestive evidence of widespread precocious puberty among girls in the USA, especially African American girls.w42 Disturbance of other secondary sexual features might also be expected—for example, inappropriate body hair or gynaecomastia—and disturbances of growth including timing of epiphysis closure. These have not been reported.
INTERPRETATION
Variation in endogenous estradiol is a possible candidate to explain the observed temporal and spatial variations. However, it is unclear whether maternal estradiol concentrations are sufficiently sensitive to nutritional factors to explain the observed trends and/or spatial variations, as there has been insufficient research in this area. Substances that block androgen or oestrogen receptors in the hypothalamo–pituitary axis could increase maternal gonadotrophin and therefore endogenous oestrogen secretion. Evidence that the concentration of maternal estradiol is associated with biological changes undermines the argument that the embryo is not exposed to endogenous oestrogen.
For exogenous agents, the DES episode provides evidence that in utero oestrogenic exposure is unlikely to influence strongly the end points discussed in this paper other than cryptorchidism. This contrasts with its much more devastating impact on female offspring, which included vaginal carcinoma in young women.w43
The low incidence of testicular cancer in Japanese and Chinese men undermines the idea that exposure to phyto-oestrogens (at any stage of life) or to any mechanistically similar compounds increase the risk of the disease. Overall evaluation of the effects of phyto-oestrogens needs to take account of their beneficial role in relation to numerous diseases, including coronary heart disease and various cancers.19
Environmental pollutants cannot plausibly be responsible for adverse effects on the health of the male reproductive system caused by oestrogenic activity, on grounds of potency and mechanistic analogy.
In contrast, it is plausible that anti-androgens could play a role. However, the substances currently known to have anti-androgenic activity have been introduced since the second world war, and therefore cannot explain the earlier rise in testicular cancer. Exposure to p,p′-DDE also cannot explain the observed epidemiological differences between Finland and Denmark, as DDE concentrations in human milk have been shown to be similar in all the Nordic countries; they have declined sharply since 1970.20
However, even if spatial differences and past trends are not explicable in this way, current/recent exposure to DDE and to phthalates (which are now ubiquitous) may possibly have adverse effects. It is reassuring that very high exposure to DDE in developing countries since the 1950s, as a result of malaria eradication programmes, has not resulted in a major epidemic of testicular cancer in young men.6 This suggests that anti-androgenic substances may not be sufficient to cause this disease in non-cryptorchid testes.
A broader argument against the importance of endocrine disruption for problems with the male reproductive system is that the observed spectrum of effects differs in important respects from that expected on biological grounds. The trends in a variety of endocrine sensitive cancers do not form a coherent pattern, and associated disturbances in boys' pubertal development and secondary sexual characteristics have not been observed.
Box 3: Endocrine explanations—key points
- ▸
- A prevalent hypothesis is that the male reproductive system is susceptible to damage by substances with endocrine activity, such as oestrogens
- ▸
- The mother's endogenous oestrogen may possibly affect the male fetus, but there is insufficient evidence to support this as an explanation of the epidemiological findings
- ▸
- The human evidence on relatively strong exogenous oestrogens does not support the hypothesis: DES (see text) has been conclusively linked only to cryptorchidism, and some populations whose diets contain abundant oestrogens of plant origin have low testicular cancer rates
- ▸
- Environmental pollutants with weaker oestrogenic activity cannot plausibly be responsible for the observed trends or spatial variation
- ▸
- Anti-androgens are a more likely cause, but the earliest known example is DDE (from DDT use) which was introduced after the trend in testicular cancer began, and widespread exposure in the developing world has not led to an epidemic of this disease
- ▸
- The observed spectrum of effects differs from that which would be expected a priori for an endocrine mechanism
- ▸
- The timing of the testicular cancer trend is consistent with a dietary origin, and the search for candidates should extend beyond hormonal agents to include those capable of causing genetic damage
Conclusions
The accumulation of evidence on different end points suggests a real deterioration in the health of the male reproductive system, at least in some populations. There has been a widespread increase in testicular cancer, starting 100 years ago in some places. There has probably been a deterioration in semen quality in north western Europe in recent decades. There may well have been an upward trend in cryptorchidism, at least in England, but clear trends in hypospadias have not been established.
