Article Text

Abstract
Objective This study characterises neurocognitive domains that are affected by movement-induced time-varying magnetic fields (TVMF) within a static magnetic stray field (SMF) of a 7 Tesla (T) MRI scanner.
Methods Using a double-blind randomised crossover design, 31 healthy volunteers were tested in a sham (0 T), low (0.5 T) and high (1.0 T) SMF exposure condition. Standardised head movements were made before every neurocognitive task to induce TVMF.
Results Of the six tested neurocognitive domains, we demonstrated that attention and concentration were negatively affected when exposed to TVMF within an SMF (varying from 5.0% to 21.1% per Tesla exposure, p<0.05), particular in situations were high working memory performance was required. In addition, visuospatial orientation was affected after exposure (46.7% per Tesla exposure, p=0.05).
Conclusion Neurocognitive functioning is modulated when exposed to movement-induced TVMF within an SMF of a 7 T MRI scanner. Domains that were affected include attention/concentration and visuospatial orientation. Further studies are needed to better understand the mechanisms and possible practical safety and health implications of these acute neurocognitive effects.
- MRI
- static magnetic fields
- static magnetic stray fields
- time-varying magnetic fields
- cognition
- exposure
- risk assessment
- electromagnetic fields
- occupational health practice
- exposure assessment
- statistics
- hygiene/occupational hygiene
- epidemiology
- retrospective exposure assessment
- neurobehavioural effects
- longitudinal studies
- exposure monitoring
- bronchitis
- health and safety
- epidemiology
Statistics from Altmetric.com
- MRI
- static magnetic fields
- static magnetic stray fields
- time-varying magnetic fields
- cognition
- exposure
- risk assessment
- electromagnetic fields
- occupational health practice
- exposure assessment
- statistics
- hygiene/occupational hygiene
- epidemiology
- retrospective exposure assessment
- neurobehavioural effects
- longitudinal studies
- exposure monitoring
- bronchitis
- health and safety
- epidemiology
What this paper adds
-
Moving in the stray fields of an MRI system can result in sensory symptoms (nausea, dizziness and a metallic taste) and previous experiments showed the possibility of temporary changes in neurobehavioral functioning (visual perception, visuomotor performance and working memory).
-
In this paper, we examine acute effects of head movements within a static magnetic stray field of an MRI system on several neurocognitive functions in the first study using a double-blind randomised cross-over design.
-
We showed that standardised head movements within a static magnetic stray field of a 7 T MRI system result in a temporarily decreased attention/concentration and visuospatial orientation, while other neurocognitive domains showed no difference compared with sham.
-
The impact of these neurobehavioural effects on employees and surgeons working with MRI and their patients is not yet clear, but these results show the importance of appropriate safety measures.
Introduction
The use of MRI scanners as a diagnostic instrument or to guide interventions increased rapidly since its introduction in the late 1970s, and this trend is expected to continue.1 For example, the amount of scans produced each year in hospitals throughout the Netherlands increased from 227 000 in 1998 to around 682 000 in 2008 (personal communication by K Schaap, 2011). Simultaneously, the applied intensity of the magnetic field increased from 0.04 Tesla (T) in the 1980s to 7 T and 11.7 T of the recently available ultra high field scanner systems.2–4 Nowadays, 3.0 T scanners are replacing 1.5 T scanners for intervention and routine clinical applications, while scanners of >7 T have started to appear in academic settings.
Scanning with higher field strengths improves imaging quality, reduces imaging time and increases the image quality of dynamic systems such as the circulatory system.1 To create an MRI image, three types of electromagnetic fields are required: a static magnetic, switched gradient magnetic field and a radiofrequency electromagnetic field. Of these, the static magnetic field (SMF) is always present, even when no actual imaging procedure is taking place. This is because most MRI systems are never ramped down since inoculation of the machine is very time demanding and expensive. The magnetic fields inside the magnet bore are completely homogenous; this in contrast to the spatially very heterogeneous fields surrounding the magnet bore that are often referred to as SMF. When individuals move through these heterogeneous stray fields, a change in gradient is brought about that induces a time-varying magnetic field (TVMF).

