Article Text

Abstract
Occupational lung cancers represent a major health burden due to their increasing prevalence and poor long-term outcomes. While wood dust is a confirmed human carcinogen, its association with lung cancer remains unclear due to inconsistent findings in the literature. We aimed to clarify this association using meta-analysis. We performed a search of 10 databases to identify studies published until June 2014. We assessed the lung cancer risk associated with wood dust exposure as the primary outcome and with wood dust-related occupations as a secondary outcome. Random-effects models were used to pool summary risk estimates. 85 publications were included in the meta-analysis. A significantly increased risk for developing lung cancer was observed among studies that directly assessed wood dust exposure (RR 1.21, 95% CI 1.05 to 1.39, n=33) and that assessed wood dust-related occupations (RR 1.15, 95% CI 1.07 to 1.23, n=59). In contrast, a reduced risk for lung cancer was observed among wood dust (RR 0.63, 95% CI 0.39 to 0.99, n=5) and occupation (RR 0.96, 95% CI 0.95 to 0.98, n=1) studies originating in Nordic countries, where softwood dust is the primary exposure. These results were independent of the presence of adjustment for smoking and exposure classification methods. Only minor differences in risk between the histological subtypes were identified. This meta-analysis provides strong evidence for an association between wood dust and lung cancer, which is critically influenced by the geographic region of the study. The reasons for this region-specific effect estimates remain to be clarified, but may suggest a differential effect for hardwood and softwood dusts.
- Meta-analysis < Methodology, speciality
- Wood dust < Materials, exposures and occupational
Statistics from Altmetric.com
Introduction
Occupational lung cancers represent approximately 75% of all occupational cancers1–4 and are a major health burden with relatively poor 5-year survival rates compared with the majority of other cancers.5 ,6 Up to 10–20% of lung cancers have been attributed to occupational exposures1–4 and a synergistic effect has been observed between smoking and many of the occupational exposures.1–4
Occupational exposure to wood dust remains extremely common in a wide range of jobs, despite advances in occupational health and safety policies.7–10 Wood dust was confirmed as a group 1 human carcinogen in 1995 by the International Agency for Research on Cancer (IARC).7 However, wood dust has only been conclusively linked to sinonasal cancers, despite individual studies suggesting an association with a range of respiratory and digestive tract cancers.7 ,8 ,11 Although the nasal cavity/sinuses appear to be the predominate locations for wood dust deposition, wood processing generally produces a wide variety of particle sizes, at least some of which have been shown to be able to deposit in the lungs.12–16 Wood dust has also been confirmed as a respiratory irritant and has been shown to be directly carcinogenic in lung cancer cell lines and to induce lung inflammation in animal models following nasal instillation.17–20 While the evidence for lung deposition and direct cellular toxicity provide a plausible biological mechanism for wood dust-induced lung cancer, the relative frequency of deposition in each location may explain the stronger evidence for sinonasal versus lung cancer.7 ,8 ,14 ,16
While wood dust exposure has been frequently associated with lung cancer, a confirmed association has not been established by the IARC due to heterogeneous results in the literature.7 ,8 A number of factors have been suggested to contribute to this heterogeneity, including the type of wood dust assessed (hardwood vs softwood),7 ,8 confounding by smoking1–4 and misclassification bias related to the method used for determining dust exposure.21–23 While, hardwood dust has been conclusively defined as a human carcinogen, limited evidence exists for softwood dust.7 ,8 However, very few occupational cancer studies have clarified the type of wood dust to which their cohort is exposed making assessment of this variable difficult. Interestingly, the primary wood type varies between countries, and so geographic region may serve as a proxy variable for the type of wood dust assessed in each study.7 ,24 In particular, wood exposure in Nordic countries is primarily to softwood dust, while hardwood dust exposure is relatively more prevalent in many other countries.7 ,24
We performed a systematic review and meta-analysis of the available literature in order to clarify the association between wood dust and lung cancer. We also aimed to assess the influences of geographic region (as a measure of softwood dust exposure), adjustment for smoking and exposure classification methods using subgroup analyses.