Large spatial variations occur in all of these four end points. There is suggestive evidence for linkage, in that the reproductive system of male Finns is consistently healthier than that of Danes and (probably) others in north western Europe.
Explanations are much less certain. Extrapolation from egg laying creatures to mammals is unhelpful. The causes may be different for each end point, but some shared determinants appear to be likely. Exogenous oestrogens are not strong candidates, but increased maternal estradiol cannot be ruled out. Anti-androgens are more likely, according to findings in experimental animals, but for testicular cancer this hypothesis would predict a major epidemic in large parts of the developing world which has not occurred.
The historical timing of the trend in testicular cancer implies that any agent introduced since the mid-20th century cannot be responsible for the earlier changes. This includes all industrial chemicals currently known to be endocrine disrupters. A change in dietary intake could be responsible, possibly one associated with increasing prosperity.
The search for causal factors should not be confined to endocrine disrupters. Genetic damage could predispose to testicular cancer and to impaired capacity for spermatogenesis. A genotoxic agent would have to be absorbed by the gut, to reach the embryo during sexual differentiation, and to localise within the testis. Mutagens in food include heterocyclic amines, which occur in meat (especially if well cooked), and have been implicated in colorectal cancer. It is plausible that they meet these criteria; in particular, their structure suggests that activated heterocyclic amine molecules could bind to androgen and/or oestrogen receptors, which would deliver them to the testicular DNA, where they could cause diffuse genomic damage.
QUESTIONS (see answers on page 260)
(1) Testicular cancer:
(a) is associated with male factor infertility
(b) incidence has increased in some places and fallen in others
(c) is especially common in Finland
(d) is especially common in Denmark
(e) is mainly a disease of old age
(2) Sperm concentration:
(a) is the only way of assessing semen quality
(b) is reliably measured from a single sample
(c) has been shown to decline over time in Paris
(d) has been shown to decline over time in New York
(e) tends to be high among Finnish men compared to Danes
(3) Which of the following statements on cryptorchidism and hypospadias are true/false?
(a) There is good evidence for an increase in cryptorchidism in England
(b) There is good evidence for an increase in hypospadias in England
(c) Geographical differences in hypospadias are difficult to establish because of problems with ascertainment and reporting
(d) Hypospadias is more common in Denmark than in Finland
(e) Cryptorchidism is more common in Finland than in Denmark
(4) Which of the following statements are true/false?
(a) In utero DES exposure increases the risk of cryptorchidism
(b) In utero DES exposure increases the risk of hypospadias
(c) Japanese men have a low risk of testicular cancer
(d) There has been a generalised increase in all hormone sensitive cancers
(e) Precocious puberty has become increasingly common among teenage boys
(5) Which of the following statements on oestrogenic/anti-androgenic activity are true/false?
(a) Endogenous oestrogens are bound to plasma proteins
(b) Oestrogenic activity has been found in numerous industrial compounds
(c) Soya contains substances that have mixed oestrogenic and anti-oestrogenic effects
(d) Anti-androgenic activity has been found in breakdown products of certain pesticides
(e) p,p′-DDE is the only known anti-androgen that was present in the environment in the early 20th century
Acknowledgments
I would like to thank Sue Barlow, Jens Peter Bonde, Cate Boyle, and Tina Kold Jensen for comments on earlier drafts. The views expressed are entirely my own.
References
Supplementary materials
- Are problems with male reproductive health caused by endocrine disruption?
Additional references
- Holmes P, Harrison P, Humfrey C. European workshop on the impact of endocrine disrupters on human health and wildlife. Brussels: Commission of the European Community, Brussels, 1997.
- Toppari J, Larsen JC, Christiansen P, et al. Male reproductive health and environmental chemicals with estrogenic effects. Copenhagen: Danish Environmental Protection Agency, 1995.
