Article Text

Abstract
Objectives: To determine if youth football officials responsible for dealing with injuries have appropriate first aid qualifications and knowledge?
Methods: Information was collected from two youth football leagues by questionnaire. First aiders were asked to provide details of their qualifications and their response from a list of alternatives to an injury scenario.
Results: Fifty two of 86 respondents did not have a current first aid qualification. Only 12% and 38% respectively gave the correct response to the injury scenarios “player choking” and “player unconscious”. Health and injury records for the players were kept by 40% and 19% of teams. Written parental consent to emergency treatment was obtained by 30%.
Conclusion: This preliminary study shows an obligation on teams who do not possess a qualified first aider to evaluate their legal and moral responsibilities to their players. The Football Association and Health and Safety Executive should produce a list of recommended equipment, facilities, and first aid qualified personnel to which teams should have access at games and training sessions. Providers of first aid training should reassess their teaching of the management of the choking and unconscious casualty.
- first aid
- football
- youth leagues
- audit
- qualifications
Statistics from Altmetric.com
Many children enjoy sport and place great emphasis on “having fun”.1 This enthusiasm needs be channelled into safe and challenging activities that will both help to address the increasing hypokinetic lifestyle of many children and improve and extend the skills base from which competent and elite athletes will emerge.
Physical activity is important to stimulate normal physical growth. The positive stimulatory effects of physical exercise outweigh the potential negative risks of injury and growth related illness.2 However, it is essential that, if injury does occur, it is appropriately managed. Trained first aiders are pivotal to the successful primary care of injuries. The International Federation of Sports Medicine advises that, where medical supervision is inadequate, damage to health can occur.
A study of the health care available to high school football players (American football) reported a high level (80%) of medical coverage at games and training.3 Little research on the medical care available in amateur sport in the United Kingdom has been published. I found no reports on the numbers of qualified first aiders in football, their level of competency, or their procedures for recording injuries and accidents.
All coaches and adults who organise youth sport have a legal duty of care towards their athletes. Sports Coach UK (2001) have issued a code of ethics and conduct. This sets out basic ethical and personal principles together with standards of behaviour. However, it fails to explicitly recommend the possession of a current recognised first aid qualification. The absence of a qualification may breach the spirit of the principle “coaches must attain a high level of competence through qualifications and a commitment to ongoing training that ensures safe and correct practice.”
Adults responsible for young footballers may be breaching both their duty of care and the code of conduct if they are not trained in first aid or fail to keep basic records on health and injuries.
This study attempted to answer the following questions.
What is the prevalence of appropriate first aid qualifications among youth football officials responsible for dealing with injuries?
Which is the most common first aid qualification?
What is the prevalence of medical and injury record keeping?
Is there a difference in the first aid knowledge between coaches who currently hold a first aid qualification and coaches who do not?
Youth football is essentially a safe activity. Peterson et al4 estimated there to be only 6 and 11 injuries per 1000 playing hours for high level and low level youth players respectively. Schmidt-Olsen et al5 reported the rate of injury to be 3.7 per 1000 hours for players aged 12–18. Junge et al6 broadly supported their findings. The American Academy of Pediatrics7 in their subject review reported injury rates of 0.6–19 per 1000 hours depending on the age and skill level of the players. The difficulty in establishing a consistent injury rate is due to different methods of investigation, incongruous injury definitions, and the characteristics of the subject groups used. It is clear though that the rate of injury is low. However, injuries do occur and it is important that the initial advice and treatment is appropriate. First aid knowledge and skills are important assets that coaches and team officials should possess.
METHODS
Survey sample
A total of 250 questionnaires and letters of explanation were sent to secretaries of youth football clubs from a northern and midlands based youth football league for distribution to officials responsible for dealing with first aid at competitive games and in training. Three age groups were considered: 8–11; 12–13; 14–15.
Survey questionnaire
The questionnaire was divided into three sections. Section A requested basic data on the officials and identified trends related to age, years spent coaching, and first aid qualifications held either currently or having lapsed.8 The reasons for qualifications having lapsed were also investigated.
Section B sought data on the medical consumables and equipment available to the club. Supplementary information on whether clubs collected information on players' personal health, injury record, and parental consent to allow emergency treatment was also recorded.
