Article Text

Abstract
OBJECTIVES Though atrial fibrillation (AF) is an important cause of cardiovascular morbidity, there are few large epidemiological studies of its prevalence, incidence, and risk factors. The epidemiological features of AF are described in one of the largest population cohorts ever studied.
METHODS The prevalence and incidence of AF were studied in the Renfrew/Paisley population cohort of 15 406 men and women aged 45–64 years living in the west of Scotland. This cohort was initially screened between 1972 and 1976 and again between 1977 and 1979. Incident hospitalisations with AF in the 20 year period following initial screening were also studied.
RESULTS The population prevalence of AF in this cohort was 6.5 cases/1000 examinations. Prevalence was higher in men and older subjects. In those who were rescreened, the four year incidence of AF was 0.54 cases/1000 person years. Radiological cardiomegaly was the most powerful predictor of new AF (adjusted odds ratio 14.0). During 20 year follow up, 3.5% of this cohort was discharged from hospital with a diagnosis of AF; the rate of incident hospitalisation for AF was 1.9 cases/1000 person years. Radiological cardiomegaly (adjusted odds ratio 1.46) and systolic blood pressure (adjusted odds ratio 2.1 for ⩾ 169 mm Hg) were independent predictors of this outcome.
CONCLUSIONS Data from one of the largest epidemiological studies ever undertaken confirm that AF has a large population prevalence and incidence, even in middle aged people. More important, it was shown that the long term incidence of hospitalisation related to AF is high and that two simple clinical measurements are highly predictive of incident AF. These findings have important implications for the prevention of AF.
- atrial fibrillation
- epidemiology
- systolic blood pressure
- cardiac volume
Statistics from Altmetric.com
Though atrial fibrillation (AF) is an important cause of stroke, heart failure, and death, few large population based epidemiological studies have reported its prevalence and, particularly, incidence. The two largest studies have been carried out in the USA. The Framingham heart study started biennial examination of 5070 men and women aged 28–62 years and free of cardiovascular disease in 1948.1 The cardiovascular health study examined 5201 adults aged 65 years or older annually, on four occasions, between 1989 and 1993.2 ,3
The Renfrew/Paisley study is one of the largest epidemiological studies ever undertaken. Its population cohort of 15 406 middle aged men and women residing in the west of Scotland were initially examined between 1972 and 1976 and then re-examined between 1977 and 1979.4 ,5 Using the unique and accurate Scottish record linkage system, we have been able to identify all hospitalisations and deaths occurring within this large cohort over the 20 years after their initial examination.6
Using these data, we report the population prevalence and incidence of AF in this (initially) middle aged cohort. We also report the rate of incident hospitalisations associated with a diagnosis of AF during 20 years of follow up. In addition, we describe the characteristics of subjects with and without baseline AF and the predictors of the subsequent development of AF in those in sinus rhythm at their initial examination. These data are important in providing a more contemporary and comprehensive European perspective on this important problem, especially as the epidemiology of cardiovascular disease can vary geographically and over time. This information is also important in understanding how AF and its associated morbidity might be prevented.
Methods
STUDY POPULATION
All data concerning the epidemiological features of AF were obtained from the Renfrew/Paisley study; the purpose, design, and methods of which have been published previously.4 ,5
This study examined middle aged men (n = 7052) and women (n = 8354) residing in a compact urban area comprising the two towns of Renfrew and Paisley in the west of Scotland. During 1972–6, 80% of the target population aged 45–64 years was screened. During 1977–9, a mean (SD) of 4.1 (.75) years following initial screening, about 60% of survivors (8532 subjects) were rescreened.