Methods
Search strategy
We followed the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines to conduct our review and analysis. A systematic search of the databases CINAHL (from 1982), EMBASE (from 1974), Google Scholar (from ∼1980), JSTOR (from ∼1909), MEDLINE (from 1946), PubMed (from 1946), ScienceDirect (from ∼1856), Web of Science (from 1990) and Wiley Online Library (from ∼1989) through to June 2014 was completed. The search terms used to search all databases were combinations of Wood Dust (‘wood dust’, ‘sawdust’, ‘saw dust’, ‘hardwood dust’, ‘softwood dust’) AND Lung Cancer (‘lung cancer’, ‘lung adenocarcinoma’, ‘lung carcinoma’, ‘lung malignancy’). No additional restrictions were used in the search. A systematic search of the Chinese literature in the database CNKI (from 1915) through to June 2014 was also completed. The English search terms were translated into Chinese as: Wood Dust (‘木屑’, ‘鋸木屑’, ‘軟木屑’, ‘硬木屑’, ‘木塵’, ‘木粉’, ‘木粉塵’, ‘軟木粉塵’, ‘硬木粉塵’, ‘木材性粉塵’) and Lung Cancer (‘肺癌’, ‘肺腺癌’, ‘肺’). The Google Scholar, JSTOR, ScienceDirect and CNKI databases perform full-text searches, and thus allow for the identification of studies without ‘Lung Cancer’ and/or ‘Wood Dust’ in the abstract.
To identify additional articles that assessed wood dust-related occupations and lung cancer risk, we performed an additional PubMed (from 1946) database search using terms for Wood-Related Occupations (occupation, hardwood, softwood, wood, woodworker, carpenter, furniture, cabinet, joiner, mill, sawmill) AND Cancer (cancer, carcinoma, adenocarcinoma). Cancer was used in the search string in order to identify articles where ‘Lung Cancer’ was not specifically listed in the abstract.
References in all identified publications, and in the IARC monographs on wood dust,7 ,8 were also reviewed for additional studies.
Eligibility criteria
This review included cohort and case–control studies looking at the relationship between wood dust and lung cancer. Papers assessing wood dust directly were chosen as the primary outcome, while studies that assessed wood dust-related occupations were included as a secondary outcome. We included all studies into the meta-analysis that met the following criteria:
Contained an estimate of relative risk for lung cancer or data allowing such estimates to be calculated.
Contained a risk estimate related to a dichotomous index of exposure (ever vs never) or data allowing such estimates to be calculated.
Contained an explicit analysis of wood dust as an exposure category at an individual not occupational level
OR
Contained an analysis of a wood dust-related occupation (ie, woodworkers, carpenters and furniture/cabinet makers).
Were published in English or Chinese.
Study selection
All articles identified in the database searches were initially screened for eligibility based on their titles and abstracts, followed by a full-text review of eligible articles. All English language articles were independently screened by two authors (DGH and MEL). Chinese language articles were initially screened for eligibility based on their titles and abstracts by a single author (KLC), while all full-text reviews were discussed by two authors (DGH and KLC). Disagreements between reviewers were resolved by consensus among all authors (DGH, MEL and KLC).
Data extraction
Data was extracted manually by one author for both the English (DGH) and Chinese (KLC) literature, and was subsequently reviewed by another author (MEL/DGH). Risk estimates for total lung cancer were extracted for the primary analysis, but risk estimates for histological subtypes were also extracted for subanalysis. When multiple methods for defining wood dust exposure were used in a single paper (ie, job-exposure matrix and self-reported), the risk estimate using the exposure classification method presented as the ‘gold standard’ by the authors of the paper was used. When males and females were analysed separately, the risk estimates for males were included as males represent the majority of those exposed to wood dust.
Publications presenting data on the same cohort of patients were identified by comparing the author lists and study locations. The most recent paper from each cohort was chosen unless a previous paper had a larger cohort size or presented a risk estimate adjusted for more confounding variables. In addition, when a study analysed a subset of the larger population in a cohort, we included the study that used the entire population, even if this was not the most recent study (eg, the full cohort vs the non-smoking subset of the full cohort). The choice of study publication was confirmed by consensus.