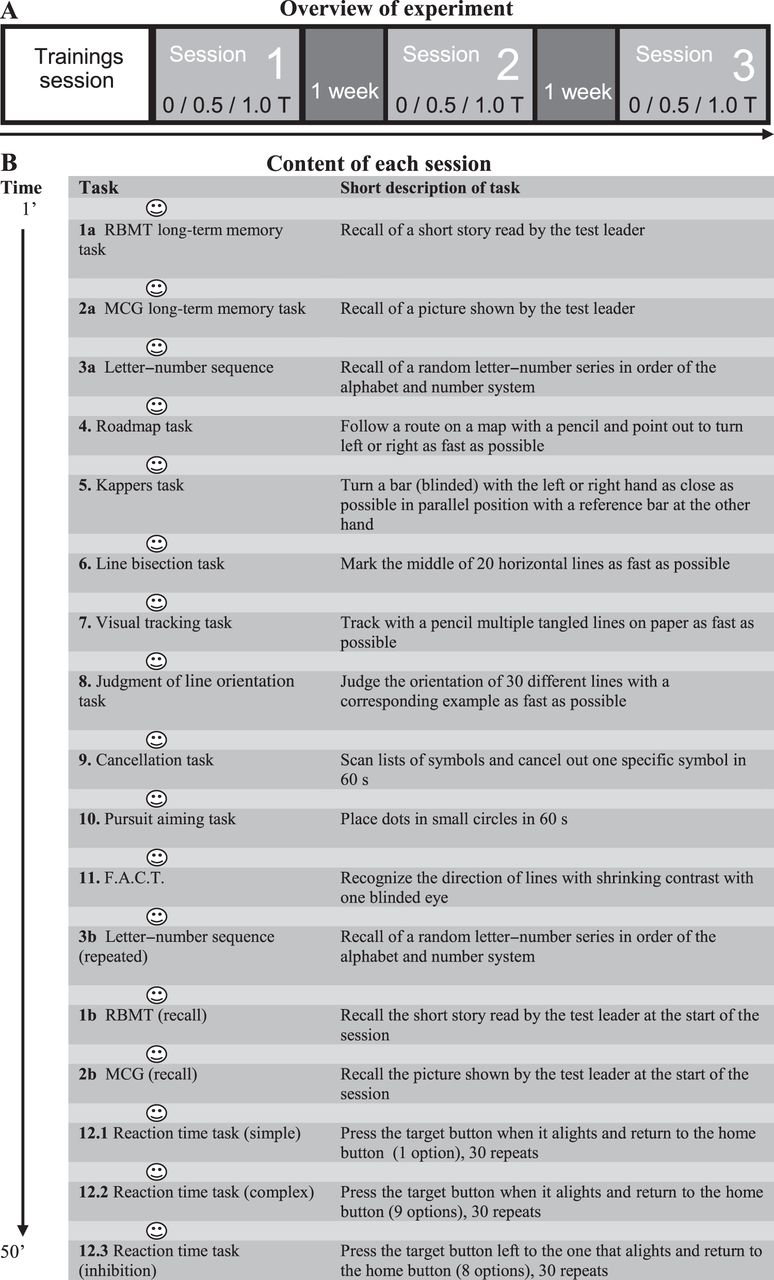
Set-up of the experiment (A) and specifications of the test battery per session (B). (A) Each subject underwent three test sessions with 1 week in between at the same time of the day. Exposure conditions were randomized over the subjects. The first session was preceded by a training session. (B) Design of a single test session. During approximately 50 min, 12 different cognitive tasks were performed each preceded by standardised head movements ( ), 10 movements in a vertical direction and 10 movements in a horizontal direction.
), 10 movements in a vertical direction and 10 movements in a horizontal direction.
The introduction of stronger MRI systems has resulted in increased exposure to SMF for both patients and personnel in healthcare, research and industry. To date, mainly safety and health concerns for patients have been evaluated, but possible consequences are particularly important for professionals including radiographers, radiologists, anaesthesiologists, nurses, cleaners and MRI engineers since they are repeatedly exposed to SMF and TVMF while working with or in the neighbourhood of MRI scanners. Employees moving in the stray fields surrounding these systems have reported symptoms like nausea, dizziness, fatigue, sleeplessness, concentration problems and a metallic taste.5–9 Beside such symptoms, even subtle temporary effects of exposure to electromagnetic fields might affect their behaviour and cognitive performance, which consequently could have implications for their own safety and that of their patients. Especially, the work of surgeons and personnel performing MRI-guided interventions and operations requires a high level of precision and performance.10–14
Previous experimental studies with volunteers found no neurocognitive effects from neither homogeneous SMF inside the magnet bore7 ,15 ,16 nor from TVMF alone.17 However, movement-induced TVMF in an SMF near a 1.5, 3.0 and 7 T MRI scanner was shown to have small but statistically significant reversible acute neurobehavioral effects on visual perception and visuomotor performance.18–20 In one of these, studies working memory was affected as well.19 It has been hypothesised that these effects probably arise due to induced electrical currents in the body that are generated during movement in an SMF.20 ,21
Given the above, there is an urgent need for more research on acute effects of movement-induced TVMF near MRI scanners. The aim of the present study was to characterise potential acute neurocognitive effects of exposure to TVMF within an SMF in a double-blind randomised crossover trial. For this purpose, a test battery has been composed that is sensitive to acute (temporal) changes in susceptible neurocognitive domains that are relevant for surgeons and other personnel in a working situation near MRI systems. In addition, domains were included that are associated to the reported symptoms of nausea and dizziness near MRI systems and domains that showed effects in earlier studies.