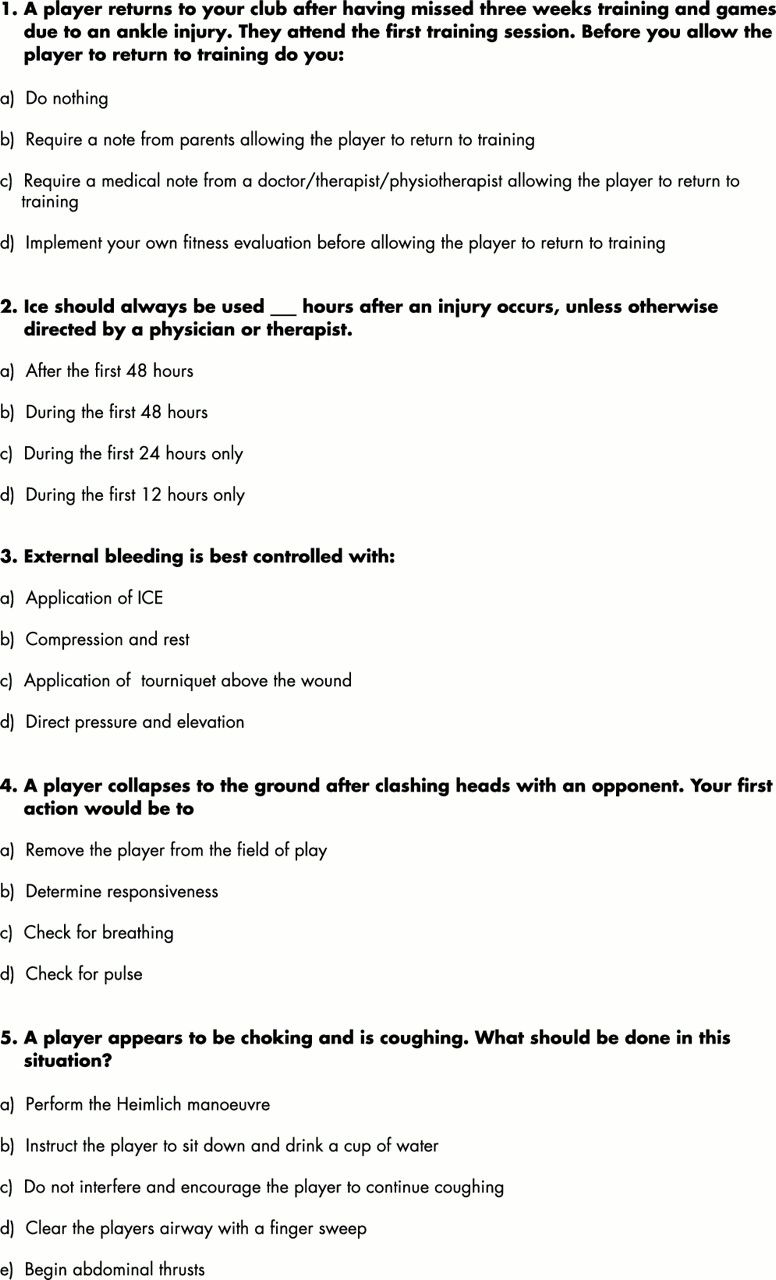
Section C asked first aiders to choose a response from a list of alternatives to an injury scenario (fig 1⇓). Validity and reliability of the injury scenarios and the appropriate response were established by expert review from a panel of physiotherapists and sports therapists currently treating sports injuries who all held a current first aid qualification.

Injury scenario questions in section C of the questionnaire.
Section D surveyed a list of injuries and requested first aiders to list those injuries/illnesses that they felt they could manage competently.
The questionnaire was piloted on 20 local teams. Team managers were asked to report any ambiguities in questions or the format of the questionnaire. Revisions were made on the basis of their responses.
The university ethics and standards committee approved all procedures.
Statistical analysis
All data were processed using the Statistical Package for the Social Sciences (SPSS version 9.0; Chicago, Illinois, USA). Methods applied were frequencies and cross tabulation. Differences between those who held a current first aid qualification and those who did not were examined by the χ2 test; the level of significance was 5%.