BASELINE DATA
During baseline screening, subjects completed a battery of health questionnaires and diagnostics tests examining their health status and subsequent risk of developing cardiorespiratory disease. In addition to basic demographic data, each subject's social class was determined by their current occupation using the Registrar General's classification (manual social class was defined as social classes IIIM to V).7 The extent of deprivation was determined by the Carstairs deprivation index.8 The Rose angina questionnaire was used to determine the presence of angina pectoris (classified as none, possible or definite).9Evidence of chronic bronchitis was assessed using the Medical Research Council's bronchitis questionnaire.10 Subjects were also asked about their medical history and current status. This included questions about the presence of or previous treatment for cardiorespiratory disease states such as hypertension, asthma, diabetes, and stroke in addition to known risk factors for the development of cardiorespiratory disease (for example, a detailed smoking history was obtained). Subjects were also asked whether they had symptoms indicative of transient cerebral ischaemia (sudden but transient loss of power to limbs or dysphasia). A physical examination with measurement of blood pressure and height and weight (to enable calculation of body mass index in kg/m2) was undertaken. Chest radiography and vitalography were also performed to calculate cardiothoracic ratio and forced expiratory volume in one second (FEV1). Cardiomegaly was defined as a cardiothoracic ratio of ⩾ 0.55. An adjusted FEV1 score was calculated as a percentage of the “expected” FEV1 score (derived from a linear regression equation of age and height for men and women separately from a healthy subset of the population who were non-smokers and had no respiratory symptoms) and the actual FEV1score.11 A non-fasting venous blood sample was also obtained for the measurement of plasma cholesterol (mmol/l) and glucose concentration (mmol/l). It should be noted, however, that not all participants were subject to every diagnostic test.
ATRIAL FIBRILLATION DETECTED AT SCREENING
During screening, a baseline six lead ECG was recorded. ECGs were subsequently classified by a cardiologist according to the Minnesota coding system.12 All cases of AF (Minnesota code 8.3) and ECG abnormalities indicative of past myocardial infarction (MI), active myocardial ischaemia, and left ventricular hypertrophy were also identified.
INCIDENT HOSPITALISATION DURING 20 YEAR FOLLOW UP
All subjects within the Renfrew/Paisley cohort who were discharged from hospital within 20 years of their original screening date with a diagnostic coding of AF (International classification of diseases, ninth revision (ICD-9) 427.3 or the equivalent ICD-8 coding for AF before 1978, in any one of six coding positions) were identified.13 These data obtained were directly from the Information and Statistics Division of the National Health Service in Scotland, which collects and collates data on all hospital discharges, on an individual basis, through the Scottish Morbidity Record Scheme.6 Regular auditing of these data suggests that coding data are 90% accurate overall.14
STATISTICAL ANALYSIS
The population prevalence of AF was calculated as the number of detected cases per 1000 examinations. The population incidence of AF was calculated as the number of new cases per 1000 person years of follow up in those in sinus rhythm at initial screening and who were subject to a re-examination. The rate of incident hospitalisation for AF was calculated as the number of new cases per 1000 person years during 20 years' follow up of the entire cohort.
Baseline characteristics of subjects with and without AF at baseline were compared on an age adjusted basis. Categorical variables were age standardised by the direct method using the male and female study populations as the standards, and age adjusted means for continuous variables were calculated using PROC GLM of the SAS system (SAS Institute Inc, Cary, North Carolina, USA).
Multiple logistic regression models were constructed using the initial entry of all variables and stepwise rejection of variables using a significance threshold level of p < 0.05. For each categorical variable in the model, the lowest class was set at unity and all adjusted odds ratios (OR) and 95% confidence intervals (CI) are relative to this class. To evaluate the influence of a large number of missing data for cardiothoracic ratio and blood glucose concentration (n = 675 and 4703, respectively) separate models were constructed in their presence and absence. Except for that mentioned above, all analyses were performed using SPSS for Windows (version 9.0) (SPSS Inc, Chicago, Illinois, USA).
Results
PREVALENCE OF ATRIAL FIBRILLATION
Analysis of ECG data for the original cohort of men and women aged 45–64 years (n = 15 406) found 100 (0.65%; 95% CI 0.53 to 0.79%) documented cases of AF.