Methods
Subjects
Thirty-one healthy volunteers who signed an informed consent participated in the experiment. Most were students (N=24) from Utrecht University, recruited by flyers and advertisement on bulletin boards. Thirty subjects finished at least pre-university education, and one subject finished higher general secondary education. Of all volunteers, 10 were men and 21 were women with an average age of 23.8 (SD 6.4) years. Applied exclusion criteria were self-reported presence of MRI-incompatible elements in the body, history of neurological disease, serious vision deficiencies, use of medication (except for birth control), soft or hard drugs, excessive alcohol (>2 glasses per day) or coffee (>5 cups per day) and sensitivity to motion sickness in adulthood. Sensitivity for motion sickness was defined as a score higher than two on a four-point Likert scale ranging from one (not at all) to four (very often) for at least one of three types of symptoms. Eight subjects reported to have undergone an MRI but none of the subjects or experimenters had worked with MRI or had seen the test room before. A modest incentive gift voucher was given as expenses for every completed test session. The study was approved by the local medical ethics committee of the University Medical Center Utrecht (UMCU), the Netherlands.
Experimental design
A double-blind randomised crossover design was used in which each subject was tested for 1 hour on three occasions, conducted at the same time of day with 1 week between each session (see figure 1A). The sequences of exposure were balanced and assigned to each subject prior to the start of the experiment using a randomisation protocol.
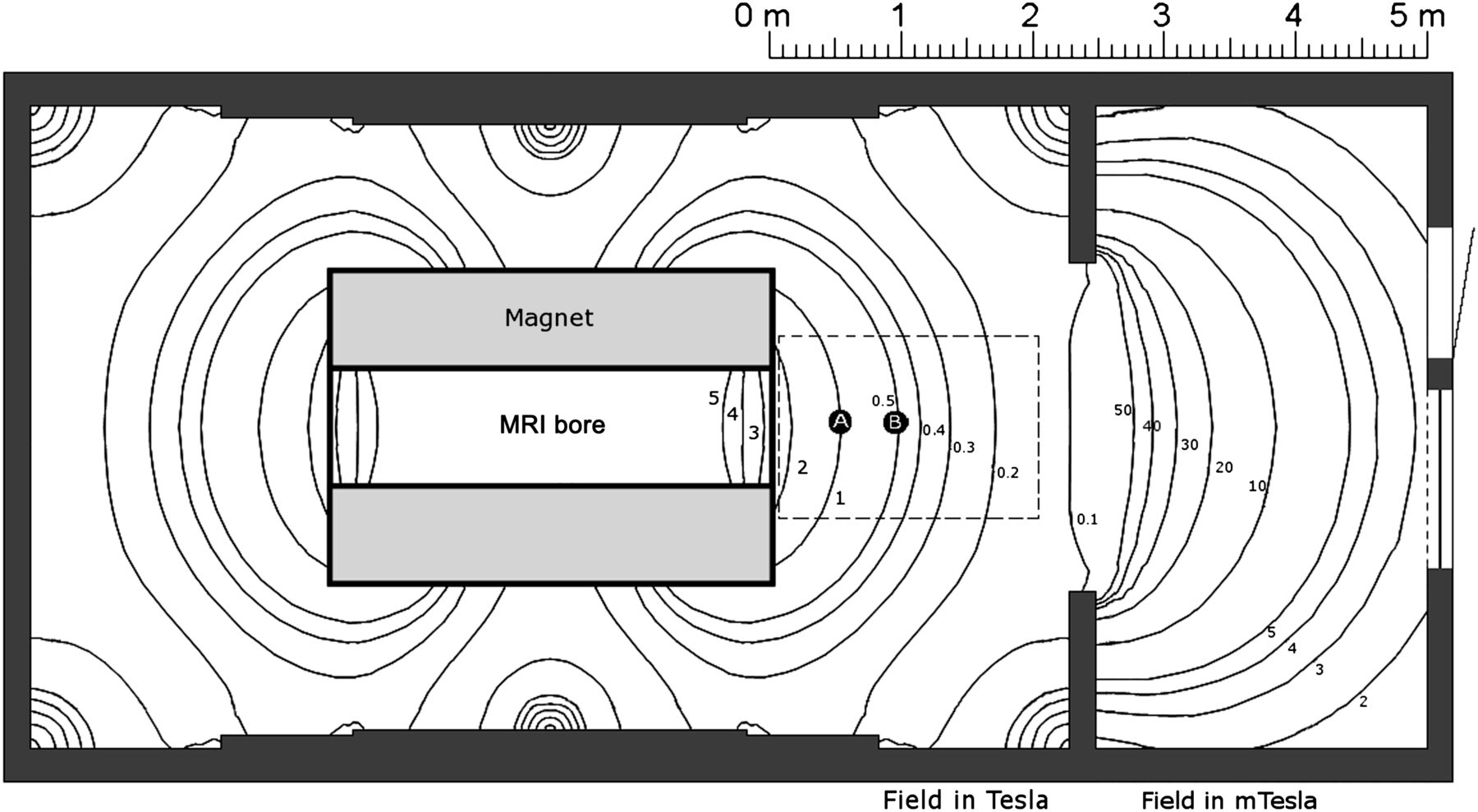
There were two active exposure conditions of 0.5 T (low) and 1.0 T (high) SMF (in the stray field of a passively shielded 7.0 T Philips Achieva research system located at University Medical Center Utecht) and an unexposed sham condition (<25 mT) in a separate room (see figure 2). The subject sat on a fixed chair, with their back towards the bore at, respectively, 47 and 86 cm for the 1.0 and 0.5 T condition. In addition to the SMF in the exposure conditions, subjects were exposed to TVMF induced by standardised head movements before each new neurobehavioral test in the test battery (see figure 1B). The head movements consisted of 10 movements in vertical and 10 in horizontal direction (covering an angle of 180° in 0.8 s), the start of each movement indicated by an auditory cue. The accompanying TVMF at head height in sitting position in the 0.5 (low) and 1.0 T (high) conditions were on average approximately 1200 and 2400 mT/s, respectively, as measured by a static magnetic field dosimeter (Magnetic Field Dosimeter; University of Queensland, Australia).22