RESULTS
A total of 250 questionnaires were administered, and 86 were returned, a response rate of 34%. This preliminary study was designed to ascertain if there is a problem with a lack of first aid knowledge and experience in youth football. Further financial and secretarial support would allow a larger cohort to be surveyed. The low response rate may indicate a reluctance to return questionnaires from non-qualified adults.
Nearly three quarters of first aiders who responded to the questionnaire had been involved in football for up to 10 years, with almost half of the replies coming from those who were involved in the younger age group of 8–11 years.
First aid qualifications held
Over half of the respondents (61%) reported that they did not possess a current first aid qualification. Most first aid qualifications held were sports specific. Almost one third of the respondents (n=13) who reported possessing an FA qualification held the FA Emergency Aid Certificate.
First aid equipment
Generally the respondents rated their consumable supplies as being very good or satisfactory. Over three quarters of the teams spent between £10 and £25 per season on consumables. Table 1⇓ lists the consumables commonly carried and equipment available at the playing venue.
First aid equipment items present within first aid kits and at the venue
All the teams had first aid equipment available at every game, and only 8% (n = 7) failed to take equipment to every training session.
Medical record keeping
Health records were kept by 41% (n = 35) of teams, but specific injury reporting records were only kept by 19% (n = 16). Written parental consent to emergency treatment was recorded in 30% (n = 26) of the teams.
Confidence to treat injuries
Each respondent was given a list of injuries and asked to indicate those that they felt capable of dealing with. Most respondents were happy to deal with simple cuts and bruises, nose bleeds, muscle strains, and minor bleeding.
Three quarters (n = 72) felt that they would not be competent to manage a diabetic attack, and almost half (n = 47) indicated an inability to manage an asthmatic attack. Over half (n = 53) reported a perceived lack of competency in treating a fracture, and slightly more than half (n = 53) indicated an inability to deal with an epileptic attack.
Injury scenarios
If a player was returning to training after injury, 65% of respondents, including those with and those without a qualification (n = 21 and n = 35 respectively), stated that they would perform their own fitness evaluations. A minority of respondents reported that they would require a medical note from a recognised doctor/therapist (n = 7) or a letter from parents (n = 10) before allowing the player to resume training.
More of those respondents who held a current first aid qualification gave the correct response to the “use of ice”, “player collapsing”, and “player choking” injury scenarios. Correct response percentages to the “external bleeding scenario” were very similar between the qualified and non-qualified.
Those who held a current first aid qualification were more likely to give the correct response to the “player collapsing” injury scenario (p = 0.04).
Most respondents, irrespective of whether or not they had a qualification, incorrectly answered the “player choking” injury scenario (72% and 88% respectively). Fifty three respondents indicated that they would use a finger sweep in dealing with a player who was choking but coughing and therefore breathing.
Half of respondents (n = 42) indicated that they would be willing to pay £10–£20 to attend a first aid course. Only a minority (n = 7) said that they would pay over £30.
DISCUSSION
There is little published evidence on the absolute number and rate of sport related injuries in children in the United Kingdom. The literature reviewing sports injury rates in children is mainly attributed to North American and Scandinavian authors, except for two important studies by Watkins and Peabody9 and Williams et al.10 Consequently there is a bias, particularly in the North American studies, towards baseball, American football, and basketball.
Bijur et al11 described the morbidity of sports and recreational injuries in adolescents in the United States. They estimated that sport accounted for 36% of injuries from all causes and 33% of all the serious injury episodes. The rate and seriousness of injuries increased as children got older. Boys (3/100) had higher injury rates than girls (1.3/100). The most common injury was a sprain (60%) followed by fracture and dislocation (48%). Many of these injuries were associated with bicycles, falls from playground equipment, and skateboards. Unfortunately, this study did not distinguish between the injuries occurring in different sports, and it relied on retrospective parental reporting. Schuller and Kopjar12 reported that 34% of injuries reported in schools were the result of sporting activities among the age group 7–12 rising to 60% in the older age group (13–15).
Sports related injuries in the United Kingdom
Williams et al10 measured the age and sex distribution of self reported sports and leisure injuries over a 12 month period. Some 42% reported a medically attended injury, with 33% of these being sports related. Over half (54%) had to miss school as a result of the injury. Most injuries from formal and informal sports were sprains and strains (34% and 30%) and fracture (32% and 36%). Boys were more likely to sustain an injury than girls, with the injury more likely to be severe. One interpretation of these figures lies in the type of activity popular with the different sexes. Boys are more likely than girls to engage in contact sports and are therefore more prone to traumatic and extrinsic injury. As children age, they are also more liable to sustain an injury. These results support the work of Bijur et al11 and Schuller and Kopjar12 who reported similar injury rates.
