Article Text

Abstract
BACKGROUND Nitric oxide (NO) is detectable in the exhaled breath, is involved in airway defence and inflammation, and probably modulates bronchial smooth muscle tone. Given the sensitivity of nitrogen oxides to local redox conditions, we postulated that exposure to oxidant or antioxidant compounds could alter concentrations of NO in the exhaled breath (eNO). We assessed the effect of nitrogen dioxide (NO2) and ascorbic acid exposure on eNO in healthy human subjects.
METHODS Ten healthy subjects were randomised to undergo a 20 minute single blind exposure to NO2 (1.5 parts per million) or medical air in a crossover fashion. Exhaled NO and pulmonary function were measured before and for 3 hours after exposure. In a separate double blind crossover study 20 healthy subjects received ascorbic acid 500 mg twice daily or placebo for 2 weeks with a 6 week interim washout. Serum ascorbic acid levels and eNO were measured before and after each supplementation phase.
RESULTS NO2induced a decrease of 0.62 (95% CI 0.32 to 0.92) ppb in the mean post-exposure eNO (p<0.01) with no change in forced expiratory volume in 1 second (FEV1). Oral supplementation with ascorbic acid increased the mean serum ascorbic acid concentration by 7.4 (95% CI 5.1 to 9.7) μg/ml (63%) but did not alter eNO.
CONCLUSIONS NO2exposure causes a decrease in eNO, an effect which may be mediated through changes in epithelial lining fluid redox state or through a direct effect on epithelial cells. In contrast, ascorbic acid does not appear to play a significant role in the metabolism of NO in the epithelial lining fluid.
- nitric oxide
- nitrogen dioxide
- ascorbic acid
- glutathione
- superoxide
- epithelial lining fluid
Statistics from Altmetric.com
Nitric oxide (NO) is a product of the enzyme nitric oxide synthase (NOS) and is detectable in the exhaled breath. However, unlike other gaseous pulmonary products, NO is produced predominantly in the airways. NOS is induced in inflamed airways and, since exhaled NO (eNO) is increased in asthma, NO has been suggested as a potential non-invasive marker of airway inflammation.1 However, NO is a highly reactive molecule with many potential target molecules in the airway wall and in the epithelial lining fluid (ELF).2Concentrations of NO gas in the airway lumen may therefore not only reflect changes in NOS activity or induction, but also changes in local airway chemistry.
A precedent for this suggestion can be found in the systemic vasculature where NO is the predominant endothelium derived relaxing factor. In this environment, NO has a very short half life due to its rapid reaction with superoxide,3 and its activity is modified by the antioxidant ascorbic acid.4 ,5
In the lung there is already evidence that eNO is affected by changes in airway chemistry. Patients with cystic fibrosis do not have increased eNO levels despite the severity of their airway inflammation, but they do have increased levels of nitrite, the stable end product of NO autoxidation, in breath condensate.6 These findings suggest that, although NOS activity is increased in this patient group, NO undergoes autoxidation before passing into the lumen. Changes in airway chemistry have been postulated to alter eNO in asthma as well. The pH of breath condensate is lower in patients with asthma7 and, since NO metabolism is pH sensitive, this may help to explain the increase in eNO found in asthmatic subjects.8
The aim of the studies presented here was to determine if eNO is altered by exposure to oxidants (nitrogen dioxide (NO2)) and antioxidants (ascorbic acid) in healthy human subjects. Ascorbic acid was chosen for the antioxidant exposure because of its known effects on the chemistry of NO in the systemic vasculature.4 ,5 NO2 was chosen for the oxidant exposure as this oxidising gas is known to undergo reactive absorption and then to alter ELF redox state in the airway ELF in a predictable and reproducible fashion following inhalation.9 ,10
Methods
STUDY DESIGN
Given that the intra-individual standard deviation in eNO in healthy volunteers is approximately 0.8 parts per billion (ppb) while the inter-individual standard deviation is approximately 3 ppb (data from previous work in our laboratory), paired designs were chosen to increase the power of the studies. For the ascorbic acid study, in order to have an 80% chance of detecting a 1 ppb difference in eNO between active and placebo supplementation at the 0.05 significance level with a standard deviation of 0.8 ppb, 20 subjects were required. The summation of serial measures used to assess eNO in the NO2 study (see statistics section) should lead to a smaller intra-individual standard deviation, so only 10 subjects were recruited to undergo NO2 exposure.