Top view map of the 7 T MRI with calculated field lines of the static magnetic stray field as provided by Magnex Scientific Inc. Dots represent the positions of the subject for the exposure conditions within the tent. Position A represents the 1.0 T condition and position B the 0.5 T condition, respectively, 47 and 86 cm in front of the bore. The tent (interrupted line) was shifted when subject was in position B. The sham condition was in a room opposite to the scanner room (not shown in this figure).
Several measures were taken to ensure a double-blind experiment: subjects were tested inside a standardised tent (210×140×190 cm) to hide the exposure condition. In addition, in the sham condition, an audiotape playing the acoustic noise of an MRI system was used. The subject and trained experimenter were blind guided into one of the tents by the experiment coordinator (LvN).
To reduce a possible practice effect in neurocognitive test performance, the subjects completed a full test session prior to the first experimental session. Before each session, subjects were checked for metallic components and were asked to complete a questionnaire about current symptoms. A second questionnaire on (adverse) side effects and perception of the actual exposure condition was completed after each session.
Test battery
Neurocognitive domains were selected based on brain functions that are most relevant for surgeons and other medical professionals operating near MRI, for example, visual perception, motor performance as well as more general functions concerning attention, concentration and (working) memory (see figure 1B and supplementary material). In addition, domains related to the reported sensory symptoms of nausea and dizziness were included like spatial orientation23 and haptic perception.
Based on the results of a pilot test (data not shown), the test battery was composed of tasks that are relatively short (<4 min each), insensitive to ceiling effects and to influences of practice and level of intelligence. This was because the change in performance is expected to be subtle, acute and short-lived in educated and healthy individuals. For this reason, we also included the time needed to complete a task in addition to task performance per se. Above all, the test battery had to be compatible and safe for use in an MRI environment and for the different sessions, parallel versions of all tests were used.