Williams et al10 concluded that sports injuries were common at this age and strategies for preventing sports specific injury should be developed.
There is also concern about the possible long term damage of intensive training to elite young sportspeople. The Sports Council instigated a prospective survey of sports injuries to intensively trained young people (TOYA study 1994).12 The highest rates of injury were found in football players, but overall the injury rate was not deemed to be high.
A practical measure to prevent sports injuries becoming chronic and affecting school attendance is to provide safe and effective primary care—that is, competent first aid treatment and advice at the time of injury.
Football injuries in youth players
There are few papers on the incidence of football injuries in youth players. This may be because injury rates are assumed to be low and most injuries are minor and self limiting. Peterson et al4 reported on the effects of skill level and the incidence of injury over a one year period. Over 80% of the players were injured, most being injured more than once. The rate of severe injury (symptoms lasting for four or more weeks) was 29%. The average number of injuries per player was two. Most were sprains (54%) and strains (34%) to the lower extremity, with the knee being the most commonly injured site (46%). Almost 30% of injuries were the result of foul play.
The American Academy of Pediatrics in their Policy Statement7 on “Injuries in youth soccer” reviewed the common types and causes of injury. They reported that 45% of all football injuries occurred to players younger then 15. The most common type of non-fatal injury was a soft tissue contusion. Other soft tissue injuries, such as sprains, contusions, fractures, dislocations, and overuse injuries, did occur but not disproportionately. Lower limb injuries accounted for 61–80% of all injuries. Two of their main recommendations were that doctors should encourage increased participation in all forms of physical activity and they should look at how football can be made safer through “rule changes, equipment modifications and other safety interventions”.
Kibler13 conducted a prospective study to examine the incidence, injury type, causes, and effect on playing status in an invitational football tournament over a period of 480 games in four years. He reported an injury rate of 23.8/10 000 playing hours, with the predominant injuries being sprains and strains. In keeping with other studies,4,9,10,14 the lower extremity was the prevalent site of injury, and, as expected, most injuries were the result of a collision. He concluded that injuries were usually mild and that “soccer is a relatively safe sporting activity for youth”. However, he did recommend that provision be made for equipment to deal with common injuries and that provision for emergency care needs to be made with appropriate medical coverage.
First aid training
The American Medical Association15 in the report on Certificate Trainers in Secondary Schools concluded that: “adequately trained personnel should be present on-site to ensure that such injuries are recognised early, treated immediately, and allowed to heal properly, thereby reducing the risk of more serious injury or reinjury.”
The Football Association (FA), the governing body of football in England, does not have any formal regulations on the minimum appropriate medical qualifications necessary for youth football. They recommend that a club official should have a first aid qualification.16 However, there is no compulsion for youth coaches or club officials to possess any qualification. Indeed the FA Emergency Aid Certificate is limited in that it only deals with life threatening situations, such as bleeding and choking, and resuscitation techniques. It does not include treatment to soft tissue injuries or practical experience of how to deal with minor wounds or medical conditions such as asthma or epilepsy. It is certainly true to say that the FA would encourage everyone concerned with youth soccer to possess a basic first aid qualification, but there is no compulsion from either the FA or County Associations.
Ransone and Dunn-Bennett8 questioned 104 athletic coaches about their first aid knowledge. They found that only 38% of coaches achieved a pass score and that they tended to return an injured player to the game. The low pass rate indicates a lack of training or review among coaches.
A requisite for holding a current first aid qualification is that they have to be periodically reviewed. This process is designed to update skills and to ensure contemporary first aid knowledge and techniques.
In summary, the epidemiological studies seem to indicate that the risk of injury in youth football is low and the injuries that do occur are commonly soft tissue injuries to the lower limb. However, a number of authors and organisations do say that first aid training is important in helping to recognise an injury and in applying appropriate immediate treatment.
This study
Most respondents showed a commitment to working with children, as 75% had been involved with youth football for up to 10 years, with 36% being involved for over five years. This goodwill needs to be recognised and encouraged.