- Institute for Environment and Health. Assessment on environmental oestrogens: consequences to human health and wildlife. Leicester, UK: Institute for Environment and Health, 1995.
- Kavlock RJ, Daston GP, DeRosa C, et al. Research needs for the risk assessment of health and environmental effects of endocrine disruptors: a report of the U.S. EPA-sponsored workshop. Environ Health Perspect 1996;104(suppl 4):715-40. [Abstract]
- Whorton D, Krauss RM, Marshall S, et al. Infertility in male pesticide workers. Lancet 1977;ii:1259-61. [Abstract]
- Stone JM, Cruickshank DG, Sandeman TF, et al. Trebling of the incidence of testicular cancer in Victoria, Australia (1950-1985). Cancer 1991;68:211-19. [Abstract]
- Skakkebaek NE, Berthelsen JG, Giwercman A, et al. Carcinoma-in-situ of the testis: possible origin from gonocytes and precursors of all types of germ cell tumours except spermatocytoma. Int J Androl 1987;10:19-28. [Abstract]
- Moller H. Trends in incidence of testicular cancer and prostate cancer in Denmark. Hum Reprod (in press)
- Levi F, Te V-C, La Vecchia C. Testicular cancer trends in the Canton of Vaud, Switzerland, 1974-87. Br J Cancer 1990;62:871-3. [Abstract]
- Pearce N, Sheppard RA, Howard JK, et al. Time trends and occupational differences in cancer of the testis in New Zealand. Cancer 1987;59:1677-82. [Abstract]
- Van Waeleghem K, De Clercq N, Vermeulen L, et al. Deterioration of sperm quality in young healthy Belgian men. Hum Reprod 1996;11:325-9. [Abstract]
- Irvine S, Cawood E, Richardson D, et al. Evidence of deteriorating semen quality in the United Kingdom: birth cohort study in 577 men in Scotland over 11 years. BMJ 1996;312:467-71. [Abstract]
- Bujan L, Mansat A, Pontonnier F, et al. Time series analysis of sperm concentration in fertile men in Toulouse, France, between 1977 and 1992. BMJ 1996;312:471-2. [Abstract]
- Wittmaack FM, Shapiro SS. Longitudinal study of semen quality in Wisconsin men over a decade. Wis Med J 1992;91:477-9. [Abstract]
- Paulsen CA, Berman NG, Wang C. Data from men in greater Seattle area reveals no downward trend in semen quality: further evidence that deterioration of semen quality is not geographically uniform. Fertil Steril 1996;65:1015-20. [Abstract]
- Fisch H, Goluboff ET. Geographic variations in sperm counts: a potential cause of bias in studies of semen quality. Fertil Steril 1996;65:1044-6. [Abstract]
- Suominen J, Vierula M. Semen quality of Finnish men. BMJ 1993;306:1579.
- Joffe M. Lower fertility in Britain compared with Finland. Lancet 1996;347:1519-20.
- Thonneau P, Bujan L, Multigner L, Mieusset R. Occupational heat exposure and male fertility: a review. Hum Reprod 1998;13:2122-5. [Abstract]
- Paulozzi LJ, Erickson JD, Jackson RJ. Hypospadias trends in two US surveillance systems. Pediatrics 1997;100:831-4. [Abstract]
- Schmidt IM, Chellakooty M, Haavisto AM, et al. Rate of hypospadias in newborn Danish boys in an urban area. Poster presentation at Workshop on Hormones and endocrine disrupters in food and water, Copenhagen 2000.
- Virtanen H, Kaleva M, Haavisto AM, et al. Prevalence of hypospadias in Turku area in Finland. Poster presentation at Workshop on Hormones and endocrine disrupters in food and water, Copenhagen 2000.
- Berkowitz GS, Lapinski RH, Dolgin SE. Prevalence and natural history of cryptorchidism. Pediatrics 1993;92:44-9. [Abstract]
- Kaleva M, Virtanen H, Haavisto AM, et al. Incidence of cryptorchidism in Turku area in Finland. Poster presentation at Workshop on Hormones and endocrine disrupters in food and water, Copenhagen 2000.