Based on the results of previous studies,9 ,18 ,20 tests selected for visual perception were the Visual tracking task24 and a Visual acuity task (F.A.C.T.®). For integration of visual and motor performance, the Pursuit aiming task24 was included. To assess attention and concentration, we selected two tasks: the symbol cancellation task (Diller, Ben Yishay et al, 1974 in Lezak et al 27) and a reaction time task with a simple, complex and inhibition section.25 ,26 Beside reaction time, this task also measures visuomotor performance, motion time and disengagement time by registration of initiation-, release-, movement- and return times of the home- and target button. To measure the performance of memory (episodic learning), we used the Rivermead Behavioural Memory Test (RBMT) story recall for verbal memory (Wilson, Cockburn and Baddeley, 1989 in Lezak et al 27) and Medical College of Georgia (MCG) figure for non-verbal memory (Loring and Meador, 2003 in Lezak et al 27). For working memory, the short version of the WAIS III letter–number sequencing test (Wechsler, 1997 in Lezak et al 27) was administered twice throughout the test session by two different versions to check for a possible decrease in attention or motivation. To asses nausea- and dizziness-related functions, tests for visuospatial orientation were specified into different aspects of spatial orientation by the Judgement of line Orientation task for angular relation,28 the Roadmap task for left–right orientation (Money, 1976 in Lezak et al 27) and the line bisection task for spatial representation (Schenkenberg et al, 198027). To explore the tactile modality, haptic perception was tested by use of the Kappers task.29 (For a more detailed description of the tasks, see figure 1B and supplemental material).
Data analysis
Statistical analyses of interindividual and intraindividual differences in test performance in association with exposure were performed using mixed-effects models30 in SPSS V.16.0 (SPSS Inc.). The exposure conditions (0, 0.5 and 1.0 T) were entered as continuous exposure variable assuming linear exposure–effect associations. All analyses were adjusted for session number, gender and reported ‘ever experienced mild symptoms of motion sickness (see paragraph ‘subjects’). Random effects were modelled using heterogeneous compound symmetry that assumes similar correlation between residuals of the same subject but no correlation between different subjects.
The data and residuals from the Visual tracking task, Roadmap, Judgement of Line Orientation were log10 transformed to account for potential ceiling effects. F.A.C.T. data were also log10 transformed since the relationship between the steps is not linear,31 and the data of the RBMT story recall were converted into percentages to obtain a better normalised distribution. Statistical significance level was defined as p≤0.05.
Results