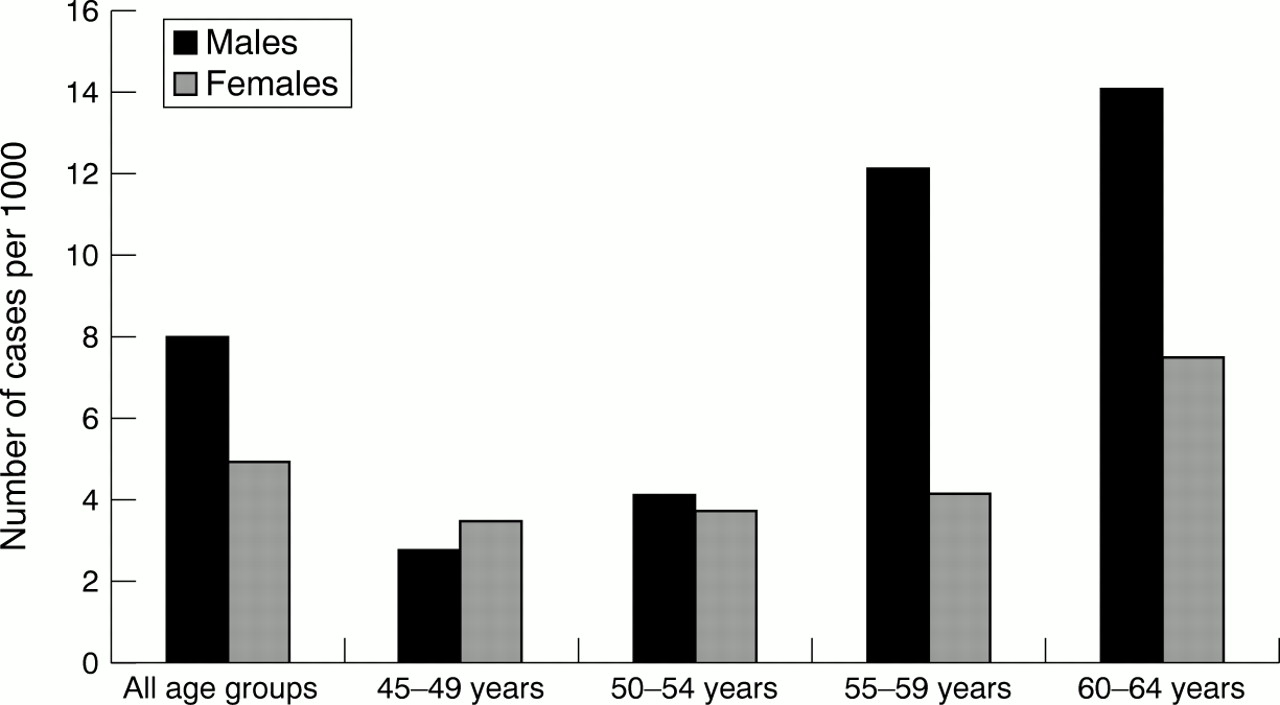
Prevalence of AF increased with age and there were more cases detected in men (53 of 7052) than women (47 of 8354). In the subset of subjects who participated in the second survey of this cohort (n = 8532) there were 46 (0.54%, 95% CI 0.40 to 0.72%) documented cases of AF. Figure1 summarises the overall prevalence of AF according to age and sex using the combined data from the two screening periods.

Age and sex specific prevalence of atrial fibrillation (AF) in a population cohort from the west of Scotland.
DEMOGRAPHIC AND CLINICAL ASSOCIATES OF ATRIAL FIBRILLATION
Table 1 shows the characteristics of this population cohort at baseline according to the presence or absence of AF on an age adjusted basis. Both men and women in AF were older and more likely to have a history of stroke, symptoms indicative of possible transient cerebral ischaemia, ECG evidence of myocardial ischaemia, and left bundle branch block and cardiomegaly as determined by chest radiography. They were also more likely to have a lower adjusted FEV1. Women but not men in AF were found to have higher diastolic blood pressure and blood sugar concentrations, lower total cholesterol concentrations, and a history of angina, and were more likely to have ECG evidence of left ventricular hypertrophy. Men but not women in AF were more likely to have symptoms indicative of chronic bronchitis and ECG evidence of past MI (pathological Q waves) and to come from a manual social class. Of the 100 subjects with AF, 13 reported exertional dyspnoea with all 13 fulfilling the Medical Research Council criteria for chronic bronchitis.11
Age adjusted characteristics of the cohort according to the presence or absence of atrial fibrillation (AF) at baseline
Table 2 summarises the independent correlates of AF according to baseline screening data. Male sex, a history of stroke, and ECG evidence of myocardial ischaemia were independently associated with AF. Overall, however, cardiomegaly was the strongest correlate of AF. When this variable was excluded from the model, older age also appeared to be independently associated with AF (OR 2.1, 95% CI 1.1 to 10.2 per decade, p < 0.05).