Information from each paper was extracted on (1) study design, (2) country of study, (3) sample size, (4) wood dust exposure measure/occupation (5) and measures of effect including 95% CIs and adjusting/matching variables. Byar’s approximation was used to recalculate missing 95% CIs for cohort studies, while crude ORs were computed for case–control studies without summary effect measures. For data sets in which no events were observed in one of the groups, 0.5 was added to all observations.25
Risk of bias in individual studies
The risk of bias in each study was determined using the Newcastle-Ottawa Scale, which assesses participant selection, comparability and outcome/exposure assessment to a maximum of nine stars.26 We rated studies as having low bias (7–9 stars), medium bias (5–6 stars) and high bias (0–4 stars). The risk of bias was determined by two independent authors for English (MEL/DGH) and Chinese (KLC/DGH) publications. Discrepancies in score (generally no more than 1 point) were resolved via consensus.
Statistical analysis
All statistical analyses were performed using the Metafor package in R.27 For each meta-analysis, a random-effects model was specified using the restricted maximum-likelihood estimator method.27 Random-effects models were chosen due to the significant heterogeneity in most analyses. For the purposes of pooling risk estimates, ORs were assumed to approximate the true risk ratio, since the baseline risks for lung cancer are generally low.28 The primary meta-analysis was performed on all case–control and cohort studies assessing wood dust exposure and lung cancer (not separated into histological subtypes). A priori subgroup analyses were performed based on the geographic region of the study (studies originating outside and inside the Nordic countries (Denmark, Finland, Iceland, Norway, Sweden) as a measure of softwood dust exposure, the method for determining wood dust exposure (job-exposure matrix, self-reported or combination methods) and the use of adjustment for smoking. The Nordic countries were specifically chosen as a proxy variable of softwood dust exposure due to the predominant softwood dust exposure in these countries.7 ,24 ,29–31 Subanalyses were also performed on all studies that assessed histological subtypes of lung cancer (adenocarcinoma, squamous cell carcinoma, small-cell lung carcinoma or other) and on studies that assessed lung cancer risk among wood dust-related occupations (ie, woodworkers, furniture makers, carpenters). Studies directly assessing wood dust exposure and those assessing wood dust-related occupations were analysed separately due to the inherent differences/limitations unique to each study design (ie, different misclassification errors, heterogeneity between occupation definitions and occupation-specific confounders).
The potential for publication bias was determined by assessing funnel plot asymmetry using the Egger regression test.27 Asymmetry in a funnel plot (the effect estimates vs their SEs) tests for small study effects (with large SEs), which may suggest publication bias. However, asymmetry can also be due to true biological heterogeneity.32 Heterogeneity between studies was assessed using the I2 statistic. Following the Cochrane handbook (http://www.cochrane-handbook.org), I2 values were interpreted as showing moderate (30–60%), substantial (50–90%) and considerable (75–100%) heterogeneity.25
Results
Study characteristics
Figure 1 details our study selection process. A total of 85 articles were included in the final meta-analysis.5 ,30 ,33–115 The included studies are detailed in online supplementary table S1. An additional 56 articles that met the inclusion criteria were identified (see online supplementary table S2), but not used in the meta-analysis as they represented publications on an overlapping cohort of patients, duplicate publications or publications missing information necessary for the meta-analysis. Five additional studies were excluded for presenting data that could not be dichotomised into ever versus never exposure.116–120 Forty studies5 ,30 ,34–36 ,38 ,40 ,42–44 ,50–54 ,60 ,62 ,64 ,65 ,67 ,69 ,70 ,73–76 ,86 ,90 ,91 ,93 ,96 ,97 ,99 ,100 ,102 ,105 ,106 ,110 ,113 ,115 were rated as having a low risk of bias using the Newcastle-Ottawa Scale (see online supplementary table S1).

Flow chart of study selection strategy. *Other sources include the International Agency for Research on Cancer (IARC) monographs and the reference lists of relevant publications. Potentially relevant studies were not counted if they were identified using the database search.
Primary meta-analysis on lung cancer and wood dust exposure
Twenty-four case–control, five nested case–control and nine cohort studies assessing the association between wood dust and lung cancer were included in the primary meta-analysis (figure 2). The studies originated from Belgium,55 Canada,42 ,69 ,99 ,109 Chile,59 China,48 ,67 ,79 ,106 ,111 ,113 ,114 England,84 Finland,30 ,74 Holland,76 India,63 Iran,68 Norway,75 Pakistan,81 Poland,105 Russia,34 Sweden,72 ,86 Uruguay52 and the USA.35 ,36 ,38–40 ,73 ,78 ,88 ,102 ,110 Overall, a significantly increased risk for developing lung cancer following wood dust exposure was observed (RR 1.25, 95% CI 1.11 to 1.41, n=38), with ‘considerable’ heterogeneity between studies (I2=82.1%, p<0.01; figure 2).

