Article Text

Abstract
Introduction Some studies have suggested increased lung cancer risks among bakers, however the results overall were inconsistent. The authors studied lung cancer risks among bakers and baking-related occupations in the SYNERGY pooled case–control database from 16 countries.
Methods Occupation in a baking-related job was identified from the subjects’ job histories. ORs adjusted for log(age), study centre, smoking behaviour and ever employment in a job with known exposure to occupational lung carcinogens were calculated by unconditional logistic regression. Findings were stratified by sex, histological subtype of lung cancer and smoking status.
Results 19 366 cases (15 606 men) and 23 670 control subjects (18 528 men) were included. 473 cases (415 men, 58 women) and 501 controls (437 men, 64 women) had ever worked in baking or a related job. We did not observe an increased risk for men in baking (OR 1.01; 95% CI 0.86 to 1.18). No linear trends were observed for duration of employment. Some results suggested increased lung cancer risks for women, for example, for working as a baker for >30 years and in never-smokers, but after exclusion of one study these increased risks disappeared.
Discussion The findings from this study do not suggest increased lung cancer risks in baking-related professions.
Statistics from Altmetric.com
What this paper adds
-
Increased lung cancer risks for bakers and workers in baking-related professions have been suggested in previous studies, but results were inconsistent.
-
Study of lung cancer risks has been impaired by a low prevalence of bakers in previous population-based studies or by insufficient smoking information in retrospective cohorts.
-
SYNERGY is one of the largest international collaborations on occupational lung cancer with detailed smoking information.
-
We calculated detailed analyses stratified by smoking status, histological subtype and several aspects of being employed as a baker.
-
Results demonstrate that bakers are not at increased risk for lung cancer.
Introduction
It has been estimated that 10% of lung cancer cases are attributable to occupational lung carcinogens worldwide, but attributable fractions vary between regions and studies.1
Previous studies have reported excess lung cancer risks among bakers, pastry cooks and confectionary makers based on job titles in large cohorts2 or case–control studies.3 ,4 However, the published evidence is inconsistent with respect to sex-specific risks or the definition of baker as a job title.4 ,5 In addition, the interpretation of these studies has been hampered by possible sources of bias, including inability to control for smoking behaviour and/or simultaneous exposure to other occupational lung carcinogens.
We studied the association between lung cancer risk and occupation as a baker, pastry cook, chocolate, macaroni or confectionary maker. Due to the study size we were able to conduct in-depth analyses by histological subtype of lung cancer, smoking status and different baking jobs.
Methods
The detailed study methods have been described elsewhere.6 ,7 Briefly, SYNERGY (‘Pooled Analysis of Case-Control Studies on the Joint Effects of Occupational Carcinogens in the Development of Lung Cancer’) has been developed as an international collaboration for research into occupational lung cancer. Currently, 16 case–control studies from 22 study centres are included in this database.
The majority of included studies used population-based controls (81.6%), while the remaining control subjects were obtained from hospitals. A total of 19 366 cases (15 606 men, 3760 women) and 23 670 control subjects (18 528 men, 5142 women) are included in this database. More information about SYNERGY is available on the study's website at http://synergy.iarc.fr.
To assess occupational exposure, five-digit ISCO (International Standard Classification of Occupations, revision 1968) codes from the subjects’ job histories indicating a baking-related job (codes 7-76.00 to 7-76.90) held for at least 1 year were used (referred to as ‘baking’). Duration of exposure was estimated using the cumulative period of being employed in baking. Missing values were observed if, for example, the start or end year was lacking in the job history.
We estimated ORs and associated 95% CIs using unconditional logistic regression. Analyses were stratified by sex and major histological subtype of lung cancer. Analyses were adjusted for study centre, log-transformed age, smoking as log(cigarette pack-years+1), time-since-quitting smoking (2–7, 8–15, 16–25, 26+ years before interview/diagnosis, never) and other tobacco smoking habits, and employment in occupations with an established lung cancer risk (‘list A’ job, yes/no).8 Participants who had never worked as a baker or in baking-related occupations comprised the reference group.
We conducted several sensitivity analyses to assess the robustness of our results. To explore effect modification in risk estimates, we performed analyses stratified by smoking status (never, former, current smokers) and calendar period of exposure (jobs starting before and after 1960).
We used random-effect meta-regression models to pool the ORs of individual studies. Between-study heterogeneity was determined using I2 statistics. Meta-analyses were performed using Comprehensive Meta-Analysis V.2.2.027 software (Biostat, Englewood, New Jersey, USA). All other calculations were carried out with SAS V.9.2 (SAS Institute, Cary, North Carolina, USA).