Independent correlates of AF at baseline
INCIDENCE OF ATRIAL FIBRILLATION DETECTED AT FOLLOW UP SCREENING
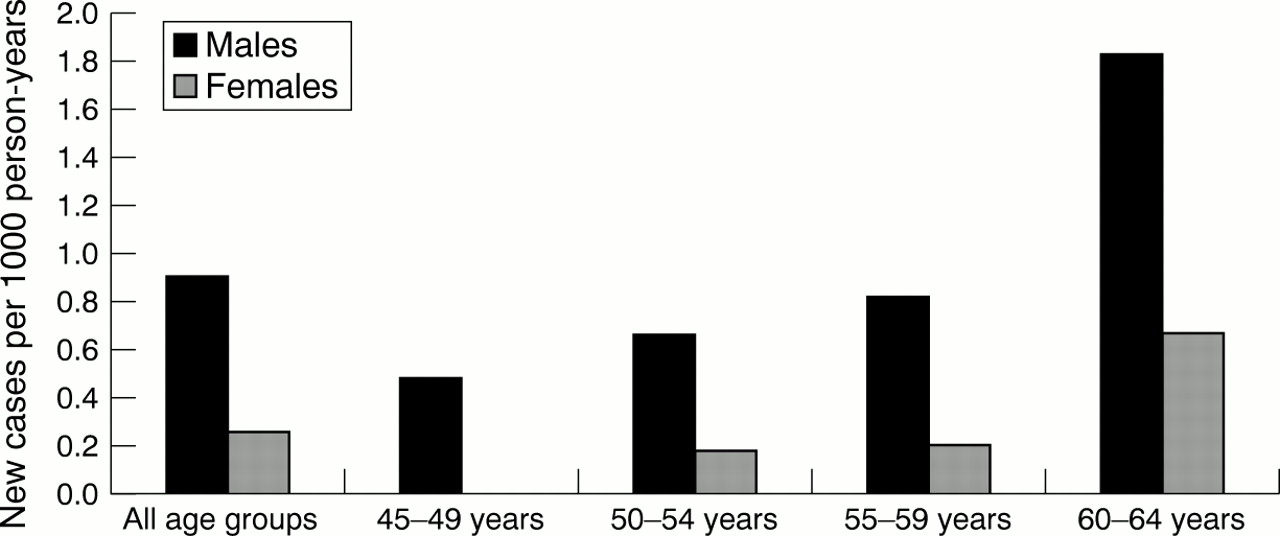
Of the 8532 subjects who participated in the follow up screening of the Renfrew/Paisley cohort, 14 men and five women had newly documented AF. Figure 2 shows the age (based on age at first screening) and sex specific rate of incident cases of AF per 1000 person years of follow up. The rate of incident cases increased notably with age and was greater in men than in women. Paired analysis of data collected during the first and follow up examinations found no significant changes in systolic and diastolic blood pressure, cardiothoracic ratio, blood sugar concentration, plasma cholesterol concentration, and adjusted FEV1 for those who developed new AF. For example, of the 19 subjects with new AF, eight had radiographic cardiomegaly detected on both occasions. However, four subjects reported new angina pectoris. Thus, 12 of 19 subjects with new AF had a history of angina. Five (including the four with new onset angina) subjects had newly documented myocardial ischaemia on their repeat ECG. Although two subjects no longer had ECG changes indicative of myocardial ischaemia during the second survey, 13 of the 19 subjects with newly documented AF had some manifestation of myocardial ischaemia (angina or ECG changes) during the second examination. Moreover, five subjects reported new symptoms indicative of transient cerebral ischaemia (making a total of six subjects with this problem), though there were no new cases of stroke.

Rate of new incident cases of AF detected during rescreening of 8532 men and women (34 891 person years of follow up). (Age groups are based on age at baseline.)
INDEPENDENT PREDICTORS OF INCIDENT ATRIAL FIBRILLATION
According to the multivariate analysis, male sex (OR 3.4, 95% CI 1.1 to 10.2), greater age (OR 1.29, 95% CI 1.2 to 1.4/decade), and cardiomegaly (OR 14.0, 95% CI 5.1 to 10.2) were the only independent predictors (p < 0.05) of new AF. In the absence of cardiomegaly, all of the above variables were retained in the logistic regression model, with the addition of ECG evidence of myocardial ischaemia (OR 4.1, 95% CI 1.2 to 14.2) detected at baseline.