Of the 31 eligible subjects, one subject decided to withdraw from the study due to non-experimental-related reasons. In total, 30 subjects completed all three experimental sessions. An experimental session had an average duration of 51 (SD 6) min for each participant conducted at the same time of day ±52 (SD 48) min. The mean test scores and SDs for all tests in the three different exposure conditions are presented in table 1.
Average test performance and SDs for each neurobehavioural test in the 0 (sham), 0.5 (low) and 1.0 T (high) exposure condition (N=30)
Table 2 shows results of the main analyses using a continuous exposure model. With respect to the visual–motor domain and the interaction between the visual and motor domain as measured by the Visual tracking task, F.A.C.T. and Pursuit aiming task, no statistically significant effects of exposure were observed.
Estimated trends of neurobehavioural test performance per 100 mT using a continuous mixed effects model adjusted for session, gender and ever experienced mild motion sickness symptoms (N=30)
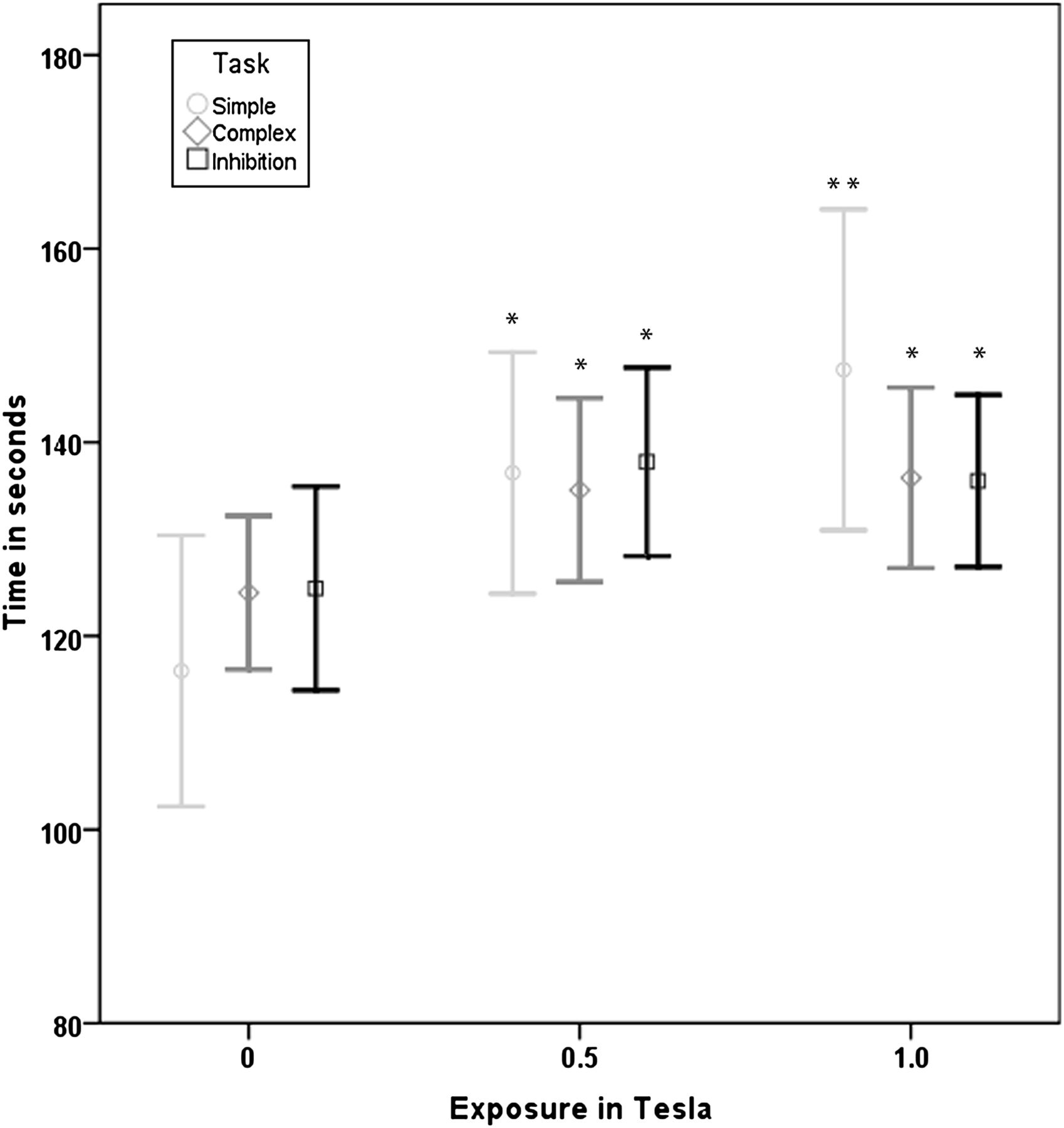
However, more general functions like attention and concentration, assessed by the reaction time task, showed a significant exposure–response association on motion time in the inhibition reaction time task (+5.0% per Tesla exposure p<0.05) reflected in increased times to move to the target button at higher exposure levels. In addition, disengagement time was negatively affected in the simple reaction time task (+21.1% per Tesla exposure p<0.001), complex reaction time task (+9.6% per Tesla exposure p<0.01) and inhibition reaction time task (+8.9% per Tesla exposure p<0.01), see figure 3. As such, increased exposure resulted in a longer time to release the target button in order to return to the starting position. The symbol cancellation task did not show a significant difference between the exposure conditions nor did the WAISS Letter–Number sequencing task testing working memory itself.
{kind=link}
{kind=link}
{kind=link}
Disengagement time (time needed to release target button) in milliseconds on the three different levels of the reaction time task in the three conditions. Error bars represent 95% CI of the mean. *Significant different from sham condition at p<0.05; **significant different from sham condition at p<0.001. n=30.
Episodic learning for verbal and nonverbal memory was not affected in the Rivermead Behavioural Memory Test story recall (RBMT) and Medial College of Georgia figure (MCG). However, the RBMT reached borderline statistical significance (p=0.07).
Domains that are related to nausea and dizziness, such as spatial orientation, showed an exposure–response association at the line bisection task indicating that the percentage deviation from the true middle of the line raised (+46.7% per Tesla exposure p=0.05) with increased exposure. The Judgement of Line Orientation and Roadmap task did not reveal an effect of exposure nor did the Kappers task demonstrate an effect of exposure on haptic perception.