Forest plot of all studies assessing wood dust and lung cancer incidence.
Subgroup analysis by geographic region of study
Owing to the well-described predominant softwood exposure in the Nordic countries,7 ,24 the geographic region of each study was used as a measure of the type of wood dust to which that cohort was exposed. In the subgroup analysis of studies originating outside of the Nordic countries (mixed hardwood and softwood dust), there was a significantly increased risk for developing lung cancer associated with wood dust exposure (RR 1.34, 95% CI 1.19 to 1.50, n=33), with ‘moderate’ heterogeneity (I2=39.4%, p=0.07; figure 3). In contrast, among studies originating in the Nordic countries (predominantly softwood dust exposure), there was a significantly reduced risk for developing lung cancer (RR 0.63, 95% CI 0.39 to 0.99, n=5), with ‘moderate-substantial’ heterogeneity (I2=55.6%, p=0.05; figure 3).

Forest plot all studies assessing wood dust and lung cancer incidence, subdivided based on the geographic region of study origin.
Subgroup analysis of smoking-adjusted studies
Twenty-three of the wood dust studies controlled for smoking (see online supplementary table S1). The overall association between wood dust and lung cancer incidence was maintained among all studies that controlled for smoking (RR 1.31, 95% CI 1.10 to 1.56, n=23). The significantly increased risk for lung cancer was also maintained among studies originating outside the Nordic countries (mixed hardwood and softwood dust) that controlled for smoking (RR 1.48, 95% CI 1.29 to 1.69, n=19, I2=0.0%). However, the reduced risk for lung cancer was no longer significant among studies originating within the Nordic countries (predominantly softwood dust exposure) that controlled for smoking (RR 0.64, 95% CI 0.40 to 1.01, n=4, I2=62.2%).
Subgroup analysis on method for classifying wood dust exposure
Nineteen of the studies used self-reported exposure, 15 studies used a job-exposure matrix, and four studies used a combination of methods to determine wood dust exposure (see online supplementary table S1). Across all studies, a significantly increased risk for lung cancer incidence following wood dust exposure was identified in studies using self-reported exposure (RR 1.29, 95% CI 1.15 to 1.45, n=19, I2=23.5%) or combination methods (RR 1.47, 95% CI 1.11 to 1.96, n=4, I2=50.5), but this association failed to reach significance among those studies using a job-exposure matrix (RR 1.18, 95% CI 0.93 to 1.48, n=15, I2=92.1%). However, a greater proportion of the studies that used a job-exposure matrix did not control for smoking and/or originated in the Nordic countries (where softwood dust is the predominate exposure). When this subgroup analysis was repeated in a post hoc analysis restricted to studies originating outside of the Nordic countries (mixed hardwood and softwood dust exposure) that also controlled for smoking, a significantly increased risk was observed among studies using the self-reported (RR 1.33, 95% CI 1.16 to 1.51, n=12, I2=20.0%), job-exposure matrix (RR 1.76, 95% CI 1.29 to 2.42, n=5, I2=28.9%) and/or combination (RR 2.09, 95% CI 1.01 to 4.34, n=2, I2=61.3%) methods.
Subanalysis of lung cancer histological subtypes
Ten studies assessed the effect of wood dust exposure on various histological subtypes of lung cancer (see online supplementary table S1). A significantly elevated risk for developing all of the histological subtypes of lung cancer was observed following wood dust exposure (figure 4). The elevated risk ratios were highest for squamous cell carcinomas (RR 1.54, 95% CI 1.24 to 1.92, n=4), followed by those for adenocarcinomas (RR 1.32, 95% CI 1.08 to 1.60, n=7) and small-cell lung carcinomas (RR 1.32, 95% CI 1.05 to 1.66, n=7). Similar trends were observed when the analysis was restricted to studies that controlled for smoking.

Forest plot of all studies assessing wood dust and histological subtypes of lung cancer, subdivided based on histological subtype. SCLC, small-cell lung carcinoma; LCLC, large-cell lung carcinoma.