SUBJECTS
Healthy non-smoking subjects not taking nutritional supplements were screened. Those with spirometric evidence of airway obstruction, those with known respiratory disease, and those taking glucocorticoid medication were excluded. Subjects who had participated in one study were not considered for participation in the other.
PROTOCOL
NO2 exposure
Exposures with medical air and NO2 1.5 parts per million (ppm), each for 20 minutes at rest were carried out at the same time of day on separate days with an interval of at least 1 week in a single blind, randomised, placebo controlled, crossover fashion.
The exposure system has been previously described.11Briefly, subjects sit, resting comfortably, with the head enclosed in a perspex dome, while medical air is delivered at 120 l/min by means of an in-series mass flow controlled valve (5853E, Brooks Instruments, Netherlands). CO2 concentrations in the dome are monitored during exposure and nose clips are not used. For the NO2exposure, NO2 in nitrogen (60 ppm, British Oxygen Company) was blended via another mass flow controlled valve (5850S, Brooks Instruments) in a ratio of 1:40 to obtain a final concentration for NO2 of 1.5 ppm. The final concentration was checked before all exposures using an NO2 analyser (PrinterNOx, Micro Medical Ltd, Kent, UK) sensitive to 0.05 ppm. Before exposure, eNO levels were measured five times and the mean was taken as the baseline eNO level, and spirometric tests were performed (Vitalograph Compact, Vitalograph Ltd, Buckingham, UK) to obtain the best FEV1and forced vital capacity (FVC) from at least two exhalations within 5%. After exposure, eNO levels were measured in triplicate and FEV1 was recorded at each of 0, 5, 10, 15, 30, 45, 60, 90, 120, 150, and 180 minutes. Spirometric tests were always performed after eNO assessment.
Ascorbic acid supplementation
This study was also performed in a randomised, placebo controlled, crossover fashion but the supplementation in this case was double blind. The study design was based on the pharmacokinetic data obtained for ascorbic acid by Levine et al who showed that 1000 mg/day ascorbic acid would be expected approximately to double serum concentrations of ascorbic acid without significant risk of toxicity.12 ,13 Two supplementation phases, each of 2 weeks, were separated by a 6 week washout phase. Subjects continued to consume their normal diet during the study. During the active phase subjects consumed ascorbic acid 500 mg morning and night and during the placebo phase they consumed an identical looking and tasting placebo (Quest Vitamins Ltd, Birmingham, UK). Compliance was checked by pill counts at the end of each supplementation phase. eNO was assessed as the mean of five measurements before and after each supplementation phase, and venous blood was drawn for the estimation of serum ascorbic acid concentrations.
For the serum ascorbic acid assay, 1 ml of serum was combined with 1 ml 10% metaphosphoric acid, prepared fresh daily, and centrifuged at 3000 rpm for 6 minutes. The supernatant was then stored at –70°C until analysed. The assay was performed using a highly sensitive high performance liquid chromatographic method.14 Ascorbic acid concentrations are expressed in μg/ml. The normal range in healthy individuals is diet dependent, but is usually >4 μg/ml.13
ENO ASSESSMENT
eNO was measured by chemiluminescence (LR2000, Logan Research, Kent, UK) in accordance with European Respiratory Society and American Thoracic Society guidelines.15 ,16 Briefly, subjects inhaled to total lung capacity and then completed a slow vital capacity exhalation through a resistance with a flow meter in series. A visual feedback display allowed the subject to maintain a flow rate of approximately 200 ml/s during the exhalation while the resistance maintained soft palate closure. Nose clips were not used. The chemiluminescence analyser sampled the exhalate in real time at 250 ml/min (4.2 ml/s) with a sensitivity of 0.3 ppb and a sampling rate of 25 Hz. Calibration was performed daily and eNO levels were obtained from the plateau phase of the exhalation curve.