Discussion
The main goal of this study was to investigate the acute effects movement-induced TVMF within a SMF from a 7 T MRI scanner on neurocognitive functioning. In the tested healthy population, we observed a significant exposure–response relationship, indicating a decrease in attention related to a reduced working memory and a decrease in visuospatial perception. Also in verbal memory functioning (story recall), a subtle decrease was seen, but this association did not reach statistical significance (p=0.07). These findings support the hypothesis that head movement in a spatially heterogeneous SMF up to one Tesla (T) does temporarily affect neurocognitive functioning. The current study design does not allow us to disentangle any effect to be associated only with SMF or TVMF or with the combination of both. In addition, the duration of any effect of motion-induced TVMF is unknown. Since it is not feasible to induce strong TVMF (by head movements) during the completion of a task, subjects performed head movements immediately before each single task. This implies that we would only pick up an effect of TVMF lasting longer than the duration of a single task (from 30 to 180 s). Our results show that effects due to TVMF would have to last for at least 90 s, that is, the longest task for which we found a statistically significant effect (reaction time task). This is longer than most other tasks except for the Kappers, memory and letter/number sequencing tasks which took up to 180 s and did not show significant effects of exposure.
The results as found in this study do not indicate a general effect of magnetic field exposure on neurocognitive functioning but show that rather specific target domains are affected. Analysis of the most fundamental neurocognitive functions of attention and concentration, like arousal, did not show an effect of exposure as tested by the symbol cancellation task and letter–number sequencing task. However, more specific aspects of attention and concentration showed that motion time was negatively affected in the inhibition reaction time task (+5.0% per Tesla exposure) meaning that participants moved slower from the home button to the target button during exposure compared with sham. Since we did not see a similar effect on the other two levels (simple and complex) of the reaction time tasks, this indicates that an increased motion time performance due to exposure might only occur when executing complex mental tasks. In the same reaction time task, disengagement time appeared to be increased on all three levels of the tasks when exposed to SMF and TVMF (ranging from +8.9 to +21.1% per Tesla exposure). This end point reflects the time a subject needs to release the target button before returning to the home button, meaning putting one trial to an end. Attentional disengagement and task demand are both processed by working memory resources and require the coordination of information under executive control.32 In this way, an increased disengagement time reflects a cognitive- or attention-related error caused by an increased working memory activity.33 This can be concluded from the intercept values (in table 2), where disengagement time increases with increasing level of the task because more working memory is required. However, we did not observe an effect of magnetic field intensity on disengagement time by task level. Both increased motion time and increased disengagement time of the reaction time task suggest that when a high cognitive working load is required in a magnetic field, less working memory is available to keep the same level of attention and concentration.
In addition to the reaction time task, verbal memory performance as reflected by the Rivermead Behavioural Memory Test story recall (RBMT) reached borderline statistical significance (p=0.07). However, non-verbal memory performance was not affected by magnetic field exposure as shown by the Medial College of Georgia figure (MCG). De Vocht and colleagues19 earlier found both verbal and non-verbal memory to be affected by magnetic field exposure.
More specific neurocognitive domains exploring visual performance (F.A.C.T.), motor performance (Visual tracking task) or an interaction between both (Pursuit aiming task) did not show an effect of exposure, in contrast to previous findings.18–20 In addition, the registered motion time in the reaction time task had a visuomotor component as well. We only found an effect at the most difficult level, indicating that the found effect is more related to working memory than to visuomotor performance.
Based on the questionnaire after each session, in the sham, low and high exposure condition, 4, 10 and 19 subjects, respectively, reported sensory symptoms. For example, in the highest exposure condition, a metallic taste (12 subjects) was most commonly reported followed by dizziness (six subjects), headache (five subjects) and nausea (one subject). Domains related to dizziness and nausea like visuospatial performance suggested that exposure to magnetic fields affects performance on the line bisection task (p=0.05). Subjects demonstrated a subtle but significant changed perception of the true middle of the line, corrected for handedness. In the sham condition, our subjects scored around the true middle of the line, while exposure to SMF and TVMF significantly increased deviation to the right (+46.7% per Tesla exposure). As described in the previous studies, normal subjects bisect lines slightly to the left (−1.6%) from the true centre of the line irrespective of hand preference.34 ,35 In this regard, subjects in our study performed above expectation in the sham condition. However, in the exposure conditions, deviation shifted in the opposite direction of those described for normal subjects above. The direction of deviation might be influenced by the position of the subject with respect to the magnetic field lines.36 de Vocht et al 20 used an adapted line bisection task with random orientated lines and found a trend for an increased deviation at exposure of 1.6 T and 300 mT/s. Other tasks examining visuospatial performance like the Judgement of Line Orientation and the Roadmap did not show an effect.