Subanalysis on lung cancer and wood dust-related occupations
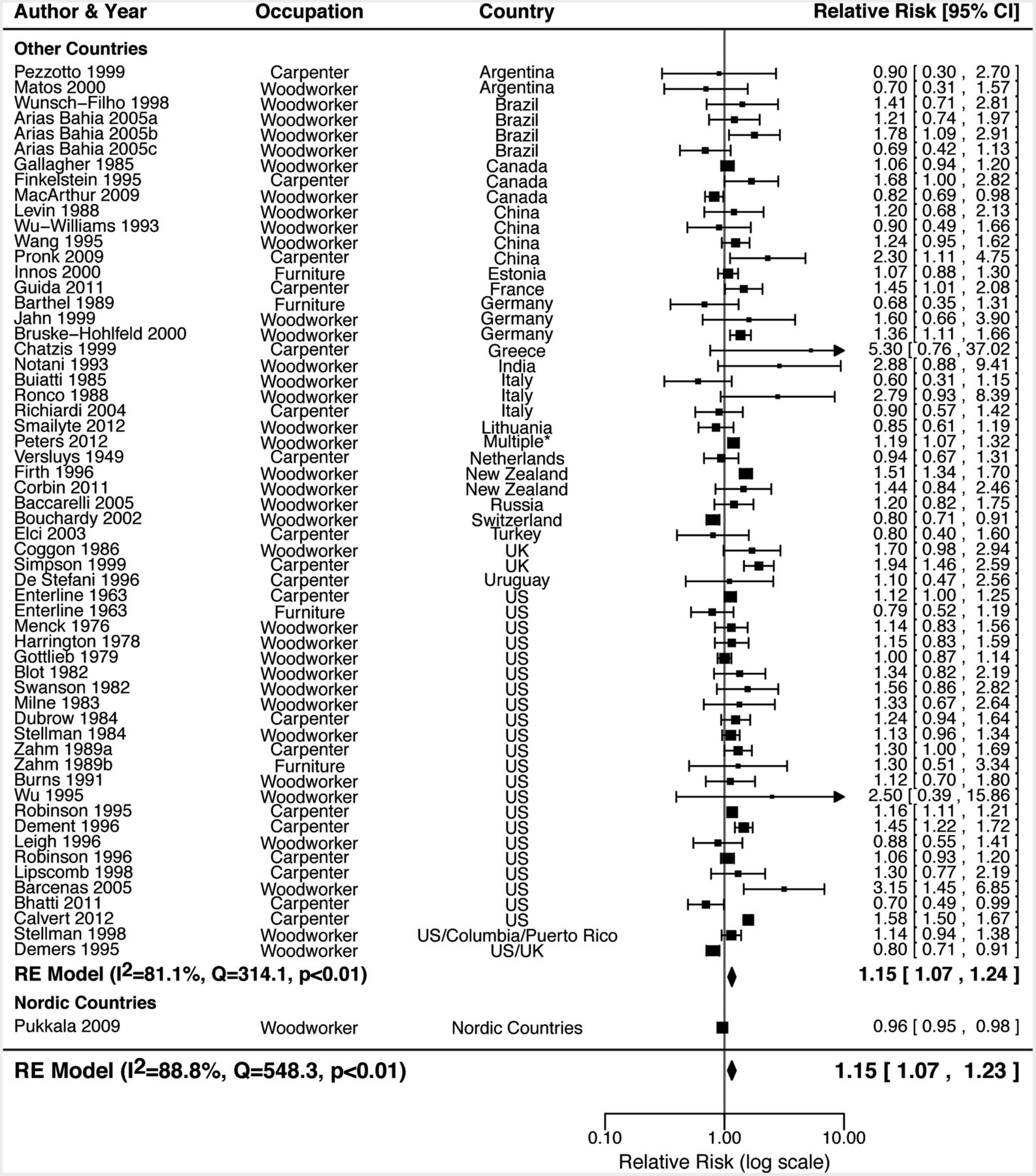
Fifty-nine studies assessed the association between wood dust-related occupations and lung cancer risk (see online supplementary table S1). Consistent with the wood dust meta-analysis, a significantly increased risk for lung cancer was observed across all studies (RR 1.15, 95% CI 1.07 to 1.23, n=59), with ‘considerable’ heterogeneity between studies (I2=88.8%, p<0.01; figure 5). This association remained significant when the multiple subcohorts from a single paper were removed (RR=1.15).33 ,58 ,115 This association was also not dependent on a single occupational group and remained significant when studies assessing ‘furniture makers’ (RR=1.16, n=55) or ‘carpenters’ (RR=1.09, n=40) were removed in a post hoc analysis. Finally, this association was also not dependent on the study type, as the association remained significant when case–control (RR 1.17, n=34) and cohort (RR 1.12, n=26) studies were analysed separately.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Forest plot all studies assessing wood dust-related occupations and lung cancer incidence, subdivided based on the geographic region of study origin.