The major aim of this study was to discover the prevalence of appropriate first aid qualifications among youth football officials charged with the responsibility of dealing with injuries. The results indicate that most (61%) do not possess any qualification.
The roles and responsibilities of a first aider include protecting casualties from further harm, administering early and appropriate treatment, and arranging for the care of the player—transfer to hospital or to see a qualified medical practitioner.16 Team officials and club committees have both a legal and moral obligation to ensure that there is a qualified first aider available at every game and training session. This position is supported by Lyznicki et al15 in their paper written on behalf of The American Medical Association.
The FA regulations state that “if at all possible coaches, should attend a recognised first aid course”.17 It is clear that many adults do not satisfy these regulations. Adults who are responsible for children under 18 are deemed to be in loco parentis. They have a duty of care under the law to make every effort to ensure their safety. Although the rate of injury in youth football is low,4–7,9 serious injuries and minor accidents do occur. The legal status of organisers is that they must reasonably foresee risk. Having assessed the risk, strategies must be taken to respond. The provision of appropriate equipment and first aid training is an important component of this response.
The liability if an error were made in assessing and treating an injury or failing to treat an injury would lie with both the first aider and the amateur club that permitted them to undertake this role.
“The amateur club which permits an unqualified member to act as an ad hoc first aid assistant without any practical experience resulting in any serious or actionable injury is as much at risk as the hospital committee allowing an inexperienced practitioner to carry out complex operations usually reserved for the maturer staff.” 18
One solution is for the football authorities both nationally and regionally to instigate a national epidemiological investigation into injury occurrence and current first aid practice in youth football. This will provide the evidence on which to base a cohesive strategy aimed at increasing both the availability and relevance of first aid courses among coaches and club organisers.
Moral case
When an adult adopts the role of a coach or sports organiser, they are morally accountable as well as legally responsible. Having respect for the young player as a person who has basic rights must place the onus on the organiser not to neglect their care. Providing opportunities for competitive football where there is a risk of injury places on the adult a responsibility to prevent injury by adopting safe practice. If an injury does occur, they must seek to provide the best possible care. It is clear that, if reasonable precautions are not taken, such as ensuring the presence of a first aider, they are failing to discharge their moral obligation.
First aid equipment
Few respondents had a facemask in their first aid supplies. Although not a mandatory item, it is recommended for use during rescue breathing.16
The number of teams who had access to a stretcher (14%), crutches (5%), or treatment couch (6%) was small. Acute lower limb injuries should be protected from further trauma by non-weight-bearing techniques such as the use of crutches. However, training in their use should be given. A treatment couch is useful for injury assessment. Portable couches are inexpensive.
Of greater concern is the lack of accessibility to cold water (23%), ice (80%), or ice packs (75%). The use of cryotherapy is fundamental in primary care. Ice can be used for both pain relief and to alleviate swelling through the preclusion of secondary hypoxic injury.19
The number of teams with access to a blanket was low (25%). Provision of a woollen or foil blanket to help maintain body temperature is important, particularly if the player cannot be removed from the field of play.
The FA and Health and Safety Executive should together produce a list of equipment and facilities to which teams should have access at games and training sessions. This checklist would provide a guide for the purchasing of appropriate items to ensure that all teams have adequate supplies to perform basic first aid.
Medical record keeping
Less then half (41%) of teams kept health records for their players. This is of some concern, as recording basic health information helps to identify players with allergies to certain drugs or materials. Players who require medical supervision for asthma, epilepsy, or diabetes can similarly be identified. This type of data should be readily available to medical personnel. Compliance with confidentiality requirements and the data protection act is necessary.
The collection of data on the initial management of an injury can be useful in helping to identify trends in injury occurrence and providing apposite information to medical personnel on treatment. Referral to a doctor or therapist is often some days after the initial injury. Information on the mechanism of injury, signs, symptoms, treatment, and response helps to produce an accurate diagnosis and treatment plan.20
Parental consent for emergency treatment is worth considering, particularly if access to parents in the event of a serious injury may be difficult.
In summary, keeping basic health and injury records together with parental permission for emergency treatment should be standard practice for all teams.
Confidence to treat injuries
Most respondents lacked confidence in the management of asthmatic, epileptic, and diabetic attacks. The initial response must be to assess the player. If the first aider is aware that a player suffers from a medical condition, they are better placed to manage the condition until medical help arrives. Further training in the initial management of these conditions as part of a first aid course would be of benefit.