Results
A total of 974 bakers and pastry cooks, and chocolate, macaroni and confectionary makers (852 men, 122 women) were identified from the SYNERGY epidemiological database.
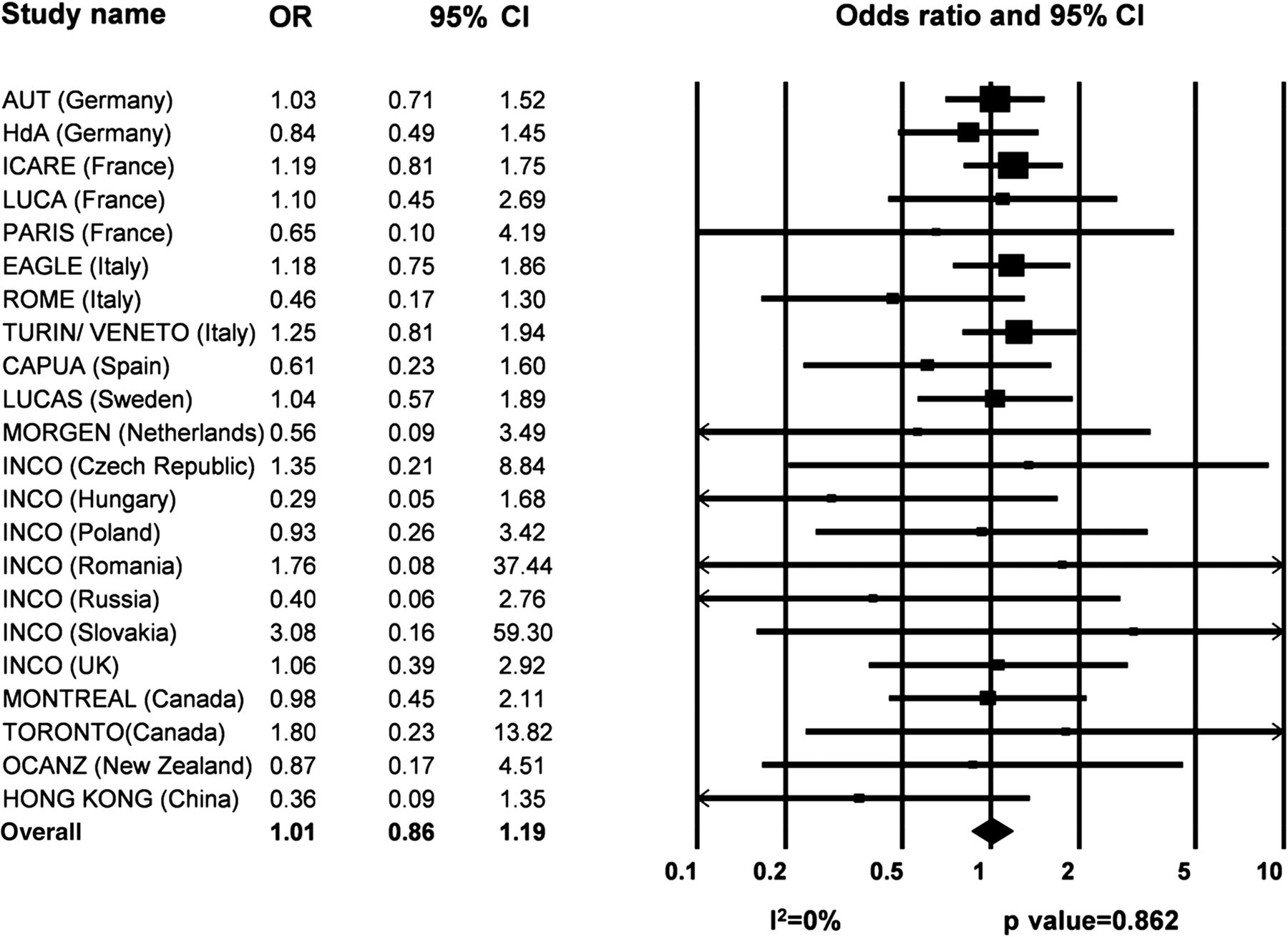
In men, the meta-analysis for ever having worked in baking did not show heterogeneity between studies (I2=0%, p=0.86) with most risk estimates either not elevated or below unity (figure 1). In women, only the Italian EAGLE study showed a statistically significant increased risk (OR 4.29; 95% CI 1.38 to 13.31) (not shown).