INCIDENT HOSPITALISATIONS ASSOCIATED WITH A DIAGNOSIS OF ATRIAL FIBRILLATION
As the age of the Renfrew/Paisley cohort ranged from 45–64 years at baseline, we were able to document incident hospitalisations for AF in this cohort up to the age of 84 years. During the first four years of follow up of the original Renfrew/Paisley cohort we found that five of the 19 subjects with new AF were hospitalised. All were coded at discharge with a diagnosis of AF. There were no hospitalisations associated with a diagnosis of AF in subjects without AF who had a follow up examination.
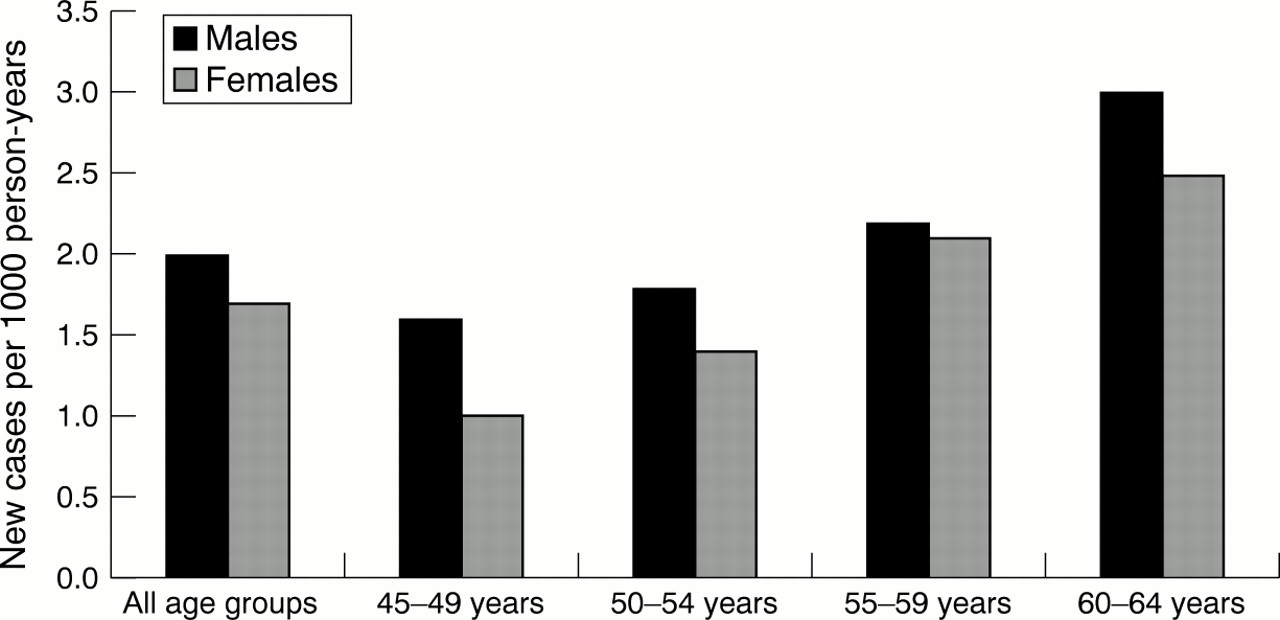
During 20 years follow up, 255 of the 6999 men (3.6%, 95% CI 3.2% to 4.1%) and 282 of the 8307 women (3.4%, 95% CI 3.0% to 3.8%) in the Renfrew/Paisley cohort without AF at baseline were discharged from hospital with a diagnosis of AF. The proportion of men for whom such a hospitalisation was recorded increased from 3.3% (95% CI 2.5% to 3.2%) in those initially aged 45–49 years to 4.2% (95% CI 3.3% to 5.4%) in those aged 60–64 years. The equivalent figures for women were 2.3% (95% CI 1.7% to 3.0%) and 4.4% (95% CI 3.5% to 5.4%), respectively. Figure 3 shows the age and sex specific rates of incident hospitalisations with AF per 1000 person years of follow up.

{kind=link}
{kind=link}
{kind=link}
Rate of incident AF hospitalisation in 15 306 men and women during 20 year follow up. (Age groups are based on age at baseline.)
Overall, this cohort recorded 808 hospitalisations where AF was coded in any position during 20 years follow up (38% of these as the principal diagnosis). The most common concurrent diagnoses (coded in any position at discharge) were heart failure (38%), coronary artery disease other than MI (34%), stroke (23%), and MI (14%). Valvar heart disease was documented in approximately 7% of cases, while thyroid disease was documented in < 1.5% of cases.