STATISTICAL ANALYSIS
Parametric statistics have been used throughout since eNO is normally distributed. For both studies data were analysed using change from baseline during each treatment period. For the NO2study the serial eNO measurements after exposure were summarised for each individual using the area under the curve method,17and the change from baseline levels was then calculated. For both studies FEV1 was expressed as percentage predicted. Data for each study were first assessed for period and order effects. Mean changes in eNO (ΔeNO) and serum ascorbic acid concentrations (ΔVit C) after exposure are presented with 95% confidence intervals and have been assessed for statistical significance using pairedt tests.
Both studies were approved by the East Birmingham Health Authority research and ethics committee.
Results
NO2 EXPOSURE
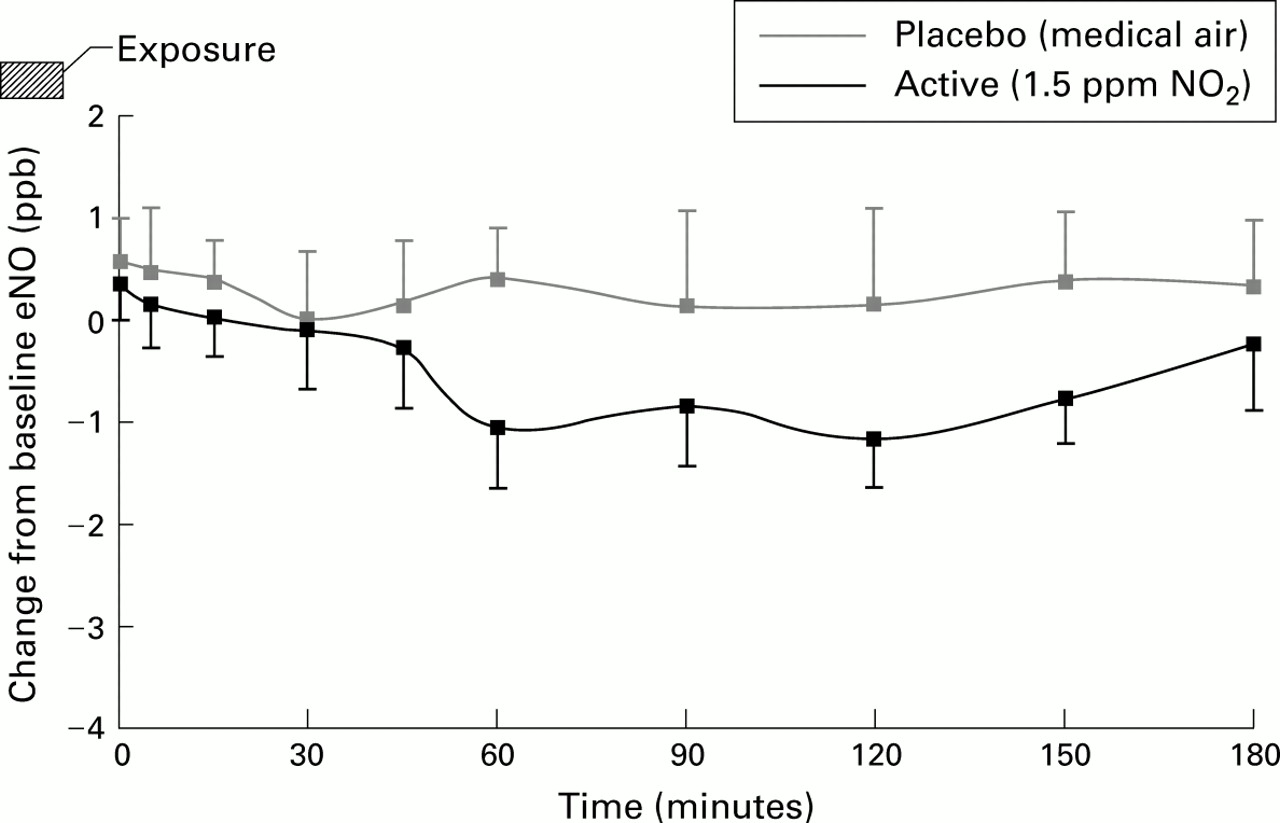
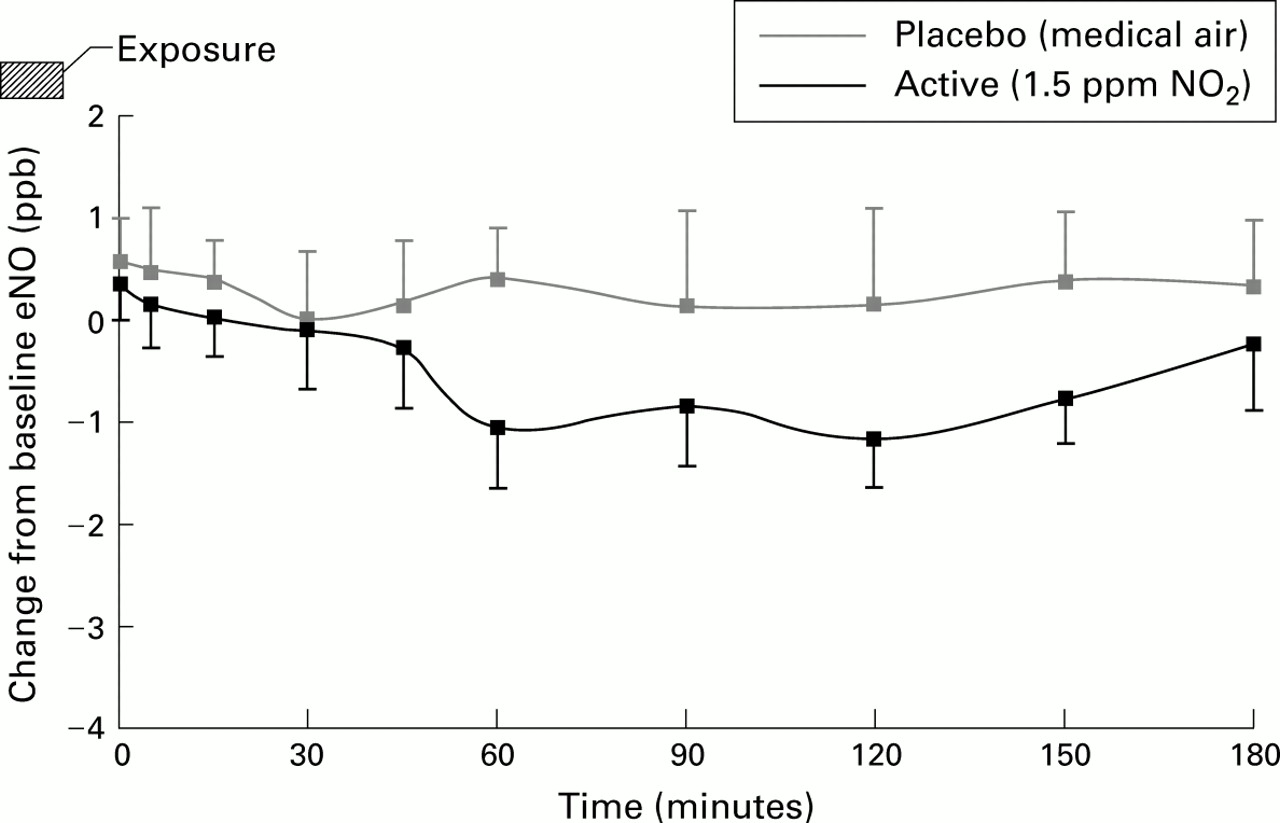
Ten subjects were screened and all completed the study. There was no statistically significant period or order effect, so data have been combined for analysis. The individual data are presented in table 1. Exposure to NO2 induced a mean fall in eNO levels of 0.62 (95% CI 0.32 to 0.92) ppb while exposure to medical air produced no significant change in eNO (0.28 (–0.3 to 0.86) ppb). The reduction in eNO following exposure to NO2 was statistically significant compared with placebo exposure (p<0.01) and fig 1 suggests that the reduction occurred between 60 minutes and 3 hours after exposure. There was no statistically significant change in FEV1 (% predicted) with NO2 exposure compared with placebo exposure.