{kind=link}
Forest plot of meta-analysis for men having ever worked in baking by study centre.
In men, work in baking and related occupations was not associated with an increased risk of lung cancer. Ever employment as a baker or in a baking-related job did not result in an increased risk for total lung cancer, adenocarcinoma, squamous cell carcinoma or small cell carcinoma. Adjustment for smoking slightly weakened the observed associations (not shown). Stratification by smoking status did not yield increased risks (table 1).
Analyses of lung cancer risk in men according to smoking status of bakers, pastry cooks, and macaroni and confectionary makers for total lung cancer and histological subtype*
Analyses according to type of baking activity (five-digit ISCO code) had small numbers and imprecise risk estimates with wide CIs. None of the ORs were markedly raised (see online supplementary table S1).
We did not observe a consistent upward trend in lung cancer risk with longer employment in baking among men (see online supplementary table S2). Likewise, our analyses did not show a consistent downward trend with increasing time since first or last employment. However, the majority of participants had stopped working in baking more than 25 years before the interview (81% of men and 75% of women in baking or a related job) (no results shown).
In contrast, increased risks were suggested for women in some analyses (see online supplementary tables S1 and S2). For example, never-smoking women showed increased risks for ever working in baking with an OR of 1.87 (95% CI 1.02 to 3.42) (not shown). However, all of the reported risk increases in women were largely dependent on the Italian EAGLE study. After exclusion of this study, risks were no longer elevated (results not shown).
When we individually dropped other studies from the analyses, results remained unchanged. Sensitivity analyses restricting the analyses to personal interviews or studies with population controls did not change results. We did not observe differences in period-specific risk estimates (for subjects starting their jobs before or after 1960) (not shown).
Discussion
In this study we did not identify elevated risks for lung cancer in association with baking-related occupations. Some analyses in women suggested elevated risks, but these results depended on a single study. When we excluded this study, there was little evidence of an increased risk.
The strengths of this study include the large sample size of more than 19 000 cases and 23 000 controls, including large numbers of never-smoking cases and women. Smoking information was nearly complete with less than 1% having missing values, making SYNERGY the largest epidemiological database for occupational lung cancer with detailed smoking information to date.7 We were able to adjust for detailed smoking behaviour and to stratify analyses according to the major histological subtypes of lung cancer. Adjustment for smoking had an effect, generally in the direction of slightly weakening the observed associations.
Limitations include the fact that due to the community-based design of the included studies, the prevalence of baking-related jobs was low (2.4% among cases and 2.1% among controls). Despite high numbers, the fraction of never-smoking cases was small, which limited our ability to further stratify analyses by sex, histological subtype or detailed baking job. Further weaknesses include the fact that analyses could only be based on job titles from the participants’ work histories. General limitations are the low response rate in several participating studies, the possibility of exposure misclassification due to the variable quality of self-reported occupational histories, misclassification of histo-pathological tumour type, and the use of proxy information in some studies.
A common reason for bakers to leave their jobs early in their career is baker's asthma.9 This may result in the selection of healthier bakers (ie, a strong healthy worker effect) with less susceptibility to other respiratory diseases. Indeed, only a minority of participants reported a job in baking as the longest in their occupational history (28% of male and 35% of female bakers, with a median duration of 33.5 years in men (IQR 25–42 years) and 10 years (IQR 6–25 years) in women). However, lung cancer risks for participants who worked for only a short time as bakers were not higher in comparison with participants whose primary job was related to baking. An analysis in a subset of the SYNERGY studies (eight centres which collected information on a diagnosis of asthma) did not reveal evidence for a healthy worker effect either: 8.7% of male bakers (50 participants) had been diagnosed with asthma during their lifetime, while 6% of men in other jobs had asthma (results not shown). Nevertheless, as the reasons why participants left their baking jobs were not ascertained in our study, we cannot rule out the possibility of bias due to a healthy worker effect.