- Schmidt IM, Haavisto AM, Chellakooty M, et al. Rate of cryptorchidiem in newborn Danish boys in an urban area. Poster presentation at Workshop on Hormones and endocrine disrupters in food and water, Copenhagen 2000.
- United Kingdom Testicular Cancer Study Group. Aetiology of testicular cancer: association with congenital abnormalities, age at puberty, infertility, and exercise. BMJ 1994;308:1393-9. [Abstract]
- Moller H, Skakkebaek NE. Testicular cancer and cryptorchidism in relation to prenatal factors: case-control studies in Denmark. Cancer Causes Control 1997;8:904-12.[Abstract]
- Depue RH, Pike MC, Henderson BE. Estrogen exposure during gestation and risk of testicular cancer. J Natl Cancer Inst 1983;71:1151-5. [Abstract]
- Henderson BE, Ross R, Bernstein L. Estrogens as a cause of human cancer [review]. Cancer Res 1988;48:246-53.
- Depue RH. Maternal and gestational factors affecting the risk of cryptorchidism and inguinal hernia. Int J Epidemiol 1984;13:311-18. [Abstract]
- Adlercreutz H. Diet, breast cancer and sex hormone metabolism. Ann N Y Acad Sci 1990;595:281-90. [Abstract]
- Henderson BE, Benton B, Cosgrove M, et al. Urogenital tract abnormalities in sons of women treated with diethylstilbestrol. Pediatrics 1976;58:505-7. [Abstract]
- Gill WB, Schumacher GFB, Bibbo M. Association of diethylstilbestrol exposure in utero with cryptorchidism, testicular hypoplasia and semen abnormalities. J Urol 1979;122:36. [Abstract]
- Leary FJ, Resseguie LJ, Kurland LT, et al. Males exposed in utero to diethylstilbestrol. JAMA 1984;252:2984-9. [Abstract]
- Wilcox AJ, Baird DD, Weinberg CR, Hornsby PP, Herbst AL. Fertility in men exposed prenatally to diethylstilbestrol. N Engl J Med 1995;332:1411-16. [Abstract]
- National Cancer Institute. SEER cancer statistics review: 1973-1990. Miller BA, Ries LAG, Hankey BF, et al, eds. No.93-2789. Bethesda, Maryland: National Cancer Institute, National Institutes of Health, 1993.
- Swan SH. Human effects of prenatal DES exposure. Presented at Workshop on hormones and endocrine disrupters in food and water, Copenhagen 2000.
- Iwamoto T, Hoshino T, Nishida T, et al. Semen quality of Japanese fertile men; a study of partners of pregnant women. Presented at Workshop on Hormones and endocrine disrupters in food and water, Copenhagen 2000.
- Gray LE Jr, Ostby J, Furr J, et al. Effects of environmental antiandrogens in experimental animals. Presented at Workshop on Hormones and endocrine disrupters in food and water, Copenhagen 2000.
- de Muinck Keizer-Schrama SMPF, Mul D. Trends in pubertal development in Europe. Presented at Workshop on Hormones and endocrine disrupters in food and water, Copenhagen 2000.
- Lee PA, Guo SS, Kulin H. US growth surveys. Presented at Workshop on Hormones and endocrine disrupters in food and water, Copenhagen 2000.
- Herman-Giddens ME, Slora EJ, Wasserman RC, et al. Secondary sexual characteristics and menses in young girls seen in office practice: a study from the Pediatric Research in Office Settings network. Pediatrics 1997;99:505-12. [Abstract]
- Herbst AL, Ulfelder H, Poskanzer DC. Adenocarcinoma of the vagina: association of maternal stilbestrol therapy with tumor appearance in young women. N Engl J Med 1971;284:878-81.
Footnotes
-
websiteextra Additional references appear on the Occupational and Environmental Medicine website www.occenvmed.com