Baseline data and change in eNO (ΔeNO, parts per billion) following exposure for 20 minutes to placebo (medical air) or to NO2 (1.5 parts per million) in 10 healthy subjects
{kind=link}
Mean (95% confidence interval) change from baseline exhaled NO level (ppb) at each time point following 20 minutes exposure to placebo (medical air) or NO2 (1.5 ppm) in 10 subjects. Time 0 = end of exposure period.
ASCORBIC ACID SUPPLEMENTATION
Twenty five subjects were screened for inclusion. One subject was excluded because of evidence of airways obstruction and four did not complete the study (two non-compliant, one inadvertently commenced additional nutritional supplements, and one unable to attend clinic visits), leaving 20 subjects for study. The serum ascorbic acid concentration following placebo was unavailable for one subject. There was no statistically significant period or order effect, so data have again been combined for analysis. Individual data are presented in table 2. Ascorbic acid supplementation significantly increased the serum ascorbic acid concentration by 7.4 (95% CI 5.1 to 9.7) μg/ml (63%). Placebo supplementation did not significantly alter serum ascorbic acid concentrations. There was no significant change in eNO levels after either active or placebo supplementation (mean change in eNO 0.3 (–0.6 to 1.2) ppb after ascorbic acid and –0.7 (–1.7 to 0.3) ppb after placebo).
Baseline data, change in eNO (ΔeNO, parts per billion) and change in serum ascorbic acid (ΔVit C, μg/ml) following placebo or active (500 mg ascorbic acid bd) oral supplementation (n=20)
Discussion
Exposure to the oxidising gas NO2 (1.5 ppm for 20 minutes) induces a small but statistically significant decrease in eNO which appears to occur 1–3 hours after exposure. These findings are in line with those of Olin et al who described a non-statistically significant decrease in eNO after exposure to the oxidising gas ozone.18 In contrast, oral supplementation with the antioxidant ascorbic acid in a dose sufficient to increase serum ascorbic acid concentrations by 63% had no effect on eNO.
There are several possible explanations for the effect of NO2 on eNO. A number of cytokine responses have been described soon after exposure to NO2. Blomberget al found increased interleukin (IL)-8 in bronchial washings 1.5 hours after a 4 hour exposure to NO2in a concentration of 2 ppm,19 while increased IL-1, IL-6, IL-8 and GM-CSF, IL-8 and tumour necrosis factor (TNF)α production have been described in supernatant after in vitro exposure.20 ,21 Such a mix of pro-inflammatory cytokines is likely to induce the NO producing enzyme nitric oxide synthase (NOS), although this process takes hours and cannot explain the decrease in eNO observed in this study.
Alternatively, NO2 may produce epithelial cell damage or dysfunction, in turn leading to reduced NO production. Devaliaet al reported increased release of51Cr from prelabelled cells (implying cellular injury), attenuation of ciliary beat frequency, and increased movement of14C-BSA across human bronchial epithelial cells in culture (again implying cellular injury) 1 hour after exposure to NO2 in concentrations ranging from 0.1 to 0.8 ppm for 20 minutes.22 It is unclear whether these changes are reversible. Transient epithelial cell damage from NO2exposure could therefore explain our study findings.
There is another possible explanation for the reduction in eNO after NO2 exposure. As described in the introduction, the chemistry of the biologically relevant oxides of nitrogen is highly dependent on local redox conditions.2 NO is likely to react with molecules present in the fluid lining the airway lumen, including superoxide, thiol containing compounds such as glutathione and albumin (to form S-nitrosothiols), and oxygen,2 ,23 so that NO produced by epithelial cells is unlikely to diffuse entirely unhindered into the lumen. Rather, a complex interplay of reactions will occur and the end products will depend on local concentrations of these reactants.8 NO2 will induce changes in this chemical milieu which are likely to impact on the local metabolism of NO.