This study demonstrates that attention, concentration and visuospatial orientation are affected by exposure to MRI-related static and time varying magnetic fields. Alternatively, the effects on neurocognitive functioning could be influenced by a fluctuation in motivation or attentional span instead of an effect that can be attributed to the exposure conditions. However, we did not find a difference in performance for the WAIS-III Letter–number sequencing task when administered at the beginning versus later in the test battery in the sham condition.
de Vocht and colleagues18–20 showed in earlier studies an association between exposure to SMF and TVMF and a lowered visuomotor performance and visual perception. In these experiments, the F.A.C.T., Pursuit aiming and Visual tracking task were affected, while these tasks were not affected in our experiment. Although our results did not corroborate earlier findings on these specific tasks, the same domains of vision and more basal cognitive functions seemed to be affected by exposure in our experiment. Differences in experimental method between experiments complicate comparisons and could have contributed to the differences in results. For example, in the current experiment, exposure levels of the TVMF were estimated at least four times higher (300 compared with 1200 mT/s) due to faster head movements over a larger angle and in two directions. In addition, we used a double blind test design to prevent potential bias due to knowledge about the exposure condition. Furthermore, the previous experiments might have included more vulnerable groups, where we used a much younger and more homogeneous group of subjects and excluded those with a history of motion sickness. Therefore, it is conceivable that only high distinctive and sensitive tests for visuomotor performance and visual perception might have been able to reveal effects of exposure in this experiment.
Although we assumed in our main analysis a linear association between SMF exposure and test performance, we realise that neurocognitive functions do not necessary have to respond in this way since individual and clusters of neurons have diverse activation and saturation thresholds. Therefore, we also analysed the data by use of a categorical exposure model, showing that the results did not appreciably differ from the continuous analysis (data not shown). The number of exposure conditions was too limited to pursue more sophisticated non-linear exposure–response modelling.
Strengths of this study include a balanced double-blind randomised crossover design that eliminates errors since neurocognitive tests in healthy subjects are highly influenced by age, gender and educational level. In this design, individuals served as their own controls. We set out to perform a double-blind experiment by using similar tents, blind guiding of subjects and test leaders into the tents and use of MRI audio recordings in the sham condition. However, blinding was not perfect since four subjects reported that they could feel the magnetic fields because they had a splint behind their teeth that was in some cases made of a weak paramagnetic material, undetected by the metal detector. Post-hoc sensitivity analyses excluding these subjects did not show notably different results. Based on the post-session questionnaires, perceived ‘exposure’ or ‘no exposure’ by the remaining 26 subjects in the sham, 0.5 and 1.0 Tesla exposure condition was correct in 69%, 38% and 65% of the sessions, respectively. Test leaders were asked to indicate ‘sham’, ‘low’ or ‘high’ exposure and had 93%, 62% and 42% correct predictions in the 0, 0.5 and 1.0 Tesla conditions, respectively. However, these rates for test leaders are more difficult to interpret since a device they needed for a test at the very end of the session contained some magnetic material, which could reveal the exposure condition. Thus, blinding of the experiment in further studies can probably be improved by refining the setup and specifically enquire about magnetic splints prior to enrolment.
Overall, the results of this study show that neurocognitive functioning is acutely affected when exposed to strong TVMF due to head movements within an SMF. Domains that were affected include attention/concentration and visuospatial orientation and possibly long-term memory. However, the exact implications and mechanisms of these subtle acute neurocognitive effects in practical settings remain unclear. In future research, it will be of interest to focus more on different neurocognitive domains under high working memory load and to differentiate between effects raised by either the SMF or the time-varying magnetic fields or the combination of both. A better understanding of the mechanisms causing acute effects can be used as a basis for design of relevant control measures to lower exposure and reduce the occurrence of neurobehavioral effects for individuals employed under these conditions.
Acknowledgments
K Schaap, MSc, S I M Bongers, MSc, and J J Baars are acknowledged for collecting data as test leaders. Dr Ir S A Uzunbajakau is thanked for constructing the button box. Professor P M Luijten, UMCU, provided the MRI room. The study was only possible due to the dedication of all subjects participating in the experiment.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Files in this Data Supplement:
- Data supplement 1 - Online supplemental material
Press release
Files in this Data Supplement:
Footnotes
-
Funding This work was supported by The Netherlands Organisation for Health Research (ZonMW) within the program Electromagnetic Fields and Health Research under grant numbers 85100001 and 85800001.
-
Competing interests None.
-
Ethics approval The study was approved by the local medical ethics committee (study number: 09-310) of University Medical Center Utrecht (UMCU), the Netherlands. Medical ethics committee of University Medical Center Utrecht (UMCU), the Netherlands (study number: 09-310).
-
Provenance and peer review Not commissioned; externally peer reviewed.
-
Data sharing statement All authors had full access to all data and can take responsibility for the integrity of the data and the accuracy of the data analysis.