Injury scenarios
Some of the criteria for returning a player to competitive play include re-establishing strength, balance, coordination, and confidence and assessing whether protective padding or bracing is appropriate.21 Without this information, any decision is based purely on intuition. Most respondents, both qualified and non-qualified, indicated that they would organise their own fitness evaluation for a player returning after injury. A first aider cannot be expected to make this decision. Rehabilitation training is beyond the scope of first aid education.
It is encouraging to note that more correct responses to the injury scenarios were obtained from qualified first aiders than non-qualified (fig 2⇓). However, the low percentage of correct scores is concerning. The “player collapsing” scenario was only answered correctly by just over half of the qualified first aiders. Most (46) replied that their first action would be to check for breathing, and five indicated that they would check the pulse. The advice from the European Resuscitation Council (2000), which is supported by all the major first aid training organisations, is that the initial action should be to determine the player's response.

{kind=link}
{kind=link}
Correct responses to first aid scenarios from qualified and non-qualified first aiders.
The number of incorrect responses to the “player choking” scenario is disturbing. The advice in dealing with a casualty who is choking but breathing is to allow them to continue coughing as they still have a patent airway.16 Most responses from both the qualified and non-qualified indicated that they would perform a finger sweep.
There is no consensus as to the recommended duration or frequency of application for the use of cryotherapy.22 The advice from the Chartered Society of Physiotherapists is that, for ice to be effective, it should be applied for 20–30 minutes every two hours, although there is no specific recommendation.23
Most responses to the “dealing with bleeding” scenario were correct for both the qualified and non-qualified first aiders, indicating that training in this area seems to have been successful.
The initial training of first aiders needs to emphasise that, if a casualty is breathing, performing a finger sweep to remove any obstruction may block the airway. The management of an unconscious casualty needs to be reinforced using the current guidelines.
Conclusion
Despite the moderate response rate, the evidence from this preliminary audit shows that there is a problem of unqualified adults being responsible for providing first aid cover in youth football. There should be a moral and legal obligation on all teams to have a qualified first aider present at all games and training sessions.
The audit portrays a lack of knowledge from both the qualified and non-qualified on how to deal with a player who is choking or unconscious.
Take home message
There is both a moral and legal responsibility on youth team officials to ensure that a qualified first aider is present at all games and training sessions. Keeping accurate records of the players' health and injuries is important.
Training organisations need to reassess and revalidate their training courses and perform follow up evaluations after one and two years to determine if knowledge and skills are retained. A reappraisal every three years would not address this problem.
The FA has an important role in encouraging or indeed obligating every team to have a first aider. Increasing the number of courses, keeping the cost down, and making them available at times to suit would all help to increase the numbers attending.
A sports specific first aid course such as that provided by the National Sports Medicine Institute may be of more relevance then a general Health and Safety Executive or St Johns qualification. The NSMI course includes treatment on the field of play and encompasses practical scenarios that recreate typical sporting situations. Further investigation into the requirements within the European Union and the United States may help to inform the debate in the United Kingdom.
Sports Coach UK should include a specific reference to the desirability of a coach possessing a current recognised sports first aid qualification and first aid knowledge. In addition, attendance of the Sports Coach UK Coach Workshop Injury prevention and management should be encouraged.
REFERENCES
Commentary
This preliminary study highlights the low priority given to the teaching of basic first aid to youth football coaches in England. Although football is the most popular club sport for young people in this country, it is likely that this lack of knowledge extends beyond football to other sports. Recent initiatives in Britain have emphasised the duty of care that all people working with young athletes have in terms of child protection. There needs to be a similar campaign to improve coaches' knowledge of medical care; this should include basic first aid (to a recognised standard), the recognition of serious injury, and some knowledge about conditions likely to be encountered such as asthma, diabetes, and epilepsy. Training in first aid should be a standard requirement for all coaches in youth sport, and should be a condition of funding to a club by the sports governing body or Sport England.
The study also illustrates the need for personnel with first aid knowledge and equipment to be available not only at matches but also at practice sessions. The lack of provision of appropriate medical cover at practice sessions is a problem through all levels of sport including elite adult teams.