A significantly increased risk for lung cancer (RR 1.15, 95% CI 1.07 to 1.24, n=58) was observed among the studies originating outside the Nordic countries, while a significantly reduced risk for lung cancer (RR 0.96, 95% CI 0.95 to 0.98) was observed in the one included study5 that originated in the Nordic countries (predominantly softwood dust exposure; figure 5).
Publication bias
No evidence for publication bias was observed on visual inspection of funnel plot asymmetry across all wood dust studies (see online supplementary figure S1A) and there was no evidence using Egger’s test for small study bias (p=0.456). There was some suggestion of funnel plot asymmetry across the wood dust-related occupational studies (see online supplementary figure S1B), although this failed to reach significance using Egger’s test for small study bias (p=0.080).
Discussion
Occupational exposure to wood dust was confirmed to be carcinogenic to humans (group 1) by the IARC in 1994, but the evidence as a risk factor for lung cancer has been inconsistent.7 The recent IARC monograph Volume 100C also failed to confirm an association between lung cancer and wood dust due to the heterogeneous findings in the literature.8 ,11 Our robust literature search and meta-analysis showed a significantly elevated risk for developing lung cancer following wood dust exposure when pooling all studies (figure 2). We also observed this significantly elevated risk in studies that assessed lung cancer risk among wood dust-related occupations, and not wood dust exposure per se (figure 5). Importantly, evidence for wood dust deposition in the lungs and its in vitro carcinogenicity provide a biological mechanism to support the observed elevated risk for lung cancer.7 ,8 ,14 ,16 The results of this meta-analysis were maintained when studies that had not controlled for smoking were excluded. Smoking is the strongest risk factor for lung cancer, and confounding due to cigarette smoking often limits the accurate assessment of the effects of other lung carcinogens.1 ,4
We had initially hypothesised that studies originating from the Nordic countries would show a proportionally lower risk for lung cancer due to the predominant softwood dust exposure in these countries7 ,24 ,29–31 and the limited evidence supporting the carcinogenicity of softwood dust.7 ,8 In support of this hypothesis, we observed a significantly elevated risk for developing lung cancer among studies originating outside of the Nordic countries and a significantly decreased risk among studies originating from the Nordic countries (figures 3 and 5). Furthermore, the only two wood dust studies in this meta-analysis that specified the type of dust to which their cohort was exposed independently concluded that their identification of a decreased risk was due to the predominant softwood dust exposure in their cohorts.30 ,38 However, one of these studies originated in the USA38 indicating that wood dust type rather than region is the likely cause of the differential risk effects of hardwood and softwood dusts on lung cancer. Consistent with these findings, all studies assessing wood dust-related occupations that described predominant exposure to softwood dust also showed a decreased or non-significant risk for lung cancer, independent of their origin in the Nordic countries.5 ,38 ,96 ,101
While we used the geographic region of the study population as a measure for the type of wood dust exposure, there are a number of other potential explanations that may contribute to the region-specific trends observed in this meta-analysis. This includes unidentified confounders,2 ,3 ,31 genetics7 ,8 ,121 ,122 and/or differences in occupational health and safety standards between countries.2 ,5 ,123–126 A potential confounder for the decreased risk for lung cancer with wood dust exposure is bacterial endotoxins, arising from bacterial colonisation of either stored wood or loose wood dust.31 ,38 ,127 Bacterial endotoxin is thought to protect against lung cancer,127 and thus increased exposure to this bacterial contamination among wood workers compared with the general population may help explain the reduced risk estimates for lung cancer in the Nordic countries.31 ,38 The contrasting risk estimates may also be due to region-specific differences in genetics, environment or health policies, which might reduce the size of any increased risk. Nordic countries are generally thought to be world leaders in occupational health and safety practice, especially at the time when majority of these studies were conducted.5 ,123 ,124 The lack of any increased risk among the Nordic countries may therefore be due to differences in the wood dust-exposed workers, such as exposure to relatively lower levels of wood dust or other harmful exposures as a result of better occupational health and safety practice.2 ,125 ,126
One of the most commonly cited limitations of the observational studies on wood dust exposure is the potential for measurement bias in the exposure assessment.22 ,76 Self-reported exposure strategies are generally susceptible to recall bias, while job-exposure matrix strategies can be susceptible to variations in true exposure under a given job title.22 ,76 However, an increased risk for lung cancer was observed across all methods of determining wood dust exposure, especially after controlling for geographic region and smoking. This finding was supported by three studies that directly compared the exposure methods and showed no significant differences between methods.36 ,55 ,76
We also assessed the association between wood dust exposure and the different histological subtypes of lung cancer (figure 4). We observed significantly increased risk estimates for all histological subtypes of lung cancer, with the highest risk for squamous cell carcinomas (although CIs largely overlapped). This appears to contradict data on sinonasal cancers, where adenocarcinomas have been most frequently observed among woodworkers,7 ,8 although some studies have identified squamous cell carcinomas more commonly.30 ,128 Overall, these data suggest that wood dust increases the risk for all subtypes of lung cancer, and not only a specific subtype.