NO2 undergoes reactive absorption in the ELF of the respiratory tract. The most important substrates for this reactive absorption are ascorbic acid and glutathione.9 ,10 Both are sacrificial for NO2, although Kellyet al reported increased glutathione concentrations in bronchial washings 1.5 hours after a 4 hour exposure to NO2 (2 ppm), possibly reflecting active secretion of glutathione as a response to this high concentration oxidant insult.9 The reactive absorption of NO2 also leads to the formation of superoxide 1 hour after exposure.10 These complex changes in ELF redox state following exposure to NO2 may impact upon the diffusion of NO from epithelial cell to lumen in at least two ways: the increased availability of superoxide in the ELF could reduce the amount of NO appearing in the lumen through a reaction producing the cytotoxic product peroxynitrite, or the excess glutathione produced could lead to the formation of stable nitrosothiols.23 Thus, at least two redox sensitive reactions, both of which have been found to occur over appropriate time courses, could explain the observed decrease in eNO after NO2 exposure.
There is mounting evidence from other sources that ELF chemistry modulates eNO. Marshall and Stamler have suggested that the increased eNO levels observed in asthma may result from increased acidity in asthmatic airways7 rather than from increased NOS induction as had been previously proposed.8 eNO levels are lower in chronic cigarette smokers than in non-smokers,24 ,25 possibly as a result of the increased concentrations of glutathione and other antioxidants in their ELF.26 eNO is lower in patients with cystic fibrosis, despite the increased NOS activity in the airways of this patient group, because NO is metabolised to nitrite in the ELF.6Our laboratory has shown an increase in eNO levels minutes after exposure to cigarette smoke,27 probably mediated through the oxidant effect of the smoke on the ELF.28 More recently we have described an increase in eNO levels after exposure tod-arginine in steroid naïve asthmatic subjects. Sincel-arginine is the substrate for NOS, this effect cannot be mediated through NOS but is likely to represent a local chemical effect of the exposure.29 The results of the current study go further to suggest that alterations in airway chemistry can modulate eNO.
The finding that NO2 exposure reduces eNO levels may have further implications. Exposure to NO2 is known both to increase bronchial hyperresponsiveness and reduce ciliary activity.22 ,30 NO has been found to decrease smooth muscle hyperresponsiveness in the airways31 ,32 and has a role in the control of ciliary activity.33 Since we have demonstrated a decrease in eNO after exposure to NO2, it may be that the effects of NO2 on ciliary function and bronchial hyperresponsiveness are mediated through decreases in the bioavailability of NO, either by chemical consumption or secondary to epithelial cell damage or dysfunction. This possibility requires further investigation.
We found no effect of oral supplementation with ascorbic acid on eNO levels, despite increases in serum ascorbic acid concentrations of 63%. Although dietary manipulation alters the ELF ascorbic acid concentration in guinea pigs,34 a similar effect has not been definitively demonstrated in humans. However, Mohseninet al have described a protective effect of oral ascorbic acid (500 mg qds) on NO2 induced bronchial hyperresponsiveness in humans,35 suggesting that oral supplemental doses of ascorbic acid are able to reach the respiratory tract. Although ascorbic acid can modify the activity of NO in the systemic vasculature4 ,5 and aids in the conversion of the NO metabolite nitrite back to NO in vitro,36 our results would suggest that ascorbic acid has no significant effect on the ELF metabolism of NO in vivo.
In summary, ascorbic acid supplementation for 2 weeks at a dose of 500 mg twice daily does not affect eNO levels in healthy human subjects. On the other hand, exposure to NO2, 1.5 ppm for 20 minutes, causes a small but statistically significant decrease in eNO levels. This observation provides a possible mechanistic link between exposure to NO2 and resulting bronchial hyperresponsiveness and decreased epithelial cell ciliary activity which requires further investigation.
Acknowledgments
The authors thank Quest Vitamins Ltd, Aston Science Park, UK for their support and for supplying both the ascorbic acid and placebo.