The published evidence on the association between a job in baking and lung cancer risk is sparse. The NOCCA study from the Nordic countries, which covered over 15 million subjects, revealed increased standardised incidence ratios for food and beverage workers in both sexes. However, this record-linkage study neither controlled for smoking behaviour nor evaluated bakers and pastry cooks as separate occupational groups.10 Other job title-based epidemiological studies that were able to control for smoking have reported excess risks for bakers, pastry cooks and confectionary makers.2–4 ,11 Nevertheless, the evidence from these studies is inconsistent. For example, one Italian study observed a fivefold risk increase for male general bakers and a 60% elevated risk for male pastry cooks and confectionary makers, which was not seen among female bakers and pastry cooks.4 In contrast, Finnish data showed an increased lung cancer risk only among female bakers (SIR 1.38; 95% CI 1.01 to 3.85).5
In SYNERGY, the majority of studies did not indicate increased lung cancer risks for work in baking. Only in one centre from a similar Northern Italian region as the previous Italian case–control study,4 were increased lung cancer risks for ever working in baking observed. However, in contrast to this other Italian study, risk increases in SYNERGY were only demonstrated for women.
A small case series from Italy described an increased risk for pleural mesothelioma among bakers who had used asbestos-insulated ovens. In Italy asbestos was banned in the early 1990s, however, field investigations revealed that in the mid-1990s asbestos-containing ovens were still in use.12 Because asbestos is a known lung carcinogen, exposure to this agent may have also been responsible for the observation of an increased risk in the EAGLE study. However, because risk increases were restricted to women, it is more likely that the positive results in this study represent a chance finding rather than a true risk elevation.
Squamous and small cell carcinoma are more frequently observed in subjects with increasing exposure to tobacco smoke.6 Few of the published studies on the association between baking and lung cancer so far were able to calculate risk estimates stratified by histological subtype, generally showing higher risks for squamous and small cell carcinoma.13 ,14 In our analyses we did not identify consistent differences in risk according to histological subtype.
Flour dust and moulds in grains and dust have been suggested as possible carcinogenic agents in bakeries.5 ,11 In addition, bakers can be exposed to fumes from the baking process, which includes heating of ovens and baking of food. These fumes may contain particulates and carcinogenic compounds, including polycyclic aromatic hydrocarbons, although the detailed content of carcinogens is still unknown,15 and heating processes may vary considerably by type of oven (electricity, gas, wood stoves, etc) and country. However, as details regarding baking practices were not solicited in SYNERGY, any assumption of exposure to possible carcinogens during the baking process is speculative.
In summary, in our large international collaborative study of occupational lung cancer which included complete occupational histories and detailed information on smoking behaviour, we did not observe increased risks in participants who were working as a baker or in a baking-related job. Our findings which suggested an increased risk among women in baking were dependent on a single study from Northern Italy, which likely represents a chance finding.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Files in this Data Supplement:
- Data supplement 1 - Online table 1
- Data supplement 2 - Online table 2
Footnotes
-
Contributors TB, BK and BP interpreted the data and supported drafting of the manuscript. TT and BK were responsible for the statistical analysis. TBr, KS, HK, RV, PB and AO conceived the design of the pooled analysis. All other authors were responsible for conception, design and data acquisition of the studies in their respective country. All authors contributed to the revision of the manuscript and approved the final version.
-
Funding This study was supported by the German Social Accident Insurance, grant FP 271. Grant sponsors of the individual studies were the Canadian Institutes of Health Research and Guzzo-SRC Chair in Environment and Cancer, the Fondation de France, the German Federal Ministry of Education, Science, Research, and Technology and the Ministry of Labour and Social Affairs, the EC's INCO-COPERNICUS Program, the Polish State Committee for Science Research, the Roy Castle Foundation, the NIH/NCI/DCEG Intramural Research Program, Lombardy Region, INAIL and the European Union Nuclear Fission Safety Program, the Italian Association for Cancer Research, Region Piedmont, the Compagnia di San Paolo, the Europe Against Cancer Program, the Swedish Council for Work Life Research and the Swedish EPA, the University of Oviedo, the European Regional Development Fund and the State Budget of the Czech Republic (RECAMO, CZ.1.05/2.1.00/03.0101), CIBERESP and FISS-PI060604.
-
Competing interests The authors declare no conflicts of interest. TB, BK, TT, BP and TBr, as staff of the Institute for Prevention and Occupational Medicine (IPA), are employed at the ‘Berufsgenossenschaft Rohstoffe und chemische Industrie’ (BG RCI), a public body which is a member of the study's main sponsor, the German Social Accident Insurance. IPA is an independent research institute of the Ruhr-Universität Bochum. The authors are independent of the German Social Accident Insurance regarding study design, access to the collected data, responsibility for data analysis and interpretation, and the right to publish. The views expressed in this paper are those of the authors and not necessarily those of the sponsor.
-
Ethics approval The national ethics committees for each study and the IARC Institutional Review Board for the pooled analysis approved this study.
-
Provenance and peer review Not commissioned; externally peer reviewed.