INDEPENDENT PREDICTORS OF INCIDENT HOSPITALISATION WITH ATRIAL FIBRILLATION
Table 3 shows the independent predictors of incident hospitalisation with AF based on original screening data in patients not found to be in AF at baseline (n = 15 306). Once again, age and cardiomegaly were independent predictors for new AF detected in this manner, although there was little difference between men and women. Other predictors were a history of symptoms indicative of angina and a higher systolic blood pressure recorded at baseline. In the absence of cardiomegaly, a higher body mass index was also retained in the final model. Not surprisingly, subjects who were in AF at baseline were also about three times more likely to be hospitalised with a diagnosis of AF during follow up (15%; adjusted OR 2.9).
Independent predictors of incident AF hospitalisation during 20 year follow up
Discussion
Using data from one of the largest and most contemporary population based epidemiological studies and incorporating a unique system for accurately identifying hospitalisations over a prolonged period, the present study is one of the largest and most comprehensive analyses of the epidemiological features of AF in middle age onwards. In particular, we have been able to identify two simple clinical predictors of future AF, which has implications for prevention of AF and its associated mortality and for our understanding of the relation between systolic blood pressure and the risk of stroke.
PREVALENCE OF ATRIAL FIBRILLATION: COMPARISON WITH PREVIOUS STUDIES
Our findings are in keeping with those of the Framingham heart study, which found an initial screening prevalence of 5/1000 in those aged 50–59 years and rising to 18/1000 in those aged 60–69 years.1 ,15-18 The prevalence rates in subjects aged 50–59 years in the Renfrew/Paisley cohort were 7.2/1000 in men and 2.9/1000 in women. The male and female rates in those aged 60–69 years were 10.2 and 7.4/1000, respectively, somewhat less than in Framingham. Our findings are also agreement with reports from Denmark,19 Iceland,20 and the Netherlands21 that have described smaller populations.
INCIDENCE OF ATRIAL FIBRILLATION: COMPARISON WITH PREVIOUS STUDIES
Of more interest are our data on the incidence of AF because of the paucity of data in this regard. The Framingham heart study reported two yearly incidence rates of approximately 1.9 and 0.9/1000 person years in men and women, respectively, aged 50–59 years.1 ,15-18 Our equivalent rates over four years in those aged 55–64 years were 1.31 and 0.44/1000 person years. Over 38 years of follow up, the Framingham study found an overall incidence of approximately 3/1000 person years in men and 2/1000 person years in women aged 55–64 years.1 We observed a 20 year rate of incident hospitalisation with AF of 2.1 and 1.7/1000 person years in men and women, respectively, in this age range.
The only other incidence study encompassing subjects in the same age range and with long term follow up is the Manitoba follow up study in Canada, which examined 3983 male aircrew recruits with an average age of 31 years in 1948.22 These subjects were followed for 44 years. The incidence rate was 2/1000 patient years overall, being as low as < 0.5/1000 before the age of 50 and rising to 2.3/1000 person years by the age of 60 years.
INCIDENT HOSPITALISATION OVER 20 YEARS
Our rate of incident hospitalisation for all men over 20 years' follow up was 2.0/1000 person years. This almost certainly is an underestimation of its true incidence because we had no means to detect AF in those who avoided hospitalisation. Consequently, our population incidence over 20 years is likely to have been higher than the hospitalisation rates and, therefore, higher than in either the Framingham.1 ,15-18 or Manitoba cohorts.22This is, perhaps, not surprising with regard to the Canadian study, which recruited fit young men, whereas our cohort was unselected and from a population with a high rate of coronary and other cardiovascular disease.4 Interestingly, however, it seems that although we found a lower initial prevalence than Framingham, our subjects went on to have a higher long term incidence, again presumably reflecting the impact of other cardiovascular diseases in later years.1 ,15-18 Indeed, one of the most important findings of our study is the high burden of incident hospitalisation related to AF, with 3% of men and over 2% of women aged 45–49 years at baseline going on to experience such an event in the subsequent two decades of follow up.