To the best of our knowledge, this is the first systematic review or meta-analysis assessing wood dust and lung cancer risk, outside of the IARC publications.7 ,8 We performed a robust search of the English and Chinese literature and identified a large number of studies not included in the IARC publications. Our analysis also included a large number of studies where wood dust and lung cancer was not the primary outcome of the paper, thereby reducing the likelihood of publication bias of positive results, which was supported by our assessment of funnel plot asymmetry. However, it is also possible that studies assessing a large number of exposures would provide a less accurate assessment of true wood dust exposure, although we found no evidence to support this hypothesis.
In the current meta-analysis, we chose to primarily focus on studies that specifically assessed wood dust exposure in order to provide the most direct assessment of the relationship between wood dust exposure and lung cancer risk. We also aimed to avoid some of the inherent challenges/limitations of assessing purely occupation-based studies, including the heterogeneity in occupational classifications and the greater risk for individual occupation-specific factors obscuring any wood dust-specific effects.25 ,103 ,129 ,130 Consistent with this, some of the studies showed a large degree of variation in the individual risk estimates when multiple different wood dust-related occupations analysed within the same paper (not shown).45 ,103 However, the observation of a significantly elevated risk for lung cancer (of similar magnitude) among these occupation-based studies (figure 5) adds further weight to the association between wood dust and lung cancer, and also suggests that our focus on wood dust-specific studies did not bias the results of this meta-analysis.
There are a number of potential limitations to our meta-analysis. First, we were unable to perform any analyses to assess the dose–response relationship between wood dust and lung cancer or to determine any effects related to duration of exposure. These factors were generally not assessed or assessed using a variety of approaches making a quantitative synthesis unfeasible. Second, the included studies varied greatly in their study design/population characteristics and accounting for all these factors in our meta-analysis was not feasible. Finally, unknown confounding exposures might still explain our findings. Asbestos, silica, formaldehyde, solvents and exhausts are all associated with wood dust-related professions and have been independently linked with lung cancer.3 ,7 ,8 However, the studies included in this meta-analysis analysed wood dust exposure from a diverse range of occupational contexts, thereby limiting the possibility that a single confounding exposure accounted for the observed associations.
In conclusion, this meta-analysis has demonstrated significant associations between lung cancer and wood dust exposure or employment in wood dust-related occupations, with an increased risk among studies that originated outside of the Nordic countries (mixed hardwood and softwood dust exposure). The reduced risk for lung cancer observed following wood dust exposure in Nordic countries may be due to the predominant softwood dust exposure in these countries. Larger studies designed to explore the causes of these differing associations are needed.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
- Data supplement 1 - Online figure
- Data supplement 2 - Online tables
Footnotes
Contributors DGH was involved in study design and supervision, analysis and interpretation of data, statistical analysis, and drafting of the manuscript. MEL and KLC were involved in analysis and interpretation of data, and critical revision of the manuscript. RJW was involved in statistical analysis and critical revision of the manuscript. EMS was involved in drafting of the manuscript and critical revision of the manuscript.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.