CORRELATES OF ATRIAL FIBRILLATION
We were also able to examine the baseline demographic and clinical features of subjects with and without AF and the independent correlates of AF in this population cohort. As in other studies, we found male sex and existing cardiovascular disease to be independently correlated with AF. We also found chronic lung disease and, in particular, cardiomegaly to be important. We found hyperglycaemia to be a much stronger correlate than in the cardiovascular health study.2 ,3
PREDICTORS OF NEW ATRIAL FIBRILLATION
Of more interest are the predictors of new AF. Here we found age and sex to be important independent predictors, as in other reports. We observed a doubling of risk for each decade of age, in close agreement with the Framingham investigators' findings.1 However, we have also been able to show that cardiomegaly, on the chest radiograph, is by far the most powerful predictor in the multivariate analysis, an observation not made previously. In the Framingham study, heart failure and ECG determined left ventricular hypertrophy were the most powerful predictors of incident AF with a four- to sixfold increase risk due to the former and a three- to fourfold increased risk from the latter.1 A later cohort of 1924 subjects aged 50–94 years did undergo echocardiography in the Framingham study, and left atrial size, reduced fractional shortening, and wall thickness were found to increase modestly the risk of developing AF.15-18 In contrast, we found that radiological cardiomegaly led to a 14-fold increase in the likelihood of new AF. These findings support the view that cardiothoracic ratio is a simple and powerful predictor of adverse cardiovascular outcomes.23 ,24 Therefore, patients with radiological cardiomegaly should, if not already under regular review, be kept under close surveillance from the point of view of their heart rhythm (and, in any case, merit further cardiological investigation).
Though this population cohort was rescreened only once, after four years, importantly, we have also been able to obtain information on incident hospitalisations with AF for up to 20 years. Clearly, these data underestimate the true incidence of new AF in our population, as mentioned earlier. Nevertheless, this manifestation of AF is clearly of interest. Once again, age and cardiomegaly were important predictors, though the latter was much less powerful a predictor for this outcome in the longer term. Of considerable interest was the finding that systolic hypertension was an independent predictor of hospitalisation with AF, approximately doubling the chances of this event. These data are difficult to interpret. Though each hospitalisation had a discharge coding of AF, it was usually a secondary diagnosis. In the approximately 800 such hospitalisations accumulated over 20 years, AF was the principal diagnosis in 38% of cases, the most frequent other principal diagnoses being heart failure (11%), MI (9%), and stroke (7%). The predictive relation we have described may, therefore, merely reflect an indirect association between systolic blood pressure and AF—for example, the association between systolic blood pressure and MI, and MI and AF. If, however, there is a direct relation, this may be of considerable importance and raises a number of interesting questions. Can AF account for some of the relation between systolic blood pressure and stroke or heart failure? This certainly seems to be an area for further investigation.
STUDY LIMITATIONS
As with any large epidemiological study, there are limitations to our analysis. Baseline information on valvar heart disease and chronic heart failure, both important causes of AF, was not collected. It should be noted, however, that only 13% of subjects with AF reported exertional dyspnoea at the time of screening, all of them fulfilling the criteria for chronic bronchitis. Moreover, only three subjects were hospitalised with heart failure within three years of screening and only a small proportion of hospitalisations for AF (< 5%) were associated with a concurrent diagnosis of valvar heart disease. In the majority of cases, a single ECG recording was made, meaning that it was not possible to differentiate between paroxysmal and sustained AF, though this limitation is true of other studies also. These data also do not provide information concerning treatment. Lastly, the potential influence of selection bias (in favour of healthier people) as part of the rescreening process is an important caveat when considering incidence data.
CONCLUSIONS
In summary, the prevalence of AF in Scotland is similar to that in comparable age groups in other countries. The incidence of AF is also similar, although in the short term (four years) only about a quarter of these cases are associated with a hospital discharge related to AF. In the longer term (20 years) almost 4% of middle aged men and women will have an incident hospitalisation associated with AF. The most powerful predictor of the future development of this arrhythmia is radiological cardiomegaly, which increases the adjusted risk 14-fold in the short term and 2.5-fold in the longer term.
Acknowledgments
Simon Stewart is supported by the National Heart Foundation of Australia. Carole Hart was supported by grants from Chest, Heart, and Stroke Scotland and the Stroke Association.
We gratefully acknowledge the contribution of Pauline MacKinnon, who is responsible for updating and maintaining the Renfrew/Paisley cohort database. Victor M Hawthorne and Charles R Gillis were responsible for the original Renfrew/Paisley study.